Article Text

Abstract
Introduction Young adults fare worse than younger adolescents or older adults on a broad range of health indicators. Those with a chronic illness such as renal failure are a particularly vulnerable group, who experience poor outcomes compared with both children and older adults. Understanding how being in receipt of renal replacement therapy (RRT) affects the lives of young adults might help us to better prepare and support these individuals for and on RRT, and improve outcomes. This study aimed to synthesise research describing young adults’ experiences of the psychosocial impact of kidney failure and RRT.
Design A systematic literature review identified qualitative research reporting the perspectives of people aged 16–30 years receiving RRT on the psychosocial impact of renal failure. Electronic databases (including Medline/EMBASE/PsycINFO/ASSIA) were searched to November 2017 for full-text papers. The transparency of reporting of each study was assessed using the Consolidated Criteria for Reporting Qualitative Health Research (COREQ) framework. Quality was assessed using the Critical Appraisal Skills Programme qualitative checklist. An inductive thematic synthesis was undertaken.
Participants Seven studies from five different countries were included, comprising 123 young adults receiving RRT.
Results Comprehensiveness of reporting was variable: studies reported 9–22 of the 32 COREQ-checklist items.
Three global themes about the impact of kidney failure on young adults were identified: (1) difference desiring normality, (2) thwarted or moderated dreams and ambitions, and (3) uncertainty and liminality. These reflected five organising themes: (1) physical appearance and body image, (2) activity and participation, (3) educational disruption and underachievement, (4) career ambitions and employment difficulties, and (5) social isolation and intimate relationships.
Conclusions Across different countries and different healthcare settings, young adults on RRT experience difference and liminality, even after transplantation. Tailored social and psychological support is required to allow young adults to experience wellness while in receipt of RRT, and not have life on hold.
- psychosocial impact
- qualitative research
- renal replacement therapy
- thematic synthesis
- young adults
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first attempt to synthesise the existing qualitative literature that investigates the impact of renal failure on young adults.
The number of participants included was large and multinational.
The emergent themes were represented across the included studies, supporting the validity of the findings.
The quality of reporting of the included studies was variable, and the quality of the research undertaken was sometimes difficult to assess due to the poor standard of reporting.
Introduction
Young adults fare worse than younger adolescents or older adults on a broad range of health indicators.1–3 Those with a chronic illness such as renal failure are a particularly vulnerable group.4 Most young adults on renal replacement therapy (RRT) have a kidney transplant: in the UK 73% of people aged 18–24 years on RRT have a functioning transplant.5 Young adults with a transplant have an increased risk of transplant graft failure compared with both children and older adults.6 7 Understanding how renal failure affects the mental health, education, career ambitions, social lives and relationships of young adults might help us to better prepare and support these individuals for and on RRT, and improve outcomes.
Qualitative research can provide valuable insight into the impact of disease on an individual’s life and lived experience, but single qualitative studies are often from one geographical area or healthcare centre, and often focus on a single aspect of experience rather than a spectrum. Thematic syntheses combine the findings from individual studies, to generate a rich, holistic, more complete understanding of the phenomena being investigated8 and generate new findings.
This thematic synthesis aimed to identify and synthesise qualitative research describing how kidney failure impacts on the lives of young adults, to identify areas which might require research and clinical attention, to ultimately improve patient outcomes. A systematic review and meta-analysis of the quantitative research on the psychosocial impact of RRT on young adults was undertaken alongside this qualitative synthesis, the results of which are reported elsewhere.9 This paper presents the findings of the qualitative literature synthesis, which might help us to explain the quantitative findings, adding the patient voice and rich context to numerical results.10
Methods
We followed the Enhancing Transparency in Reporting the Synthesis of Qualitative Research framework.11
Search strategy
A sensitive search strategy was applied to nine databases (Medline, EMBASE, PsycINFO, ASSIA, CINAHL, Web of Science, Scopus, Open Grey and Cochrane Library). The full search strategy for the Medline, EMBASE and PsycINFO databases is provided as online supplementary material. We ran our first search in July 2015, and a final search in November 2017, for the latter limiting results to those from the last year only. We used EndNote to identify duplicate studies. AH screened the titles and abstracts of all the citations resulting from the search to identify studies fulfilling the inclusion criteria. PB screened the titles and abstracts of all the citations resulting from the final search. RC screened a random sample of 1000 titles and abstracts to ensure consistency. Any disagreements were resolved by discussion. When the literature database did not already provide a translated title and abstract, Google Translate was used to screen non-English abstracts: no relevant non-English articles were identified.
Supplementary file 1
Study selection
We included qualitative studies of young adults (aged 16–30 years) on RRT (dialysis and transplants) that explored participants’ perspectives on and experiences of the impact of renal failure on their lives (including education, employment, social life, relationships and psychological health). Studies were included if all or the majority (>50%) of participants were in this range. When studies included participants aged <16 or >30 years, quotes from those participants were excluded from analysis. There is no consensus definition for young adulthood, and we chose a priori a wider age range to ensure that we did not miss any important publications. Globally, the legal age at which individuals enter adulthood varies between 16 and 21, and there is generally a gradual transition to full adult status. All included qualitative articles were double-checked by PB to ensure they met the inclusion criteria. The references of identified articles were screened to identify any additional papers. One study12 analysed interviews with young people who had chronic kidney disease as well as individuals on dialysis. The lead author was contacted to request access to the original transcripts of those patients on dialysis, but the study’s ethical approval did not allow transcripts to be shared. A decision was made to include this study, extracting the findings but excluding the quotes from individuals not on RRT. This decision was made as the paper was the highest quality study identified, the majority of the illustrative quotes were from individuals on dialysis (30/39 quotes presented in table), and the themes identified were deemed relevant to our study, and overlapped with findings from other included studies.
We assessed the transparency of reporting of each study using the Consolidated Criteria for Reporting Qualitative Health Research (COREQ) framework.13 The quality of the included studies was assessed using the Critical Appraisal Skills Programme Qualitative Research Checklist.14 PB assessed all seven studies. RC and AH independently assessed two papers and any differences were discussed as a group. No study with relevant data was excluded from the synthesis.
Thematic synthesis
Inductive thematic synthesis was undertaken with reference to the method outlined by Thomas and Harden.15 The text in the results sections of each article was extracted electronically and entered verbatim into NVivo V.10 qualitative software16 for analysis. Data were analysed inductively. Line-by-line coding was undertaken, assigning sections of text descriptive labels. Codes were then grouped on the basis of shared properties to create concepts, which were grouped into themes. Subsequent studies were coded into pre-existing concepts, and new concepts were created when deemed necessary. Thus, themes were identified and analytic induction used to identify any patterns arising. Relationships between themes were identified and explored. PB and AOS independently coded all the papers. PB and AOS discussed their findings and any coding discrepancies to maximise rigour and reliability.
Results
We included seven studies (figure 1), from five different countries, comprising 123 young adults receiving RRT. All studies were published in English; two were undertaken in countries in which English was not the primary language. All studies used in-depth semistructured interviews to collect data, with some also using focus groups, diaries and questionnaires (table 1).
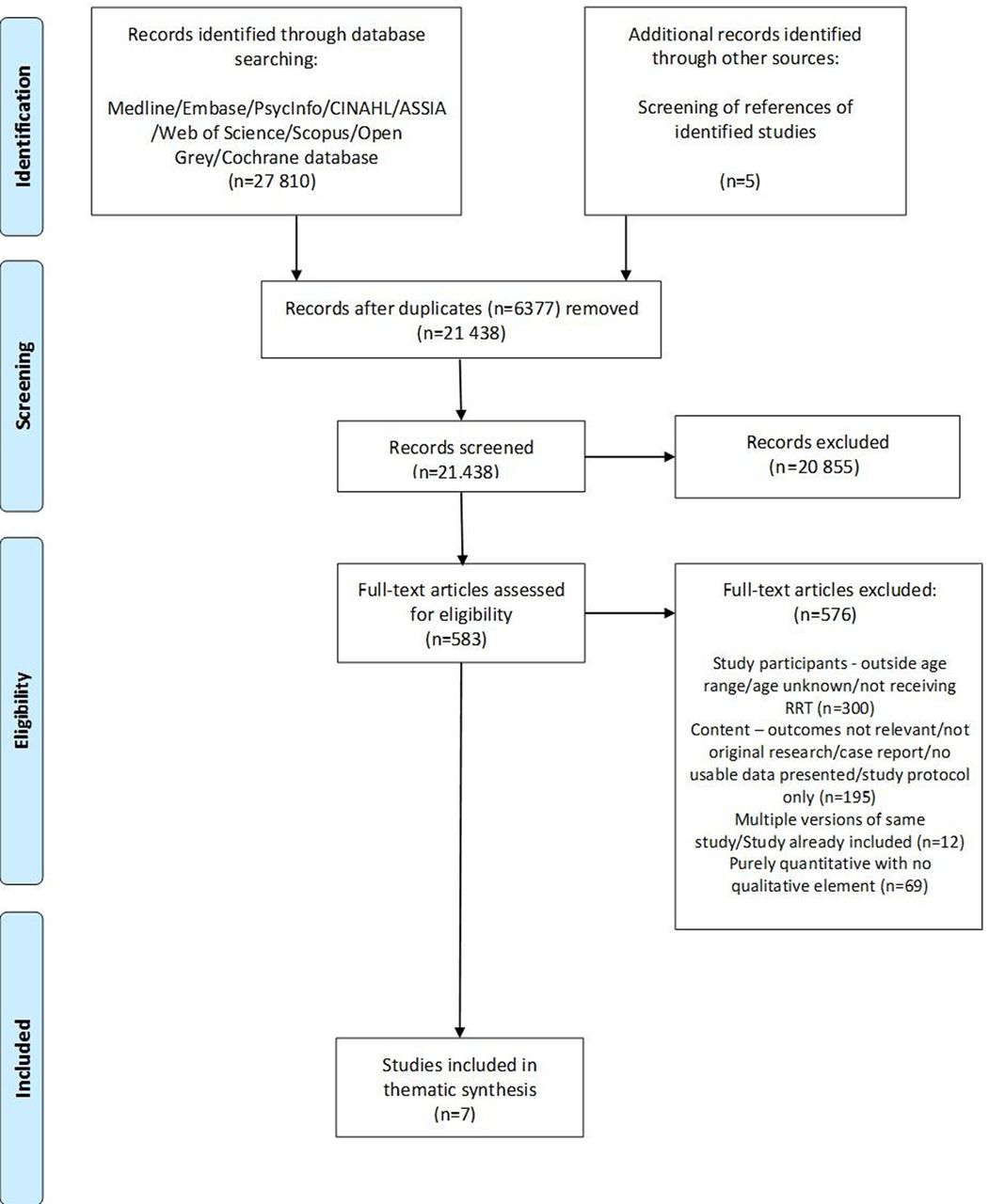
Systematic search results for studies. RRT, renal replacement therapy.
Study characteristics
Comprehensiveness of reporting was variable: studies reported between 9 and 22 of the 32 COREQ-checklist items (table 2). Only four studies reported that theoretical data saturation had been reached. One study reported that this had been reached after only interviewing five participants17 which is unexpected with such a small sample. Only one study was accompanied by an interview topic guide.12 One paper presented the findings from a mixed-methods study, but details regarding the qualitative analysis were lacking.18 Two studies suggested differences in the experiences of young adults who developed renal failure as children compared with those who were diagnosed as young adults.12 19 The quality of the studies was sometimes difficult to assess due to poor reporting: findings are presented in table 3.
Comprehensiveness of reporting
Quality assessment of included papers
Themes
Three global themes about the psychosocial impact of renal failure on young adults were identified: (1) difference desiring normality, (2) thwarted or moderated dreams and ambitions, and (3) uncertainty and liminality. These reflected five organising themes: (1) physical appearance and body image, (2) activity and participation, (3) educational disruption and underachievement, (4) career ambitions and employment difficulties, and (5) social isolation and intimate relationships (figure 2).

{kind=link}
{kind=link}
Thematic schema.
Results are now presented under the three global themes with reference to the organising themes. Participant quotes illustrate themes. When reported in the primary research paper the characteristics of the person to whom the quote belongs are provided after the quote: Key: Age (in years), Sex (M=male; F=female), RRT (HD=haemodialysis; PD=peritoneal dialysis; Tx=transplant).
Difference desiring normality
Study participants reported that they felt different to their peers; difference appeared to be perceived and reported as negative by all participants, who expressed strong desires to be ‘normal’. Difference was primarily characterised by differences in physical appearance, and by differences in ability to participate in activities. While young adults who had developed renal disease in childhood reported desiring a perceived normality, young adults who developed renal failure in young adulthood also described ‘an unbearable loss’ of a previously experienced normality.12
Going from living a normal life, from what I knew, to being in hospital most of the time…I don’t like it. (18,M,HD)12 [Key: Age, Sex, RRT (HD=haemodialysis; PD=peritoneal dialysis; Tx=transplant)]
To look at me just like before, when I did not have the illness. Treat me normally. (18,M,HD)20
Physical appearance and body image
Participants across studies reported problems with being physically different to peers, due to surgical interventions (eg, peritoneal dialysis catheters), medication (eg, weight gain) and chronic illness (eg, short stature).
It can make you a bit like self-conscious if you have the tube. You worry that people can see it through your clothes or the scars… (16,F,PD)12
These differences in physical appearance were often described using terminology suggesting a sense of dehumanisation and mechanisation, such as looking ‘like a robot’ and feeling like a ‘wood block.’ 21
Many participants described finding that to some extent transplantation provided the physical normality they’d desired, resulting in:
[a] face without swelling, and no more being hairy 21
However, others experienced further physical changes following transplantation:
I’m covered in scars… my face is really fat… I just hate looking at myself, I think I look like a freak. (28,F,Tx)22
…prednisone [steroids] makes me eat a lot and gain weight…17
Activity and participation
As well as physical differences preventing individuals from feeling ‘normal’, study participants reported barriers to participating in everyday activities. Being able to participate in sport22 and education were seen as particularly vital to being normal:
While being on dialysis, I couldn’t soak in water. When I went to a water park after the transplant, it was quite wonderful as I didn’t need to attach a bandage to my body anymore, could get along with friends, and was not different from others. (17,F,Tx)20
The local education… wanted me to go to a special school, for people with learning difficulties… My Mum and Dad were like, ‘No, he hasn’t got a physical disability, it’s a medical condition, we want him to go to a normal school like all his friends and be treated normally. (27,M,HD) 18
Young adults tried to engage in the same activities as their peers, by denying their health problems, lying about hospital appointments and missing medication when socialising:
I’d lie [about missing school for clinic]. I’d say I went to visit my girlfriend you know. You don’t say ‘I went to the hospital,’ …It’s stupid. I just say I went to visit someone, or I didn’t feel like coming.16
I didn’t take (my tablets) on time, ever… It was an embarrassment… I was going out with friends, they were drinking, smoking, doing things and there was me with a tablet box. (26,F,Tx)21
A few participants described feeling a sense of normality when they had individually accepted their health problems, and had successfully developed an identity separate to their illness:
[I started] to build more of an identity for myself that wasn’t so centred on my illness and it was more like…I do have an illness yet I still want to establish that I’m a normal teenager like everyone else. (19,M,HD)12
Thwarted or moderated dreams and ambitions
Many participants described a sense of underachievement and lost opportunities, related to education, employment and intimate relationships.
Educational disruption and underachievement
Young adults reported that renal failure negatively impacted on their educational achievement whatever their educational level when starting RRT:
Cos I’d started haemo… my [high school exam] results were really quite bad… I was really, really upset… I went on to University… but I’d still not done English and Maths. (24,F,Tx)19
Some participants directly attributed educational underachievement to their disease and treatment, while others felt personally responsible, reporting that they had allowed their illness to affect their achievements:
When everyone was graduating year 12, I’m thinking oh, that could have been me if I didn’t let everything get in the way. (18,F,HD)12
Many participants, despite feeling they had underachieved, had often still succeeded in gaining significant qualifications:
For the whole of my Finals year I was on dialysis. It was quite a struggle, I would have got a 1st, but I got a 2(i). (28,M,HD)19
Career ambitions and employment difficulties
Participants moderated their career expectations with many reporting that they were able to find employment, but sometimes in jobs which were not what they’d hoped for:
I can get a job, like in a shop, but it doesn’t really do much for me. (29,M,Tx)19
One participant powerfully described his gradual realisation of the impact of renal failure on his career ambitions12:
Interview quote: It’s always been a military career for me and nothing else, and the thing is that this kidney puts that whole dream and that whole lifestyle at risk, like even if I get this [transplant], there’s thousands of really strong men and nothing wrong with them at all that go for that and they don’t get it, so you know like I have to work my arse off ten times harder and there’s still no guarantee that I’m going to get it, and that’s like the only career I’ve ever wanted, I can’t think of myself doing anything else. I feel like that, this seems to have taken a lot of things away. (16,M,PD)12
Later journal entry: Today we went to hospital for some transplant education. It involved a detailed description of the procedure and medication I would go through. I was feeling good about it when a sudden realisation hit me. Since I would be on anti-rejection drugs to keep my immune system down so it would not attack the new kidney, I would be more likely to get disease and sick which makes a career in the army a not so likely future. I mean healthy normal men don’t always get in and I’d be expected to fight in environments w[h]ere disease like dysentery and malaria are common. As if the fact that I’ve had renal failure didn’t screw up my chances enough. (16,M,PD) (journal)12
Disclosure of their renal disease to employers was perceived, and had been experienced by some, as a challenge, the timing of which was thought to be crucial:
If you [kidney patient] put your CV in and you [employer] get a ‘normal’ CV in; ‘I can work full time, there’s nothing wrong with me.’ Well, who would you choose? (Age not provided,F,Tx)17
My attitude… is to demonstrate… that I am more than capable of doing whatever it is that they want me to do. Once that has been established I tell them. I delay disclosure… that is the tactic. (28,M,HD)18
Social isolation and intimate relationships
Participants described experiencing social isolation from peers as a result of their renal disease. Sometimes this was associated with self-imposed isolation due to a dislike of their physical appearance (see ‘Physical appearance and body image’):
(Transplantation) made me…huge basically…I didn’t go out for…about 3 months…‘cos I felt like everyone was looking at me. (19,F,Tx)22
Some participants reported experiencing name-calling17 and bullying by peers because of their physical difference.21
Sometimes social isolation resulted from feeling physically unwell or due to needing to dialyse:
…you’re so distanced from your friends, like they’re off enjoying being eighteen, going to parties and everything, and I’m here stuck doing dialysis. (18,F,HD)12
Renal failure was described by young adults as having a particularly significant impact on their confidence in pursuing, and ability to establish and maintain intimate relationships. Young adults were concerned with finding a partner who would accept their need for RRT:
With my future, I’m mostly worried about relationships. Will I ever meet a guy who’ll be there for me no matter what? Will he care if I’m still doing dialysis? (18,F,HD)12
Participants in several studies perceived rejection by a partner as being because of their renal disease.17 22 Some participants used the internet to find partners, and ‘avoided the kind of pain incurred by more ‘personal’ rejection’.22
The themes of fertility and parenthood were key for older participants. There were multiple concerns, regarding fertility, heritable renal disease, the safety of pregnancy and the impact of renal disease on the ability to be a long-living and active parent:
We’d love kids… But, do you pass the problem on… then die half-way through as well? (27,M,Tx)22
Uncertainty and liminality
The lives of the young adults appeared to be characterised by perpetual uncertainty. Participants across the studies expressed feelings suggestive of a sense of liminality related to their renal disease, that is, of experiencing periods of ‘middle ground’ or time spent ‘treading water’ before the final goal of receiving a transplant. During these liminal periods, participants described putting life ‘on hold’:
One participant ‘cut his girlfriend off’ while on dialysis.22 Others on dialysis decided to wait until they ‘got a transplant’ to seek a partner22:
(I thought) I’m just going to… be on dialysis for a little while, have a transplant, then I can ‘move on’ (find a partner), because everything’s easier once you’ve had a transplant. (28,M,Tx)22
Participants described ‘being shunted back and forth between wellness and illness, with intense periods of ill health, followed by variable periods of relative stability, sometimes lengthy, with a successful transplant.’19 Young adults reported that periods of stability felt precarious and were often disrupted:
I had the dialysis problems at the wrong time…I’d just started (college) I thought I got them all sorted, then all re-occurred…so I had to stop the course. (29,M,Tx)19
For most participants, the liminal phase described time on dialysis before transplantation. However, the sense of finally having reached the ‘end goal’ of transplantation was often not sustained, as participants began to recognise that they were still different, and still had to manage restrictions in diet, medication and activities.21
Uncertainty was felt regarding all aspects of their lives, not just physical health, and included concerns regarding future employment, relationships and parenthood (see other organising themes).
Discussion
Young adults reported that renal failure impacted on their ambitions and life goals, and their capacity and opportunities to achieve them. RRT impacted on their developing personal identity by affecting their education, career ambitions, employment capabilities, social activities and personal relationships. They described a sense of difference and uncertainty, both of which were intertwined with a sense of social isolation.
In qualitative syntheses of research with older adults,23 24 participants have described RRT affecting their personal identity, as well as impacting on existing relationships with spouses/partners and children.23 24 This contrasts with our findings in young adults who describe renal failure as impacting on the development of their identity and their capacity to form relationships, and gain employment. The concerns of younger adults specifically relate to establishing key aspects of their lives, rather than managing the impact on an established life.
Liminality
The concept of liminality, developed by anthropologist van Gennep in his work on rites of passage,25 describes a state of ‘being inbetween’ pre and post ‘ritual’ states. Turner described liminality as a space in which individuals are ‘neither one thing nor another or maybe both’,26 and a transitional intervening period between ‘two relatively fixed or stable conditions’.26
The emerging adults in this study were already in a liminal state, between childhood and older/full adulthood. In addition, participants described being in a liminal state with respect to their renal disease, which in many ways prolonged the liminal phase they were already experiencing as a young adult as they put life ‘on hold’. Liminality was particularly experienced on dialysis, while participants awaited transplantation. This has previously been described in the renal literature,27 28 including the experience of transplantation not always delivering the desired/expected normality of wellness, and so in many ways continuing the liminal state.27
A recent quantitative systematic review and meta-analyses found that compared with healthy peers, young adults with transplants had lower quality of life.9 Our thematic synthesis suggested possible reasons for this, including the effects of transplant medications on appearance and ongoing restrictions in diet, medication and activities. The poor quality of life is also likely to be explained by the persistent sense of liminality, and experience of transplantation as not the ‘normal life’ that was anticipated pretransplantation.
This thematic synthesis found that young people had to moderate career expectations due to their disease, resulting in a mismatch between the jobs they wanted and those they were offered. Participants also reported difficulties disclosing their disease to employers, with a perceived impact on the likelihood of and security of employment. Many individual quantitative studies have reported that young adults on RRT are more likely to be unemployed9 18 29–32; often despite education levels comparable to their healthy peers9 29 32, these qualitative findings highlight possible reasons for this.
Numerous quantitative studies have reported that young adults on RRT are less likely to be married or to have a long-term partner.9 30 33 34 The thematic synthesis found that young adults reported that their renal disease had an impact on their confidence in pursuing, and ability to establish and maintain intimate relationships. Young adults reported concerns finding a partner who would accept their need for RRT, and many reported rejection as a result of their renal failure. Concerns regarding fertility, heritable disease and parenthood were also reported as impacting on relationships. The sense of difference identified in the synthesis is likely to both cause and result from the described differences in employment, intimate relationships and social isolation.
Clinical implications and future research
Psychosocial outcomes in patients on RRT have been identified by older adult patients as a priority for future research.35 36 At the moment, the research priorities of young adults are being investigated as part of the SONG-Kids priority setting work, which includes ‘children aged up to 21 years’.37 There is a need for specific research into the priorities of young adults.
Mental health appeared to have been underinvestigated in the included qualitative studies: two studies reported that two young adults had reported feeling suicidal12 17 but this was not described further. Some participants described feelings of hopelessness12 and body image concerns. Formal research into mental health problems in young adults with renal disease is required.
A number of clinical interventions could be considered to better support young adults on RRT, who have unique needs associated with the development of personal identity and achieving life aims. The development of young adult clinics (including individuals diagnosed in young adulthood as well as those transitioning from paediatric care) may allow support to be tailored to these needs. The inclusion of social workers, citizens advice volunteers, youth workers and psychologists in clinic, alongside CV-writing/interview skills workshops, and an area for socialising has been modelled in a UK centre.38 This model may be suitable for larger centres but a greater understanding is also needed of optimal models for smaller centres; providing this multidisciplinary support across conditions/disciplines for young adults with chronic illness could be considered.
Help with managing expectations of transplantation, and support to not put life ‘on hold’ while waiting is important. Young people need to be prepared for the reality of transplantation, which includes expectations of improved health, but with an ongoing treatment ‘burden’, possible complications and medication side effects. A mindfulness-based intervention has been reported as a possible way of helping people with chronic disease to ‘experience wellness within illness’.39
Social media, online resources and dating apps can support the development of social networks, especially for those with visible signs of RRT/body image issues who want to establish a relationship before meeting in person. Online communities have been found to be helpful in allowing young adults with cystic fibrosis to build an identity and sense of self, and have been shown to help develop a social community and sociability that extends beyond illness.40
Strengths and limitations
To our knowledge, this is the first attempt to synthesise the existing qualitative literature that investigates the impact of renal failure on young adults. The systematic review and synthesis were rigorous. While the number of included studies was small, highlighting young adults as an under-researched group, the number of participants included was large and multinational. The emergent themes were represented across the included studies, supporting the validity of the findings.
There were a few limitations: (1) the quality of the included studies was variable, and the quality of the research undertaken was sometimes difficult to assess due to the poor standard of reporting; (2) only one study published an interview topic guide, important themes may not have emerged due to limited questioning and (3) only two of the included studies explicitly reported the cultural or ethnic background of study participants12 18 and all studies were from high-income countries except for one.20 Findings may therefore not be transferable to individuals from ethnic minority groups or to different healthcare settings.
Conclusions
This thematic synthesis enhances our understanding of the experiences of young adults with renal failure. These results will help clinical teams to better support young adult patients and better address their holistic and complex needs. Findings will also help research teams focus on areas of particular importance to young adults.
Acknowledgments
This work was presented as an oral presentation at the 18th Congress of the European Society for Organ Transplantation (ESOT) at Barcelona in September 2017.
We would like to thank Penny Whiting for help in planning this review. We thank Dee Knipe, Mairead Murphy and Penny Whiting for their help with creating and managing a database for references. We acknowledge Catherine Borwick, specialist librarian, for assistance with the search strategy.
References
Footnotes
Contributors Research idea and study design: AJH, PKB, AO-S; data acquisition: AJH, RLC; assessment of reporting and quality: PKB, AJH, RLC; thematic synthesis: PKB, AO-S; data interpretation: PKB, AJH, RLC, FJC, YB-S, CDI, AO-S; supervision or mentorship: AO-S, YB-S, FJC, CDI. Each author contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved. PKB takes responsibility that this study has been reported honestly, accurately and transparently that no important aspects of the study have been omitted, and that any discrepancies from the study as planned (and if relevant, registered) have been explained.
Funding This study was funded by Kidney Research UK and Kidney Care UK.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.