Article Text

Abstract
Objective To assess the efficacy of an interactive smoking cessation decision-aid application (pp) compared with a smoking cessation static information app on continuous abstinence.
Design Automated double-blind randomised controlled trial with 6 months follow-up (2014–2015).
Setting Smartphone-based.
Participants 684 participants (daily smokers of cigarettes, 18 years old or over) recruited passively from app stores in the USA, Australia, UK and Singapore, and randomised to one of two sub-apps.
Intervention(s) Behavioural, decision-aid, smartphone application.
Main outcome(s) Continuous abstinence at 10 days, 1 month, 3 months and 6 months.
Results Smokers who received the decision-aid app were more likely to be continuously abstinent at 1 month compared with the information-only app (28.5% vs 16.9%; relative risk (RR) 1.68; 95% CI 1.25 to 2.28). The effect was sustained at 3 months (23.8% vs 10.2%; RR 2.08; 95% CI 1.38 to 3.18) and 6 months (10.2% vs 4.8%; RR 2.02; 95% CI 1.08 to 3.81). Participants receiving the decision-aid app were also more likely to have made an informed choice (31.9% vs 19.6%) and have lower decisional conflict (19.5% vs 3.9%).
Conclusion A smartphone decision-aid app with support features significantly increased smoking cessation and informed choice. With an increasing number of smokers attempting to quit, unassisted evidence-based decision-aid apps can provide an effective and user-friendly option to many who are making quit decisions without healthcare professionals.
Trial registration number ACTRN12613000833763.
- decision-aid
- smoking cessation
- smartphone
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first fully powered efficacy trial of a smoking cessation decision-aid application (app).
The design deliberately reflects the real-world setting recruiting through app stores.
It compares ‘state-of-the-art’ decision-aid design and support with passive information-only apps.
The trial was a novel fully automated design across four countries.
The decision-aid with support app significantly improved continuous abstinence at 6 months compared with information-only app.
Introduction
Just over one-fifth of the world’s adult population continues to smoke despite significant declines in smoking rates over the past decades.1 Smoking is responsible for the deaths of around 6 million people per year and costs the global economy around US$500 billion annually.1
Smoking cessation programmes are accessible to only 15% of the population globally2 despite more people attempting to quit. Approximately two-thirds of smokers in the USA attempted to quit in 2014,3 11% of male Chinese smokers mainly aged 15–24 years attempted to quit4 and a range of tobacco-control policies have been increasing quit attempts in low-income and middle-income countries.5 We also know that most quit attempts are likely to be unassisted6 and that the reasons for this may relate to personal and societal values of independence and autonomy which influence smokers’ beliefs and decisions about quitting.7
Mobile phone interventions have become a new but effective way to help smokers quit. A recently updated Cochrane review8 includes 12 studies, showing that these, mainly text message-based interventions, significantly improved continuous abstinence at 6 months compared with control9 interventions of information only. The authors also remarked on the lack of research on smartphone applications (apps) despite the plethora of these available to the public. As we have previously shown, a smartphone app was able to reach 1751 smokers in the USA, Australia and the UK over a period of 12 months. Most of these people were not seeking professional help and were ready to quit in the next 30 days.10
Smartphones with their advanced processing capabilities, rapid global uptake, proximity to the user and push notifications (a short message service-like function that is free of cost and more interactive),11 are potentially an ideal vehicle for health interventions.12 In addition, smartphone apps have shown feasibility across diverse ranges of health conditions.10 13–15 Although app stores have hundreds of smoking and tobacco-related apps, the majority are of low quality, very few provide evidence-based content and some are actually pro-smoking apps.9 16 17
The efficacy of smartphone apps as an intervention for smoking cessation remains untested, although three small pilot studies have shown a potential effect on short-term abstinence rates.13 18 19 This study, the Smartphone Smoking Cessation Application (SSC APP) trial, therefore, is the first that we are aware of to assess the efficacy of a SSC APP in a full-scale, multicountry, longer-term trial. It tests the efficacy of an interactive smoking cessation decision-aid app compared with a smoking cessation static information app on quit rates.
Methods
Study design
This is an automated, double-blind, randomised controlled trial (RCT) to determine the efficacy of a smartphone smoking cessation decision-aid app with support features compared with an app that contains only smoking cessation information. An overarching app was developed that included the baseline questionnaire and two sub-apps—the intervention and control apps. The participants from the USA, Australia, Singapore and the UK were randomised over a 5-month period. These countries were selected because of high smartphone coverage, English language, high income and good access to smoking cessation treatments across different geographical regions globally.10 The study app was published on the Apple App Store during the recruitment period and was the main portal of advertising the trial. We also advertised the app as an (in-app) advertisement to Apple iPhone users while they are using other apps, allowing for demographic targeting.
Participants
Users of the Apple App Store in the four countries were recruited passively via the app’s download page in the Apple App Store. The App Store description advised them that by downloading the app they would be participating in the study, that they could read the provided information about smoking and options for quitting, complete a questionnaire to find out their nicotine dependency test score and rate the information for its helpfulness in motivating them to quit. The app would collect anonymous data about how often the app was used and how long it was used for, and their internet protocol (IP) address would be collected only to identify duplication of data in our database and then deleted permanently. No personal identifying information would be collected through the app or the questionnaire. All anonymous data including the questionnaire responses, information ratings, frequency/duration of use and IP address would be sent directly from the app in their phone to an online secure research database. The eligibility criteria were daily smokers of cigarettes, 18 years old or over and from the included countries. Occasional smokers and users of other tobacco products were excluded.
Patient involvement
Patients were not directly involved in the design of this study. However, a previous study has explored the potential participants’ characteristics to inform this study design.9
Baseline registration and data collection
When a participant opened the app for the first time, the app assigned them a unique device identifier and registered the user’s smartphone device in our secure remote database. The unique device identifier could not change if the user deleted the study app and reinstalled it. This allowed anonymous data collection, prevented duplicate enrolments and contamination between groups. As this study is fully automated, not being able to ensure that some users may download the app from another device is an unavoidable limitation. However, to monitor users who download the app onto two devices, we have implemented a server-side IP that can identify the users who use different devices connected to the same internet network at similar times. This may not completely eliminate the possibility of contamination but will reduce it. To increase the response rate to the baseline questionnaire, we have implemented a reminder function that will send a notification to the user to complete the baseline questionnaire. The baseline questionnaire included sociodemographic variables (age, sex, educational level, marital status and income level) and tobacco consumption (eg, number of cigarettes smoked per day and nicotine dependence as measured by the Fageström test).20
Randomisation and blinding
The study app automatically randomised eligible participants (daily cigarette smokers, aged 18 years and above and from the four countries) to either the intervention or the control sub-app using stratified block (age, gender, country) randomisation. The strata were defined by age, country and gender. Participants and all investigators were blinded to group allocation (double blind).
Intervention and control app components
Both apps motivated the participant to set a quit date. The intervention app included four main components that made optimal use of smartphone features: (1) mandatory information about quitting options, with their benefits and harms; (2) daily motivational messages using push notifications sent from the study server, (3) a quitting diary and (4) a quitting benefits tracker. The intervention app could thus be described as a smartphone ‘decision aid with additional support’ because it included structured content on the options, benefits and harms of smoking cessation, along with ongoing support and motivation for the implementation and adherence to a quit decision through the use of push notifications, motivational messages, a diary and benefits tracker. Unlike many existing smoking cessation services through mobile phones and quit-lines, the decision-aid app allowed smokers to freely choose a quit method through a structured process of weighing up the available options and their benefits and harms. The decision-aid design was based on the Ottawa Decision Support Framework that draws on a number of psychological and behavioural theories (https://decisionaid.ohri.ca/odsf.html).
The control app included non-mandatory information about quitting options, benefits and harms, similar to those available in the intervention app. It did not provide any structured process for considering options, benefits and harms of quitting methods nor did it provide ongoing support for adherence to a quit decision. This could therefore be described as a smartphone app with information only. As stated earlier, both the intervention and control apps encouraged users to set a quit date. Full details about the study design, the intervention and control apps are available in the published protocol.12 A public version of the intervention app called ‘Quit Advisor Plus’ is available for downloading free of charge from the Apple App Store.
The follow-up data were collected by pushing a notification to the participants that were received even if the app was not running. Participants could also click on a follow-up button inside the app to initiate the follow-up process if the follow-up time had come. The follow-up notification generated an automated process where participants could click ‘yes’ or ‘no’ to answer the follow-up questions.
Outcomes
The primary outcome was the proportion of participants who remained completely abstinent after 1 month. Participants were asked the question “Have you been totally smoke-free (‘not even a puff’) for the last x days/months?” at 10 days, 1 month, 3 months and 6 months. Secondary outcomes were the proportion who made quitting attempts of at least 24 hours, abstinence rates at 10 days, 3 months and 6 months, the proportion who made an informed choice (based on the Multidimensional Measure of Informed Choice (MMIC)— 10 days after quitting) and the proportion with low decisional conflict (SURE score of less than 4 measured 10 days after quitting).21
Statistical analysis
We calculated a sample size of 672 participants to achieve 80% power at a 0.05 significance level to detect a change in continuous abstinence after 1 month from 5% to 15% allowing for 20% loss to follow-up.12 All analyses were undertaken on an intention-to-treat basis. To account for the non-responses at follow-up, four multiple imputation models were constructed for the non-responses at the follow-up at 10 days, 1 month, 3 months and 6 months continuous abstinence. The covariates that were included in the models were age, gender, educational level, income level, nicotine dependence, intervention group, selected quitting method and country. Ten imputed datasets were generated based on Rubin’s formula for relative efficiency to produce about 99% efficiency.22 We also conducted a sensitivity analysis with the assumption that all participants with missing outcome data were smokers.23 Effect measures were relative risk (RR) and 95% CIs. We assessed whether the effect of the intervention on abstinence rates was mediated by choice of quitting method or use of particular app components such as the use of the benefit tracking function by applying the method of Baron and Kenny.24
Results
The recruitment process started on 5 May 2014 and continued until the required sample size was reached on 1 September 2014. The 684 participants were randomly assigned via our automated randomisation algorithm to the intervention or control group (figure 1). Treatment groups were balanced with respect to baseline characteristics (table 1). χ2 analysis to examine the non-response at 1-month follow-up association with intervention groups revealed that non-response was independent of the intervention groups χ2(1, n=684)=1.2, P=0.27. However, turning off the app push-notification function (8.6% of the participants) was associated with non-response χ2(1, n=684)=11.1, P<0.001.
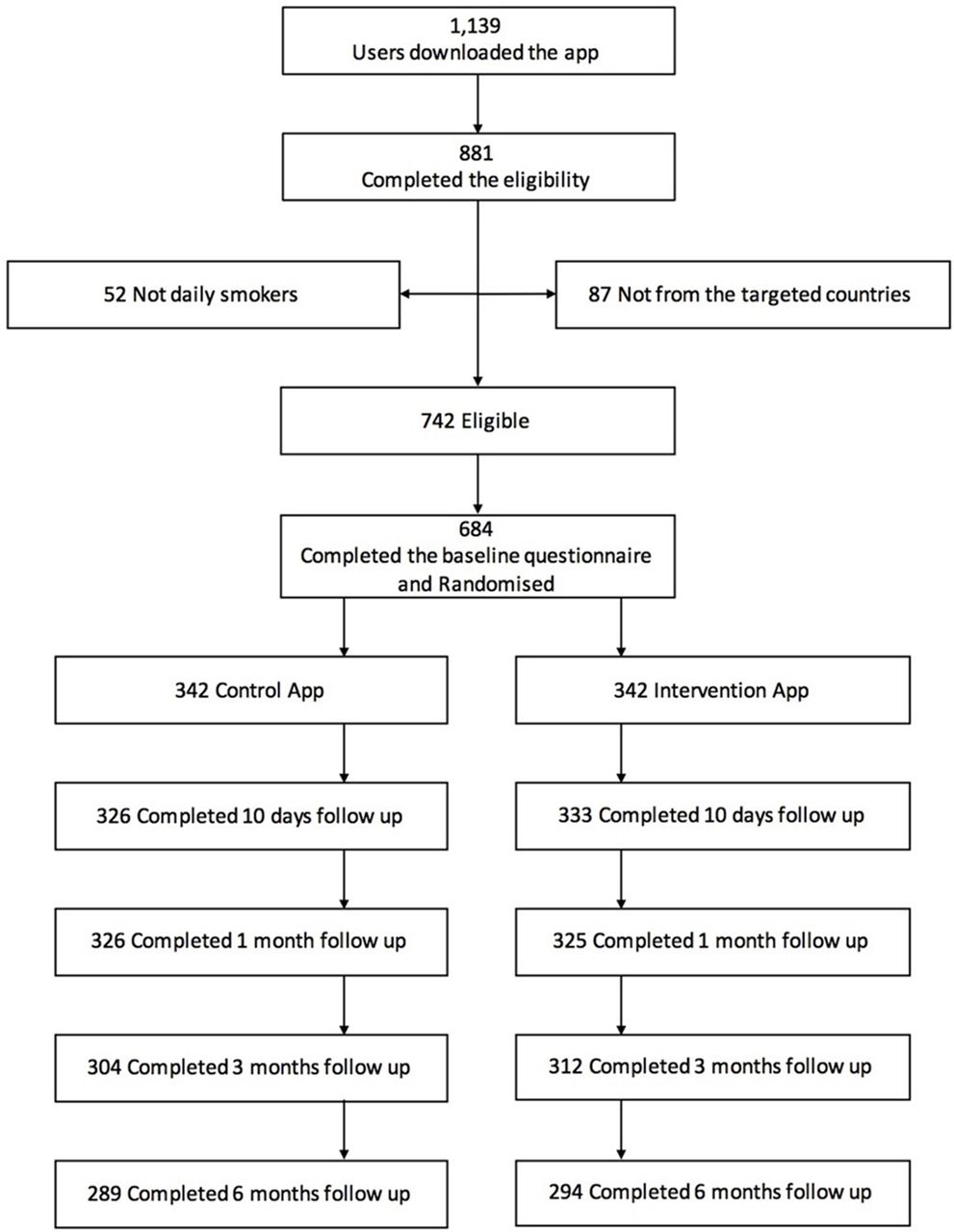
{kind=link}
Flow chart for trial. app, application.
Baseline data of participants and self-reported quitting method (n=684)
The majority of participants in both groups decided to quit unassisted, followed by nicotine replacement therapy (NRT) (table 1). Only 2.3% of the participants changed their selected quitting method within the first 10 days.
The multiple imputations results showed that self-reported continuous abstinence at 10 days, 1, 3 and 6 months was significantly increased by the intervention app (table 2). At 1 month, 28.5% of those in the intervention arm were completely abstinent compared with 16.9% in the control arm. Similar results were obtained when the participants who were lost to follow-up were treated as smokers (table 3) at the main outcome 1 month (continuous abstinence 13.2% (45/342) control vs 26.0% (89/342) intervention; RR 1.97, 95% CI 1.41 to 2.79, P<0.001), and when excluded (table 3) (continuous abstinence 14.2% (45/317) control vs 27.4% (89/325) intervention; RR 1.92, 95% CI 1.39 to 2.66, P<0.001).
Primary and secondary outcomes (number of imputations=10)
Self-reported abstinence (intention to treat analysis)
In three countries, abstinence rates at 1 month were significantly higher in the intervention group compared with the control group (USA (RR 1.83, 95% CI 1.04 to 3.25), Australia (RR 2.29, 95% CI 1.13 to 4.64), UK (RR 1.97, 95% CI 1.10 to 3.55), but not Singapore (RR 1.56, 95% CI 0.71 to 3.44). There was no statistically significant difference in the effect of the intervention between the countries.
The effect of quitting method on continuous abstinence at 1 month was assessed in a logistic regression analysis using the imputed data adjusting for age, gender, educational level, country, treatment groups. None of the quitting methods were associated with abstinence compared with ‘No treatment (quitting unassisted)’. The quitting method did not mediate the impact of the intervention since method chosen was not associated with abstinence (P=0.99) and inclusion of method did not alter the estimate of the intervention effect.
Finally, we measured the effect of ‘app component use’ on quitting, using a logistic regression model with the imputed data at 1 month and 6 months. The model included the quitting benefit tracker use, quitting diary use and the self-reported reading of the compulsory information adjusting for age, gender, educational level, country, quitting support method. Only the quitting benefit tracker was significantly associated with continuous abstinence at 1 month (OR 3.85; CI 2.15 to 6.91) and 6 months (OR 4.27; CI 1.53 to 11.88). Mediator analysis was not preformed because the quitting benefit tracker was only available in the intervention app which violated the mediation analysis assumptions.
In terms of the decisional conflict, 19.5% of the participants in the intervention group had low decisional conflict compared with 3.9% in the control group χ2(1, n=684)=28.4, P<0.001. Table 4 shows the MMIC at 10 days after quitting with participants receiving the decision-aid app more likely to make an informed choice than those getting the information-only app (31.9% vs 19.6%), χ2(1, n=684)=12.8, P<0.001.
Rates of informed and uninformed choice—intervention and control
Discussion
The results of this fully automated RCT show that continuous abstinence from smoking at 1, 3 and 6 months was significantly increased by a smartphone decision aid that included behavioural support compared with a simple non-mandatory information-only app. Most of the participants chose to quit via ‘No treatment (unassisted)’ with intervention recipients being more likely to make an informed choice and have lower decisional conflict than those receiving the information-only app. We have also shown that smartphone apps can be successfully used in an RCT design, with good follow-up response rates in both groups. Turning off the app push notification was associated with follow-up non-response.
We believe our intervention app was successful in achieving the 28.5% 6-month continuous abstinence rates because it combined features of previously evaluated smoking cessation interventions that were shown to be effective—that is, decision aids and mobile phone interventions. Willemsen et al 25 conducted an RCT of a smoking cessation decision aid over a decade ago. While the aid increased 6-month continuous abstinence rate to 20.2% compared with no decision aid (13.6%), it consisted of a box with leaflets, a video and some treatment samples which were posted to the home. The researchers reported an increase in knowledge, a more positive attitude, an increase in confidence about quitting and feedback that the decision aid helped them decide on a quit method. Second, there has been increasing evidence for the efficacy of mobile phone interventions (mainly text messages or counselling).8 We hypothesise that our 6-month abstinence rate of 28.5% is due to the combined effect of decision support and the convenience of mobile technology. In addition, the effect of smartphone-unique features on health behaviour change has not yet been assessed and this study is the first to do so.10
Strengths
A strength of our intervention was that it incorporated patient decision-aid features which significantly increased the proportion of people who made an informed choice that was concordant with their personal values and significantly reduced decisional conflict about their quit decision. Comparing our results to a previous paper-based smoking cessation decision-aid RCT,25 our study has also shown comparable results at short-term and long-term follow-up period but has the added convenience of smartphone accessibility.
Importantly, about 56.0% of the participants in this study (in both groups) had made a previous quit attempt that had lasted at least 24 hours. This is relatively consistent with our finding in the feasibility study where the majority (75.6%) of participants who had used smoking cessation apps in the past had made a quitting attempt that lasted at least 24 hours using an app.10 It supports the notion that smartphone apps are an effective way of reaching serious ‘quitters’ who tend to quit ‘unassisted’.25 Interestingly, our study participants who used NRT had similar results to those who quit unassisted. Although, this study was not powered for subgroup analyses, our intervention was effective in three countries out of four.
Furthermore, 77.3% of those who downloaded the app, completed the eligibility test and of those eligible, 92.2% completed the baseline questionnaire. The introduction of the push notification reminders in this study may have contributed to this high response rate, with other studies reporting similar results with this method.15 26 By contrast, our feasibility study only generated a response rate of 36.8% without reminders.10 Our trial retention rate was good with 1-month follow-up (93.9%) and 6-month follow-up (85.2%). Another study comparing a smartphone app with a website found that trial retention was 93% at 6 months in the smartphone group, compared with 55% in the website group.14 Turning off the app push-notification feature was associated with loss to follow-up. In future, the app could include an in-app reminder to the user to turn on the push notification.
Limitations
One of the limitations of this study is that continuous abstinence was measured via self-report through the app questionnaires, which is less rigorous than a biochemically verified abstinence.27 Our study was not funded for the latter. The second limitation is the possibility of contamination between groups, although we took measures to minimise this through the unique IP feature.12 Finally, we recognise that the participants in this study were likely to be more motivated than other smokers because they were searching for smoking cessation apps during the recruitment period.
Generalisability
This study has used a novel approach for conducting an automated RCT via a smartphone app, and thereby simulated the ‘real-world’ setting, recruiting via the app store in multiple countries. This automated process eliminated hours of recruitment time, and cost, it reached various ages, education levels and income groups, including 31% of the participants with low incomes but still used an expensive smartphone device. However, the study sample was limited to four high-income countries, and the findings may not be generalisable to smokers with smartphones in other settings.
Future challenges
Unlike web technology where the intervention can be developed and hosted on the producer’s resources, smartphone apps are hosted on the publishers’ servers (eg, Apple app store or Google Play) and thus subjected to their changing regulation policies and technical specifications. For example, in this project the app was released on an iPhone operating system version that did not require the user to provide permission to receive local notifications (used in the quitting benefit tracker function). However, new versions of the iPhone operating system required the app producer to implement a user permission function to use local notifications. In this case, some users may disable the local notifications and the utilisation may be reduced. Thus, future interventions may need to come up with new solutions to improve the utilisation of specific app functions. The same issue was faced in another project that uses the location detection function to follow-up travellers for infection control purposes.28
Other smartphone operating systems such as Android allows the app producer to publish their apps via email or self-hosted web links. Although the producer may lose the mass exposure advantage by publishing their apps on the official app stores, they at least can avoid the changing policies issue.
Conclusions
A smartphone decision-aid app significantly increased smoking cessation rates with greater informed choice and lower decisional conflict across three out of four countries. It shows that the benefits of earlier mobile phone smoking cessation interventions can potentially be transferred to the more contemporary and user-friendly smartphone interface. We have also demonstrated the feasibility of conducting an RCT entirely using smartphone technology. Evidence-based decision-aid apps should be promoted to smokers who are thinking of quitting.
References
Footnotes
Contributors All authors made substantial contributions to editing and revising of the manuscript. NFB was responsible for the conceptual development, the app design and development, and drafting of the manuscript. NFB and LT were responsible for the study design. NFB and KM were responsible for the statistical analysis. All authors read and approved the final manuscript.
Funding The app was developed by NFB as part of a PhD degree, advertisement was covered by a small fund from the PhD sponsor (Ministry of Education, Saudi Arabia).
Competing interests None declared.
Patient consent Not required.
Ethics approval The trial was approved by the University of Sydney’s Human Research Ethics Committee (Project Number 2013/513).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Relevant anonymised patient-level data are available on reasonable request from the authors.