Article Text

Abstract
Objective To investigate suicide and mortality risk in deployed military veterans versus non-deployed comparators who had gone through military conscription testing.
Design Population-based matched cohort study.
Setting Sweden.
Participants Participants were identified from the Military Service Conscription Register and deployment status from the Swedish Military Information Personnel Register. Of 1.9 million conscripts, 21 721 had deployed at some time between 1990 and 2013 (deployed military veterans). Non-deployed comparators were matched to deployed military veterans in two ways: (1) by cognitive ability, psychological assessment, mental health, body mass index, sex, birth-year and conscription-year (carefully matched), with further adjustment for exercise capacity and suicide attempt history; and (2) by sex, birth-year and conscription-year (age- and sex-matched).
Main outcome Suicide retrieved from the Swedish National Patient and Causes of Death Register until 31 December 2013.
Results During a median follow-up of 12 years, 39 and 211 deaths by suicide occurred in deployed military veterans (n=21 627) and carefully matched non-deployed comparators (n=107 284), respectively (15 vs 16/100 000 person-years; adjusted HR (aHR) 1.07; 95% CI 0.75 to 1.52; p=0.72) and 329 in age- and sex-matched non-deployed comparators (n=108 140; 25/100 000 person-years; aHR 0.59; 95% CI 0.42 to 0.82; p=0.002). There were 284 and 1444 deaths by suicide or attempted suicides in deployed military veterans and carefully matched non-deployed comparators, respectively (109 vs 112; aHR 0.99; 95% CI 0.88 to 1.13; p=0.93) and 2061 in age- and sex-matched non-deployed comparators (158; aHR 0.69; 95% CI 0.61 to 0.79; p<0.001). The corresponding figures for all-cause mortality for carefully matched non-deployed comparators were 159 and 820 (61 vs 63/100 000 person-years; aHR 0.97; 95% CI 0.82 to 1.15; p=0.71) and 1289 for age- and sex-matched non-deployed comparators (98/100 000 person-years; aHR 0.62; 95% CI 0.52 to 0.73; p<0.001).
Conclusion Deployed military veterans had similar suicide and mortality risk as non-deployed comparators after accounting for psychological, psychiatric and physical factors. Studies of mental health in deployed veterans need to adjust for more factors than age and sex for comparisons to be meaningful.
- Deployment
- Military
- Suicide
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
In this population-based study, data were collected from nationwide registers from military conscription and the universally accessible national healthcare system, providing access to several pre-existing risk factors for suicide including cognitive ability, psychological assessment scores, mental health history and physical fitness.
Using the unique personal identity number of each Swedish resident, follow-up was complete regarding all-cause mortality and registered suicide.
Generalisability to other countries of the absolute rates of suicide is limited by cultural differences, different national recruitment strategies for the military and military operation area.
In the absence of randomisation and despite careful matching on baseline psychiatric, psychological and physical factors, the military selection process may have resulted in remaining selection bias and residual confounding.
Introduction
Mental health in deployed military veterans has received considerable attention as traumatic events may cause mental health problems, instantly or with delayed onset.1 Some countries report that their recent deployed military veterans have worse mental health than the general population as well as earlier-era deployed military veterans.2 3
Although military personnel deployed abroad commonly are exposed to stressful events, there is conflicting evidence regarding their suicide risk. Compared with the general population, a lower suicide risk has been reported among UK,4 French5 and Swedish deployed military veterans.6 In some US studies, deployed military veterans have also been found to have a lower risk of suicide and all-cause mortality compared with the general population,7 8 while others have reported a twofold higher risk.9 Other studies performed on US and Danish military veterans have not detected any differences among military veterans versus the general population.10 11
Suicide rates may also be a moving target: the report from the US Veterans Affairs ‘Suicide Among Veterans and Other Americans 2001–2014’ described how the risk of suicide among US active duty service members surpassed US civilians in 2008, but that it later dropped below the rate observed among civilians of comparable age and sex.12 However, the overall rate masked a 10-fold higher suicide rate among recently discharged veterans aged 18–24 years compared with civilians.
Military personnel are commonly selected based on performance on physical and psychological tests which are conducted before entering military service. The purpose of such testing is partly to evaluate the capability of managing physical and psychological stress. By not accepting everyone applying for military service, this creates a group of individuals who are in overall better shape than the general population, a selection bias referred to as the ‘healthy soldier effect’.8 13 14 Most studies comparing suicide and other mortality outcomes among military personnel to the general population are likely affected by this bias.15 16 A potential additional selection bias termed the ‘healthy warrior effect’ may also affect results, as military personnel selected for deployment may be in better health than those not selected.17 18
The aim of this study was to investigate the risk of suicide among previously deployed Swedish military personnel compared with two different non-deployed matched comparator groups based on individuals who had gone through military conscription testing, one that accounted for demographic, psychological, psychiatric and physical fitness factors and one that took only age and sex into account.
Methods
This is a population-based cohort study of suicide risk among previously deployed Swedish military personnel (deployed military veterans) and matched comparators without deployment history identified from the Military Conscription Service Register including individuals who had gone through military conscription tests but not necessarily completed military training (see online supplementary appendix table 1). The cohorts were created and outcome data collected by linking nationwide Swedish registers by use of the unique personal identity number assigned to each Swedish resident. The study was approved by the regional ethics committee at Karolinska Institutet, Stockholm, Sweden. Data were deidentified prior to delivery to the research group.
Setting
Sweden has been contributing military personnel to United Nations sanctioned operations since 1956 and North Atlantic Treaty Organization sanctioned operations since 1990. Military conscription was mandatory for Swedish men until 2010. Around the age of 18 years, all men (excluding those with severe disabilities) went through conscription tests with extensive physical and psychological assessment. Test results have been saved electronically since 1969.
During the era of mandatory military conscription, military deployment abroad was voluntary. In 2010, rules changed due to political decisions with military conscription put dormant and a transition to professional armed forces began. During the study period (1990–2013), Swedish military forces were deployed in 27 different countries. During the 1990s, most deployments were in the Balkans and between 2008 and 2013 Afghanistan dominated (see online supplementary appendix figure 1).
Data sources
Data were collected from the National Board of Health and Welfare, the Military Archives, the Swedish Defense Recruitment Agency, Statistics Sweden and the Swedish Armed Forces.
The Swedish Military Information Personnel Register
The current study was based on deployment data retrieved from the Swedish Military Information Personnel Register (SWIP) of individuals deployed abroad at some point between 1990 and 2013. The SWIP Register includes all types of service members, armed and unarmed, and includes information about country of deployment, date of deployment and return, sex, age, military rank, personal identity number and regiment. All deployed military personnel have been registered in SWIP since 1965 except individuals serving in the Special Forces and classified personnel (representing <1%; personal communication, Swedish Armed Forces research coordinator Anders Claréus, 5 June 2015). Since 2012, the same deployment information, and additional salary information, has been entered into a new database called PRIO.
The Military Service Conscription Register
The Military Service Conscription Register has been described in greater detail elsewhere.19 Briefly, it contains data on all men and women going through a 2-day test protocol at military conscription, including both physical and psychological examinations. While conscription testing has been voluntary for women, only 2%–3% of all Swedish men were exempt from conscription testing until 2005, in most cases because of severe disabilities or congenital disorders. After 2005, the number of conscripts dropped to about a third of each birth cohort due to political decisions. In 2010, mandatory conscription was put dormant.
The Register of the Total Population
Date of emigration was retrieved from this register, which includes all Swedish residents and is managed by Statistics Sweden.20
The Causes of Death Register
This register tracks mortality and causes of death among Swedish residents. Causes of death are coded using the International Classification of Diseases (ICD) codes by the physician who determines the time of death. In some cases causes of death are missing (1.8% in 2011).21
The National Patient Register
This register was started in 1964 and attained nationwide coverage for inpatient care in 1987.22 In 2001, hospital-based outpatient care was added. Data on psychiatric inpatient and outpatient care were retrieved from the National Patient Register, which contains data on admission and discharge date and causes of admission.
Study population
Three cohorts were identified via the Military Service Conscription Register for this study, including individuals who had gone through military conscription testing but without requirement of completed military service (see online supplementary appendix figure 2).
Deployed military veteran cohort
Swedish military personnel who deployed at some time between January 1, 1990, and December 31, 2013 were identified through the SWIP and PRIO registers.
Non-deployed comparator cohorts
Through the Military Service Conscription Register, we identified 1.9 million potential comparators. In the carefully matched cohort, up to five comparators were matched to each deployed veteran on sex, birth-year (1950–1994), conscription-year (1969–2013), cognitive ability (1–9, missing), psychological assessment (1–9, missing), self-reported mental health problems (yes/no), body mass index (BMI; kg/m2; <18.5, 18.5–19.9, 20.0–22.4, 22.5–24.9, 25.0–27.5, 27.5–29.9, 30.0–60.0, missing) and deployment year (1990–2013). Individuals who had served abroad before 1990 were not eligible to be selected as comparators. As matching date, comparators were given their deployed military veteran homecoming date. The purpose of this carefully matched comparator group was to serve as benchmark when accounting for differences between deployed military veterans and the whole group of non-deployed comparators in demographics, cognitive ability, psychological resources and mental health.
A second comparator cohort was also created, matched on sex, birth-year and conscription-year. The purpose of this comparator group was to provide a benchmark for death by suicide and all-cause mortality based on the whole group of individuals going through military conscription testing.
Outcome and follow-up
The primary outcome was death by suicide retrieved from the Causes of Death Register until 31 December 2013. Participants were followed from the date of return from deployment (or matching date for comparators) until death by suicide, death from other cause, emigration or end of follow-up, whichever came first. We used the following ICD codes to identify death by suicide: ICD9 E950–E959 and E980–E989; ICD10: X60–X84 and Y10–Y34.
As additional outcomes, we analysed confirmed deaths by suicide (ICD9: E950–E959, ICD10: X60–X84; that is, excluding deaths from undetermined intent), the combined outcome death by suicide or attempted suicide by adding data also from the National Patient Register (ICD9: E950–E959 and E980–E989; ICD10: X60–X84 and Y10–Y34) and all-cause mortality.
Variables
We retrieved data on cognitive ability, psychological assessment test score, BMI, exercise capacity, previous mental health problems, history of attempted suicide and healthcare contacts due to psychiatric disorders.
Cognitive ability
At conscription testing, verbal, spatial, logic inductive and technical ability were tested.23 The four different variables were assessed on a STAndard-NINE scale (Stanine; from 1 to 9 with a normal Gaussian distribution, where 9 represents the top 4% and 1 the bottom 4%) and weighted to a G-factor value also presented on a Stanine scale.24 25
Psychological assessment
At conscription, conscripts were individually interviewed by a psychologist using a semistructured interview form along with a questionnaire to assess ability to cope with prolonged and elevated stress, leadership skills as well as suitability for military service.26 Results were reported on a Stanine scale.
Mental health problems
History of mental health problems was retrieved from a self-reported question (yes/no) at conscription testing, as well as through the National Patient Register as any recorded psychiatric diagnosis (ICD9: 290–315; ICD10: F00–F99) prior to deployment/matching date. History of attempted suicide prior to deployment was also retrieved from the National Patient Register.
Physical health
At conscription/testing, participants had their height and weight measured. We categorised BMI into underweight (<18.5), normal weight (18.5–24.9), overweight (25–29.9) and obese (≥30). We have previously found BMI to be associated with all-cause mortality.27
Exercise capacity
At conscription/testing, participants were evaluated using a maximum exercise capacity test (measured in watts) by using an ergometer bicycle. After 5 min of low-resistance and high-frequency bicycling, the load was gradually increased by 25 W per min until the conscript was no longer able to go on with the test due to exhaustion.28
Blood pressure
Blood pressures were measured according to a written protocol after 5 to 10 min of rest in the supine position, with an appropriately sized cuff at heart level. A single measurement was made if systolic blood pressure was 145 mm Hg or less and diastolic blood pressure was between 50 and 85 mm Hg. If measurements were outside these limits, blood pressure was measured a second time, and the result of the second measurement was used.29
Statistics
Comparison of the descriptive data of the deployed military veterans and their unmatched non-deployed comparators were performed by t-tests for continuous variables and χ2 tests for categorical variables. For conditioned comparisons of the matched cohorts, analysis of variance was used for continuous variables and logistic regression for categorical variables. Conditioning was made on the matching set (with each set consisting of one deployed military veteran and up to five matched comparators) to account for the matched design.
Incidence rates and Kaplan-Meier failure functions were used to present absolute risks. Cox proportional hazards models were used to estimate hazard ratios (HRs) for (1) death by suicide, (2) death by suicide or attempted suicide and (3) all-cause mortality. The models were estimated conditioned on the matching set. For the comparison with the carefully matched non-deployed comparator group, additional adjustment was performed for history of attempted suicide, history of psychiatric care prior to deployment/matching and exercise capacity measured at conscription.
Subgroup analyses were performed for the outcome death by suicide or attempted suicide by sex, age at deployment, psychological assessment and cognitive ability.
Data were analysed using SAS V.9.4 (SAS Institute) and Stata V.13.0. All tests were two-sided and p values<0.05 were considered statistically significant.
Patient/participant involvement
The protocol for this research project has been presented to representatives from associations of Swedish deployed military veterans, as well as for the Swedish Armed Forces Veteran Department.
Dissemination of results will be done through presentations at the annual Veterans’ Day, at seminars on veteran affairs organised by the Armed Forces Veteran Department and through direct contact with the main associations of deployed military veterans.
Results
Between 1990 and 2013, we identified 42 613 deployments performed by 25 073 individuals. Of these, 3341 were excluded due to missing military conscription data, and 11 who died during deployment. For each of the remaining 21 721 deployed military veterans, we attempted to carefully match up to five non-deployed comparators who had performed military conscription testing, but for 94 individuals no comparators could be identified. The final sample consisted of 21 627 deployed military veterans and 107 284 comparators. For the second comparison group, matched only for age and sex, the corresponding numbers were 21 628 and 108 140.
Participant characteristics
Before matching, the deployed military veteran cohort had higher cognitive ability, lower prevalence of mental health problems and better results on the psychological assessment than comparators (table 1; figure 1; all p<0.001). These differences were eliminated by the matching procedure (carefully matched cohort) (table 1). No difference was detected in history of attempted suicide (0.6% vs 0.5%; p=0.07), but hospital visits listing a psychiatric diagnosis prior to deployment/matching date were less common among deployed military veterans than carefully matched comparators (2.3% vs 2.9%; p<0.001; table 1). The mean age at deployment was 27 years (SD 6).

Distribution of results from the intelligence test, psychological assessment and body-mass index in deployed military veterans and age- and sex-matched non-deployed comparators
Participant characteristics
Death by suicide
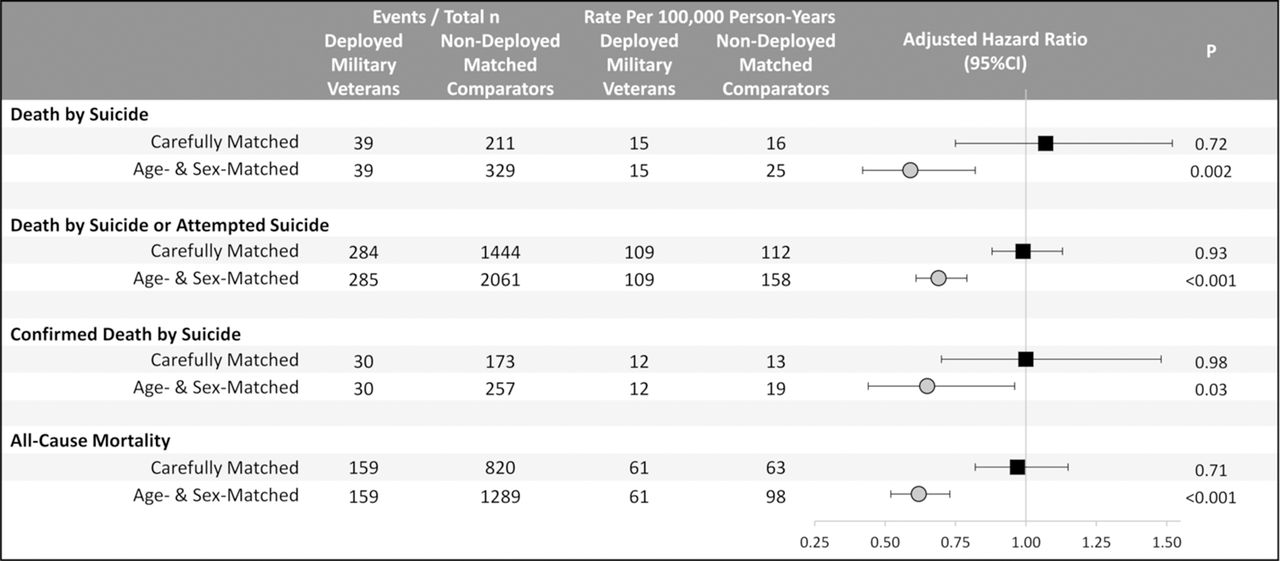
During a median follow-up of 12 years, 39 deaths by suicide were registered in the deployed military veteran cohort compared with 211 in the carefully matched comparator cohort (15 vs 16 per 100 000 person-years; adjusted HR (aHR) 1.07; 95% CI 0.75 to 1.52; p=0.72), while a lower risk in deployed military veterans was observed compared with only age- and sex-matched comparators (aHR 0.59; 95% CI 0.42 to 0.82; p=0.002; figures 2 and 3). Results were similar when analysing confirmed deaths by suicide.

Death by suicide, attempted suicides and all-cause mortality among deployed military veterans versus carefully matched non-deployed comparators (n=21 627/n=1 07 284) and versus age- and sex-matched non-deployed comparators (n=21 628/n=108 140).

{kind=link}
{kind=link}
{kind=link}
Cumulative incidence of death by suicide, death by suicide or attempted suicide, confirmed death by suicide and all-cause mortality.
Death by suicide and attempted suicide
Regarding death by suicide or attempted suicide, there were 284 and 1444 such events registered during follow-up in deployed military veteran cohort and the carefully matched comparator cohort, respectively (109 vs 112 per 100 000 person-years; aHR 0.99; 95% CI 0.88 to 1.13; p=0.93; figures 2 and 3). Accounting only for age and sex, deployed military veterans had lower risk (aHR 0.69; 95% CI 0.61 to 0.79; p<0.001).
All-cause mortality
During follow-up, 159 deployed military veterans died in comparison to 820 of the carefully matched comparators (61 vs 63 per 100 000 person-years; aHR 0.97; 95% CI 0.82 to 1.15; p=0.71) and 1289 for the age- and sex-matched cohort (aHR 0.62; 95% CI 0.52 to 0.73; p<0.001; figures 2 and 3).
Subgroup analysis
For the outcome death by suicide or attempted suicide, no subgroup differences were detected by sex, age, psychological assessment or cognitive ability versus the carefully matched cohort (see online supplementary appendix figure 3).
Discussion
After accounting for psychological, psychiatric and physical fitness factors, deployed military veterans showed no difference in suicide or mortality risk in comparison to non-deployed carefully matched comparators who had performed military conscription testing. If only matching comparators for age and sex, deployed military veterans had a substantially lower risk of both suicide and all-cause mortality than these age- and sex-matched comparators. These results illustrate the difficulty in selecting comparators for assessment of suicide and mortality risk in deployed military veterans unless detailed data are available on both deployed veterans and comparators.
Previous research
To the best of our knowledge, no previous study comparing suicide risk in deployed military veterans versus the general population has matched non-deployed comparators by psychological, psychiatric and physical fitness factors. Not taking suicide risk factors that are differentially distributed in the deployed military veteran population and the general population into account is likely the explanation for the lower suicide risk found in deployed military veterans versus the general population in previous US,30 UK,4 French5 and Swedish studies.6
Based on standardised mortality ratios, a previous Swedish study showed a 50% lower suicide risk among veterans deployed 1960–1999 than in the general population after taking age and sex into account,6 while reports from Norway and Denmark have reported no difference versus the general population.31 32 These findings are difficult to interpret as it is likely that also their cohorts of deployed military veterans differ from the general population in terms of psychological, psychiatric and physical fitness.
Regarding the absolute risk of death by suicide, a study from the American Millennium Cohort of active duty military personnel and veterans reported an incidence of 12 suicides per 100 000 person-years compared with 15 in our study.33 They detected no military-specific correlates to suicide33 but large excess risks associated with mental health problems and substance use. They did not compare suicide risk with the general population, but found no difference between deployed and non-deployed military personnel.
Mechanism
In our main analysis, we found deployed military veterans to have lower suicide risk than the general population when only taking age and sex into account, but the difference disappeared after accounting also for baseline psychiatric, psychological and physical factors that differed between the two groups.
We found that mental health problems at conscription was almost five times more common in age- and sex-matched non-deployed comparators than deployed military veterans, that >20% had low cognitive test score results versus <10% among deployed military veterans and that 12% had low results on the psychological assessment compared with 2.5% among deployed military veterans. Deployed military veterans also had considerably greater exercise capacity. Given these observations regarding psychological and psychiatric characteristics, it is expected that analyses taking only age and sex into account are insufficient for assessment of suicide and mortality risk. In our analyses, the HR moved from a large and statistically significant protective effect to a non-significant effect near null.
Implications
Deployed military veterans are a selected group of mentally healthy individuals compared with the whole group of individuals going through military conscription testing. Therefore studies of mental health after foreign military deployment need to take more factors than age and sex into account for comparisons to be meaningful. Our results show how previous estimates of suicide risk in Swedish deployed military veterans, and likely deployed veterans in other countries, have been biased by failing to account for the greater cognitive, psychological and physical fitness of individuals selected for military deployment.
Strengths
Strengths of this study include the use of national registers enabling us to follow a large number of individuals over a long time period with minimal loss to follow-up, as well as to characterise them based on both conscription and predeployment psychological, psychiatric and physical characteristics. Second, up to five non-deployed comparators were matched to every deployed military veteran according to multiple factors associated with suicide and were thereafter combined with additional adjustment for mental health and exercise capacity.
Limitations
This was not a randomised trial and we can therefore not conclude that foreign military deployment increased or decreased suicide risk. Suicide studies in this field, where randomisation is near non-existent,34 struggle with selecting a relevant comparator group. We chose to match comparators by age, sex, cognitive ability, psychological assessment score, history of mental health problems and BMI from a pool of individuals who had undergone mandatory military conscription tests. We further adjusted for history of attempted suicide and exercise capacity to reduce the healthy soldier and healthy warrior effect. However, selection bias and residual confounding may have remained with deployed military veterans differing systematically from the carefully matched non-deployed comparators in factors associated with the outcome.
We chose to include both confirmed and unconfirmed suicides (deaths with undetermined intent) in our main analysis, as is customary in Swedish suicide statistics. This will overestimate the number of true suicides but not as much as it would underestimate the number of true suicides by excluding those coded as unconfirmed.35 36 Unconfirmed suicides have been described to predominantly be different kinds of poisoning.21 36 When restricting our analysis to only deaths by suicide coded as confirmed, the findings were the same. We also analysed all-cause mortality with similar observations as for death by suicide.
An additional potential limitation was the lack of information on combat exposure, which might influence mental health.37 However, studies suggest a weak, if any, association between combat exposure and suicide risk in US military personnel.33 38 We also did not have access to data on help-seeking behaviour or access to lethal means.
Finally, the generalisability of our findings may be limited by cultural differences between countries, as well as differences in the population groups from which the military recruits personnel.
Conclusions
Deployed military veterans did not differ from non-deployed comparators in suicide or mortality risk after accounting for psychological, psychiatric and physical fitness factors. If only taking age and sex into account, deployed military veterans displayed substantially lower risks, illustrating the impact of the healthy soldier and healthy warrior effect.
References
Footnotes
Contributors MN is the principal investigator. CMP wrote the first draft of the manuscript. KJ was responsible for the preparation of data. CMP performed the statistical analyses. All the authors undertook revisions and contributed intellectually to the development of this paper. MN and CMP are the study guarantors.
Funding Research reported in this publication was supported by Kungafonden (the Royal Fund). The content is solely the responsibility of the authors and does not necessarily represent the official views of the Royal Fund.
Competing interests None declared.
Patient consent This study is a register-linkage study based on de-identified data.
Ethics approval Regional ethics committee in Stockholm, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data regarding technical details, statistical code and derived data are available from the lead author (carl-martin.pethrus@ki.se).