Article Text

Abstract
Introduction Vitamin B12 is crucial for normal cell division and differentiation, and necessary for the development and myelination of the central nervous system. Pregnant mothers in resource poor settings are at risk for poor vitamin B12 status. Poor vitamin B12 status in infancy is linked to poor growth and neurodevelopment. Brain development starts from conception, and pregnancy is a period of rapid growth and development for the brain.
Methods and analysis The study is an individually randomised double-blind placebo controlled trial in 800 pregnant Nepalese women randomised in a 1:1 ratio. A daily dose of 50 µg of vitamin B12 or placebo is given to women from early pregnancy, not later than week 15, until 6 months after birth. Weekly visits are conducted in order to record compliance, growth and morbidity. The primary outcomes are scores on the cognitive, language and motor subscales of the Bayley Scales of Infant and Toddler Development, Third Edition, measured at 6 and 12 months of age, and growth (length and weight) measured at 6 and 12 months of age.
Ethics and dissemination National Health and Research Council, Nepal (NHRC 253/2016) and Regional Committee for Medical and Health Research Ethics of Western Norway (2016/1620/REK vest) have approved the study. Investigators who have contributed to the conceptualising, conducting, as well as being involved in the data analyses and manuscript writing will be eligible for authorship and be responsible to share outcomes with different stakeholders through publications and workshops. The results from this study may support new dietary guidelines for Nepalese and possibly South Asian pregnant women that can lead to improved pregnancy outcomes, neurodevelopment and cognitive functioning in children.
Trial registration number Universal Trial Number: U1111-1183-4093. Trial registration: clinicaltrials.gov: NCT03071666. Protocol date: version 1.2, 1 June 2017.
- Cobalamin
- Nepal
- Pregnancy
- Supplementation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is a large-scale randomised controlled trial which aims to investigate the effect of maternal vitamin B12 supplement during pregnancy through 6 months postpartum on early child development and growth.
We are performing a comprehensive neurodevelopmental assessment with tools that have been previously used in the same population.
A potential caveat in this study is that not all women will have poor vitamin B12 status, and if the proportion of women with adequate status is high, this will reduce our statistical power which may result in failure to detect important differences.
The primary outcomes will be measured when the children are 6 and 12 months old, beneficial effects of improved vitamin B12 status of the mother might not be measurable in the children until later childhood.
Background
Cobalamin (vitamin B12) deficiency is common in many low and middle-income countries.1 2 This is not surprising as the main source of vitamin B12 is animal source foods, which are expensive and for cultural and religious reasons often not eaten at all. In several studies of women and children, we have demonstrated that poor vitamin B12 status is common in South Asia.3–5 There is also compelling evidence that vitamin B12 deficiency occurs frequently during pregnancy,2 6 7 and case studies have demonstrated harmful effects of severe vitamin B12 deficiency on the developing infant brain.8 9 The consequences of mild or subclinical vitamin B12 deficiency are less clear but it has been shown to be associated with decreased cognitive performance in both the elderly and children.10–13 Three randomised controlled trials (RCT) have measured the effect of vitamin B12 supplementation on neurodevelopment in children: In a Norwegian trial, an intramuscular injection of B12 substantially improved the motor development in 6-week-old infants after 1 month,14 another intervention study in low birthweight children recently confirmed these findings.15 The infants in these studies had evidence of suboptimal vitamin B12 status, but none was severely deficient. We found a beneficial effect of vitamin B12 supplementation for 6 months on neurodevelopment in young North Indian children.16 In this study, where the children were supplemented daily with two recommended daily allowances (RDA) for 6 months, the effect of vitamin B12 supplementation was more apparent in children who had evidence of vitamin B12 deficiency at the start of the study.
During pregnancy, vitamin B12 is concentrated in the fetus and stored in the liver.17 18 Infants born to vitamin B12-replete mothers have stores of vitamin B12 that are adequate to sustain them for the first several months postpartum. Consequently, vitamin B12 deficiency rarely occurs before the infant is about 4 months old if the mother has adequate vitamin B12 status during pregnancy. However, infants of vitamin B12-deficient breastfeeding mothers are vulnerable to B12 deficiency from an early age.19
Maternal vitamin B12 deficiency has been associated with increased risk of common pregnancy complications, including spontaneous abortion, low birth weight, intrauterine growth restriction and neural tube defects.20–22 Children born to vitamin B12-deficient women are at increased risk for adverse health outcomes, including developmental abnormalities and anaemia.9 23 In a recent RCT in Bangalore, India, daily maternal vitamin B12 supplementation (50 µg/day) during pregnancy through 6 weeks postpartum substantially improved maternal vitamin B12 status and increased breast milk and infant plasma vitamin B12 concentrations.24 In this study, the proportion of children being born small for gestational age was lower in the vitamin B12 group than in the placebo group (25% vs 34%); however, no difference was found in neurodevelopment in infants at 9 months of age.25 Similar improvements in vitamin B12 status were found among Bangladeshi mothers and infants when supplemented with 250 µg of vitamin B12 from 11 to 14 weeks of pregnancy through 3 months postpartum.26 In this study, women who were randomised to receive vitamin B12 also had an improved immune response to the pandemic influenza A (H1N1) vaccine.
The first 1000 days after conception are regarded as the most critical time for brain development. During this period, brain growth is rapid, increasing the susceptibility to influences from the environment.27 This is also the period when most of the myelination of the brain occurs.9 In infants, moderate and severe vitamin B12 deficiency has been associated with demyelination and brain atrophy.28 29 Little is known about the consequences of maternal vitamin B12 deficiency for early brain myelination, neurodevelopment and cognitive function.
Hypothesis to be tested
In Nepalese women, daily supplementation of 50 µg vitamin B12 from early pregnancy, not later than week 15, and until 6 months postpartum, improves linear and ponderal growth as well as cognitive, language and/or motor scores of the Bayley Scales of Infant and Toddler Development, Third Edition (Bayley-III) in their infants.
Specific objectives
Primary objectives
Measure whether daily maternal administration of 50 µg vitamin B12 from early pregnancy until 6 months postpartum improves cognitive, language and motor scores of the Bayley-III measured at 6 and 12 months of age.
Measure whether daily maternal administration of 50 µg vitamin B12 from early pregnancy until 6 months postpartum improves the infant’s z-scores length for age, weight for age and weight for length at 12 months.
Secondary objectives
Measure whether daily maternal administration of 50 µg vitamin B12 from early pregnancy until 6 months postpartum improves haemoglobin concentration of the mother and infant, and also assess the relationship between maternal and infant haemoglobin concentration on cognitive outcomes at 6 and 12 months of age.
Measure whether daily maternal administration of vitamin B12 from early pregnancy until 6 months postpartum improves cognitive function of infants as measured by the Bayley-III at 24 months of age.
Measure whether daily maternal administration of vitamin B12 from early pregnancy until 6 months postpartum improves development as measured by the Ages and Stages Questionnaire, Third Edition (ASQ-3), at 6 and 12 months of age.
Measure whether daily maternal administration of vitamin B12 from early pregnancy until 6 months postpartum improves motor function of infants as measured by the Test of Infant Motor Performance at 45 days.
Measure whether daily maternal administration of vitamin B12 from early pregnancy until 6 months postpartum reduces the risk of complicated deliveries.
Measure whether daily maternal administration of vitamin B12 from early pregnancy until 6 months postpartum reduces the risk of giving birth to a child small for gestational age.
Explore the efficacy of vitamin B12 on growth and development in various subgroups (defined before the randomisation code that links the group treatment to a study participant is broken).
Measure whether daily maternal administration of vitamin B12 from early pregnancy until 6 months postpartum alters sleep and activity patterns of the infant.
Measure whether daily maternal administration of vitamin B12 from early pregnancy until 6 months postpartum affects heart rate variability.
Methods
Study setting
The study site is located in Bhaktapur, 15 km east of the capital city Kathmandu. Bhaktapur city is an ancient city famous for its traditional temples and buildings. It is listed under Unesco world heritage and one of the main tourist attractions in Nepal. Bhaktapur is a homogenous community consisting mostly of practising mixed Hindus and Buddhists. It is a periurban agricultural-based community located 1400 m above sea level with a population predominated by the Newar ethnic group. In the Bhaktapur municipality, domestic migrant workers from diverse ethnic groups work in several carpet factories. The local climate is humid subtropical with a wet and hot season (monsoon) from May to August, and a dry and cool season from October to March. The annual average rainfall is 78.3 mm, and the temperature ranges from −2°C to 35°C. The majority of the residents in Bhaktapur consume foods grown in the community. Rice is the staple food. The eating pattern varies with season, workload in the field and availability of foods. A variety of local green leafy vegetables is widely consumed mainly in the winter and spring seasons.
Eligibility criteria
20 to 40-year-old pregnant women from early pregnancy, not later than 15 weeks pregnant;
residing in Bhaktapur municipality and surrounding areas in Bhaktapur district;
availability of informed consent.
Exclusion criteria
taking dietary or multivitamin supplements containing vitamin B12;
known cases of chronic disease under treatment such as tuberculosis, diabetes, hypertension, hypo or hyperthyroidism, pernicious anaemia, Crohn’s disease and current use of anticonvulsant drugs;
severe anaemia (haemoglobin concentration <7 g/dL); blood will be analysed for haemoglobin concentration immediately after collection at enrolment by using HemoCue;
suffering from any condition that requires treatment with vitamin B12 such as pernicious anaemia and strict vegans.
Intervention
The supplements are produced by GC Rieber Compact (Bergen, Norway). The vitamin and placebo tablets are, except for the cyanocobalamin content, identical in composition, taste, smell and appearance. The compositions of the tablets follow the recipe of the commercial product ‘Seven OceanS Emergency Ration.’ Each daily dose (placebo or 50 µg vitamin B12) also contains 31 kcal from the 6.95 g vehicle which mainly consists of dextrose and palm oil. First dose of supplementation will be given by research staff at the hospital, and mothers will then be instructed to properly store the supplements, and consume these every day preferably in the morning. During the weekly visits, our research staff will record consumption of supplement during the last 7 days including iron, folic acid and calcium, and also count the amount of remaining supplements. We will also record if there was vomiting after supplementation, and reasons why the supplements were not taken. During the antenatal visits or other visits at the hospital, the study gynaecologists will verify the compliance. Additionally, study supervisors will randomly select days (5% of total days) to make independent visits to participant’s mother's home in order to record compliance with supplementation.
Cointervention
All pregnant women will also be given folic acid (0.4 mg) for the first 2 months of pregnancy followed by iron (60 mg elemental iron) and calcium supplements (500 mg) until 45 days after delivery according to the WHO guidelines.30
Recruitment procedure, confirmation of pregnancy and assessment of gestational age
Prior and throughout the study period, we will identify pregnant mothers through a hospital and community-based surveillance system (figure 1). We have records of newly married couples in the study area that are updated quarterly. Information regarding pregnancies will be obtained monthly by household surveys or phone calls. Women with history of interrupted menstruation cycle or pregnancy detected by standard human chorionic gonadotropin kits, are screened in the hospital. In these women, pregnancy and gestational age is estimated by ultrasonography (USG). Follow-up USG is performed between 18 and 22 weeks for anomalies scanning.
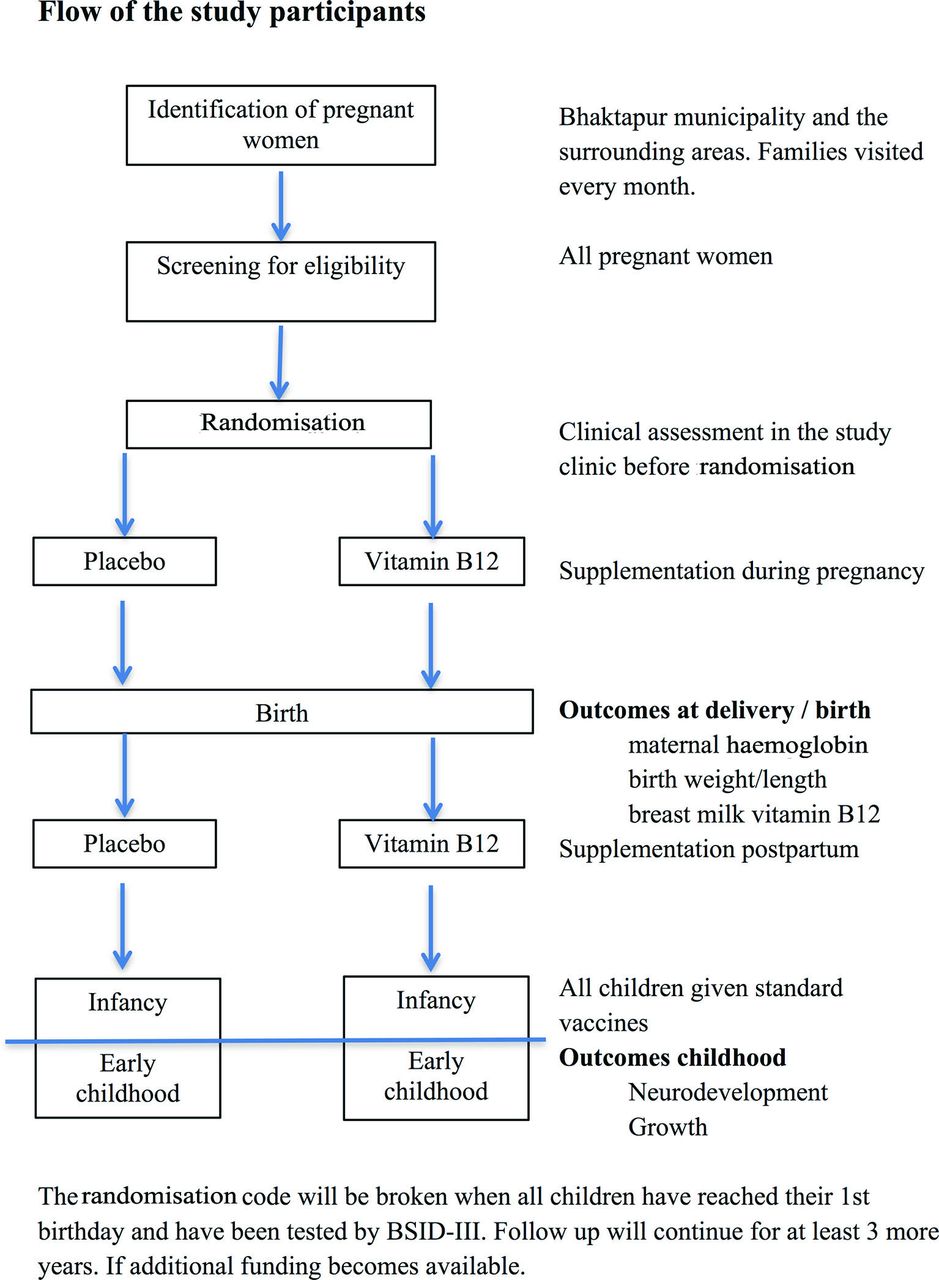
Study flow chart—recruitment, supplementation and follow-up plan. BSID, Bayley Scales of Infant Development.
After screening for eligibility, a detailed information regarding the study will be provided focusing on the duration, collection of biological samples and the follow-up plan of the study. The consent forms will be filled up by study gynaecologists or supervisors, preferably in the presence of the husband. A copy of the consent form along with the information sheets will be provided to each participant. In the consent form, there is a separate provision for consent of biological samples where the participants may agree or refuse. In case of illiterate participants, we will obtain thumbprints after getting signature from an impartial witness who is not part of research team.
Allocation, randomisation and blinding
The randomised allocation list was generated in STATA (Stata, College Station, TX) using the script ‘randomize’ (net from http://folk.uib.no/mihtr/stata/). We randomised the women in a 1:1 ratio in blocks of 8. Each woman is assigned a packet of supplementation according to her ID number which is sequentially numbered. This packet is only labelled with general information about the study and the unique ID number. The list that links the ID number to the randomisation code is kept with the company that produces the intervention and the placebo, and with the scientist who generated it who is otherwise not involved in the study. We will ensure allocation concealment throughout the study as none of the investigators will have access to this list until completion of data collection. This is only after the database with the main outcomes (growth and neurodevelopment scores) has been cleaned and locked, and after the plan of analysis for the main outcomes is finalised and approved by all involved scientists.
Rationale for choosing 50 µg dose of vitamin B12
Based on results from previous studies in this area, we expect the intake of vitamin B12 among women in our study to be low, both due to a predominant plant-based diet and poor gut function that again may disturb vitamin B12 absorption and increase dose requirements. Absorption of vitamin B12 is strictly regulated, and the body is not able to absorb more than 2–4 µg/day. The vitamin B12 supplementation study in pregnancy from South India24 and the study from Bangladesh26 used very high doses of 20–100× RDA with no reported adverse effects. There are other large RCTs where similarly high doses of vitamin B12 have been given together with other micronutrients.31 32 These studies found that the micronutrient mixture that included high doses of vitamin B12 reduced the risk for small for gestational age (SGA) with no adverse effects. In Europe and the USA, vegans and vegetarians are aware that there is a risk of B12 deficiency that can result in poor neurodevelopment and other adverse outcomes.33 Many therefore take additional supplements with similar high doses of B12 during pregnancy.
Timeline
The first participant in the study was enrolled in March 2017 and we plan to enrol for 2 years. End of follow-up of infants (for collecting primary outcomes) will be completed approximately 18 months after the last enrolment.
Laboratory procedures
From the mother, blood samples will be obtained at enrolment (baseline) and at the end of supplementation (6 months postpartum). In the infants, we will collect blood samples at 6 months by a trained lab technician with direct supervision of study paediatrician. Three millilitres of blood will be collected into vials containing EDTA as anticoagulant. The plasma will be centrifuged at approximately 700 g at room temperature for 10 min, separated and transferred into storage vials, and stored at −70° before analysis.
The blood samples will be analysed for the following:
Haemoglobin concentration by using HemoCue B immediately after blood collection (HemoCue, Vedbæk, Denmark).
Plasma vitamin B12 and plasma folate concentrations will be estimated by microbiological assays using a chloramphenicol-resistant strain of Lactobacillus casei and colistin sulfate-resistant strain of Lactobacillus leichmannii, respectively.
The plasma will be stored and used for other biomarkers (nutrients, markers of inflammation, epigenetic markers and markers related to neurodevelopment).
Follow-up
We keep track of the enrolled women in a Global Positioning System (GPS)/mobile-based surveillance system. Enrolled women will be visited every week in the period of supplementation and the fieldworker will ask questions about their physical condition, compliance among both study groups and adverse events (AE). The family/women are asked to inform us when they go into labour, and we will ensure transportation to hospital where they will give birth. This will also ensure that we get information about the pregnancy outcome. We will not try to influence the choice of place to deliver; however, we will encourage the women to deliver in a health facility rather than at home. In the Kathmandu Valley, less than 5% of deliveries are at home.
After delivery, we will follow-up the child at home every month until 2 years of age. We will collect information on breast feeding and complementary feeding (frequency, whether other drinks or solids/semisolids have been given). We will also ensure that the child receives standard vaccines as per the expanded programme on immunization schedule. Growth will be measured and dietary recalls undertaken every 3 months. Neurodevelopment will be measured at different time points during infancy.
Outcomes
Anthropometry
Weights will be measured with a portable electronic scale that measures to the nearest 0.01 kg (portable Seca weight). Height and length (portable Seca board) will be measured according to standard guidelines. Both length and weight will be measured in their homes immediately after birth and at 1, 3, 6, 9, 12, 18 and 24 months.
Neurodevelopment
With the exception of the Test for Infant Motor Performance (TIMP), all the planned assessment tools are currently in use in our ongoing studies in Nepal. Thus, the study benefits from the fact that the necessary translations, adaptations, piloting and psychometric evaluations have been completed for the study setting.
Bayley Scale of Infant and Toddler Development, Third Edition (Bayley-III) is a comprehensive assessment tool of developmental functioning in infants and toddlers aged 1–42 months.34 It is administered directly with the child and provides information on functioning in cognition, language (receptive and expressive), motor (fine and gross) abilities and social-emotional functioning. The Bayley-III is considered to be the gold standard in developmental assessment of this age group, and is widely used for research purposes worldwide. Summary scores of the Bayley-III cognitive, language and motor subscales at 6 and 12 months of age will be the primary outcome in the current study, while the assessment at 24 months will serve as secondary outcome.
The ASQ-3 is an easily administered checklist of developmental status standardised for children aged 1–66 months.35 The screening system includes age-appropriate questionnaires for every 2/3-month intervals. Each questionnaire contains 30 items in five domains: communication, gross motor, fine motor, problem solving and personal social. The questionnaires are designed to be completed by caregivers, but can also be administered by a trained examiner which will be done in the current study. Since the ASQ-3 is a screening tool developed to identify children at risk for delay, there is a possibility for a ceiling effect. To avoid possible ceiling effects, children who get maximum scores will be administered the next level checklist. We have used this tool in the current and at a similar study setting36 previously, and find the tool to be a feasible addition to the assessment of neurodevelopment in young children. The ASQ-3 will be administered in the homes of the families and provide us the opportunity to assess developmental trajectories.
Actigraph (the Actiwatch 2 (Philips)) is a wristwatch-like device that records motion data. Using a validated scoring algorithm, the Actiware software translates the activity data to sleep-wake patterns and activity level. Sleep problems and sleep patterns will be further corroborated by questionnaire data (the Brief Infant Sleep Questionnaire (BISQ)). The BISQ has demonstrated good psychometric properties as a brief sleep screening tool for clinical and research purposes in infants and toddlers (0–30 months).37
Heart rate variability (Vagal tone) is a marker of parasympathetic activity. Vagal tone has been suggested to be a sensitive marker of self-regulation and cognitive control and associated with the status of vitamin B12 during pregnancy,38 and may be an important subjective measure of early risk identifier of child development. We plan to measure the vagal tone at 3, 12 and 24 months of age.
TIMP is a test of functional motor behaviour which can be used up to 4 months of age.39 40 It consists of 42 items that are scored as present or absent based on observation. The TIMP has shown good predictive validity for later neurodevelopmental outcomes.41 We will pilot the test in the current study setting ahead of study start to ensure that it is appropriate for the study setting. Three psychologists and medical doctors will be trained through an online course and standardised to perform this test, which will be conducted when the children are 45 days to estimate early signs of effect of the maternal vitamin B12 supplementation.
Questionnaires/Inventories
The Home Observation for the Measurement of the Environment (HOME Inventory) is an internationally recognised tool for measuring both the quality and quantity of stimulation and support available to the child in the home environment. The tool has been used successfully in over 100 countries and validated in several low and middle-income countries.42 It consists of six subscales: parental responsivity; acceptance of child; organisation of the environment; learning materials; parental involvement; and variety in experience. A disadvantaged environment is among the many factors identified as influencing child cognition and development, and studies have demonstrated that the HOME Inventory is a predictor of later school achievement.42 Administration of the HOME Inventory requires both interviewing the mother as well as observing the household. It takes approximately 45 min to 1 hour to complete, and trained fieldworkers will conduct this assessment. Information about the child’s environment will be collected so that we can account for the effect on child development in our study.
The Caregiver Knowledge of Child Development Inventory (CKCDI) is a brief questionnaire to assess parental knowledge of child developmental milestones and knowledge of developmental stimulation.43 Parental knowledge on child developmental milestones may be of importance to promote adequate development in children. In this study, we will use the CKCDI in the third trimester and at 12 months postpartum to account for the effect of the caregivers’ knowledge on child development.
Self-Report Questionnaire (SRQ-20) is a screening of mental health developed by the WHO especially for low to middle-income countries.44 The scores on the SRQ-20 may serve different purposes in the current study. We can estimate the association between maternal depressive scores and child development, and in addition, we may investigate possible effects of maternal vitamin B12 supplementation on depressive symptoms.
Quality control of field activities
The fieldwork will be monitored by skilled supervisors, medical doctors, gynaecologists and qualified psychologists. For all outcomes, the study staff have received training before initiation of the project, and the staff will be used based on their skill level. For a specified proportion (5%) of the primary outcomes, a study supervisor or scientist monitors the worker's performance. Some of these assessments are also done independently. For example, when a fieldworker has measured the weight and length of a child, a supervisor or scientist will undertake the same measurement and compare their findings with that of the fieldworker. For all main outcomes, we compare the reliability and precision of each examiner with the reliability of a gold standard. For example, for measuring length we have training sessions where the fieldworkers and a gold standard measure each child twice. In a typical training session, each worker measures 10 children twice. The intraindividual variability (mean squared difference) of a trainee will be compared with that of the gold standard. For length measurements, we will accept no more than 50% higher intraindividual variability of the examiner compared with the gold standard. In this exercise, we can also compare the mean deviations of absolute differences between the gold standard and the worker. The mean deviation is also compared with the mean variability of the measurements of the gold standard. The deviation is also compared on a qualitative scale to assess whether there are systematic higher or lower readings. In case of poor agreement, extra training will be carried out until acceptable agreement was achieved.
Quality control for the neurodevelopmental tools
All methods that will be used to measure neurodevelopment have been translated, adjusted and/or piloted in previous studies at the current study site. The comprehensive neurodevelopmental tools such as the Bayley-III and TIMP will be administered by the medical doctors and psychologists. Medical doctors and qualified psychologists will train and monitor fieldworkers to perform the neurodevelopmental assessments such as the ASQ-3, HOME assessment and the various questionnaires. Ahead of study start, we will arrange training sessions. The trainings will be supervised and monitored by experienced psychologists from the Regional Centre for Child and Adolescent Mental Health and Welfare, Uni Research Health, Bergen, Norway. Standardisation exercises will be conducted measuring the inter-rater reliability of the assessor compared with a gold standard until satisfactory level of agreement. Video recording will be done for all Bayley assessments and 10% of the videos will be scored independently for quality control. For all other instruments, 5% of the assessments will be double scored. Once a month inter-rater reliability will be analysed for quality control.
Safety considerations, safety monitoring and AE reporting
All AEs and serious adverse events (SAE) will be recorded by the study staff. AEs are graded from 1 to 5 according to their severity according to Common Terminology Criteria for Adverse Events.45 All immediate AEs following each dose of intervention will be documented for all women.
All AEs will be followed up until resolution or stabilisation as judged by gynaecologist or paediatrician (site investigator) and the principal investigator. All SAEs will be followed up until satisfactory resolution or until the treating physicians and the principal investigator deem the event to be chronic or the participant to be stable.
SAE, which includes critical or life-threatening illness or death, will be documented from the time of enrolment throughout the study period. The pregnant women will be visited every week. During each contact, the study staff will collect data to ascertain SAEs and illness requiring hospitalisation. All SAEs of death, development of signs of critical illness and severe illness requiring hospitalisation, and AEs as described previously will be reported to the Ethics Committees, the Data and Safety Monitoring Board (DSMB) and to the sponsors of the study within 24 hours of awareness of the event, followed by a final report within 10 days. SAE’s relatedness to the administration of vitamin B12 or placebo will be judged by the investigator/designee, the Ethics Committee and the DSMB who will have access to all relevant investigations, clinical assessments and if require unblinding allocated interventions.
Data and Safety Monitoring Boards
The DSMB comprises a paediatrician, public health expert and a biostatistician. The DSMB is independent from the sponsor and has no competing interests. The DSMB members have prepared a charter and decided the study stopping rules, and will review the SAEs and AEs reported in the study periodically. They will examine all pregnancy complications, cases of severe illness, infant deaths and other SAEs to decide if the study should be continued, based on the predecided stopping rules. After one-third of the study participants have been enrolled and completed follow-up, the DSMBs will review the data and make recommendations concerning continuation, modification or termination of the study due to unexpectedly large beneficial effects or serious side effects and can suggest extension of the trial should the primary outcomes occur less often than anticipated. Any important protocol modification such as changes to eligibility criteria, outcome analyses will be thoroughly communicated with DSMB members and will obtain amendment clearance from the institutional review board (IRB).
Sample size calculations
We expect that as many as 15% of the enrolled women will be lost to follow-up because of abortions, stillbirths and migration (see table 1).
Expected losses to follow-up due to different conditions during the study period
We have calculated the sample sizes based on standard formulas46 to compare two means which are used in the ‘power’ function in STATA (Stata). For an effect size of .25 SD, we would need to analyse 676 infants to achieve a statistical power of 90% (p values of 0.05); we will therefore target 800 women–infant dyads (676/(1–0.15)). In these calculations, we assumed equal SD in the placebo and vitamin B12 groups. The power to detect differences between the study groups is larger than what is projected here as we will measure most of the outcomes more than once and also use these repeated measurements in the same analyses, adjusting for interdependence within a child using mixed effects models, generalised estimating equations or other appropriate methods. Various required total sample sizes according to meaningful differences and powers of 80% and 90% are depicted in figure 2.

{kind=link}
{kind=link}
Estimated required total sample sizes based on relevant effect sizes at 80% and 90% power.
These figures are based on national figures and our experiences from the field site. Infant morbidity and mortality are expected to be lower than national figures because of the proximity to the capital Kathmandu and because of our close follow-up.
Data management
All information will be collected in structured forms designed specifically for this project. A relational database has been designed. All forms are checked manually by the study supervisors before they are sent for computer entry. All data are entered twice by two different data operators within 1 week of data collection.
Data are stored in secure servers in the field office and in a data management centre (DMC) in Kathmandu. A substantial proportion of the forms is captured using iPads or similar tablets using the cloud-based data management system. We have used this electronic data capture system with success in many previous studies. Only computer data entry staff and supervisors will have access to the data. In the data system, the entered data are processed in several steps and the system will be designed to identify inconsistencies between different variables and different forms. The system can also detect entries that are out of range and notify when information is missing. This system also includes reminders about study activities, that is, the study staff will be notified when a birth or a scheduled vaccine is due. We are collecting GPS coordinates and phone numbers from several family members. By this, we can more easily reach the families and will probably reduce the numbers of missed home visits.
Data tracking, cleaning and quality checks
The DMC is also responsible for initial cleaning of the data. Interim tabulations and scatter plots for some variables will be made at regular intervals to identify data errors. Special checks are made on observations that are more than two or three SDs from the mean. There is a regular feedback of errors from the DMC to the study sites.
Record retention and archival
All the study documents including participant’s source data and documents will be archived by the study sites after the completion of the study, until the time the sponsor informs in writing to the study sites that they no longer need to maintain the study documents.
Plan of analysis
All analyses will initially be done on an intent-to-treat basis. All randomised participants will be included in the analyses if the relevant outcome variables have been collected. The main outcomes are continuous and expected to be normally distributed. We will use the Bayley-III scores at 6 and 12 months in separate analyses where B12 supplementation is the main exposure. We will compare the mean Bayley-III scores (scores on the cognitive, language and motor subscale scores, with the language scale analysed both separately for receptive and expressive language and as a composite measure, and the motor scale analysed both separately for fine and gross motor development and as a composite measure) between the vitamin B12 group and the placebo group. For growth, the main outcome will be measured when the child is 12 months. Linear growth, expressed as centimetres and height for age z-score (HAZ), and weight expressed as kilograms, weight for age (WAZ) and weight for height (WHZ) will be compared between the study groups. If baseline differences are observed, we will adjust these imbalances in multiple linear regression models, adjusted and unadjusted effect estimates will then be presented.
We will analyse the effect of vitamin B12 separately in the following subgroups:
Vitamin B12 status:
based on cobalamin (cut-off: 150 pmol/L)
based on low total homocysteine (cut-off: 10 µmol/L)
based on low methylmalonic acid (cut-off: 0.26 µmol/L)
Maternal body mass index (cut-off: 18.5)
Vegetarian (yes/no)
Birth weight (cut-off: 2500 g)
In these subgroup analyses, the differences in the effect between the levels of the subgroups will be measured by including two-way interaction terms in multiple regression models. Statistically significant effect modification will be when the p value of the interaction term is <0.05.
Per protocol analysis
In addition to a standard per protocol analysis, we will use instrumental variable analysis in an attempt to estimate the true effect of cobalamin had it been given to all women in the scheduled doses and intervals. The random allocation will be the instrument in these analyses. For per protocol analysis, women who receive less than 50% of the projected doses during pregnancy will not be included in the analyses, well acknowledging that the ensuing effect estimates may be biased and will certainly represent an effect higher than what can be achieved even in our well-resourced study setting.
Discussion
This proposed study measures the effect of vitamin B12 supplementation from early pregnancy through 6 months postpartum on early neurodevelopment and growth in 800 Nepalese infants at 6 and 12 months. Randomised clinical trials on vitamin B12 in pregnancy are called for as concluded in a recent systematic review and meta-analysis.22 This trial will add to the knowledge on the potential beneficial effects of vitamin B12 on pregnancy and perinatal outcomes.21 Our results can be used to inform both regional dietary guidelines for Nepalese and South Asian pregnant women. The recently published report ‘WHO recommendations on antenatal care for a positive pregnancy experience’ only recommends iron and folic acid to pregnant women,30 the results from our study may possibly contribute to necessary updates of these guidelines.
The primary concern raised by the Norwegian IRB was that this RCT was violating the principle of clinical equipoise. The IRB was accordingly concerned that we were withholding necessary vitamin B12 treatment for those who were randomised to the placebo. This concern was based on comments from an expert reviewer appointed by this IRB, and we are dealing with this concern, in part, by measuring functional motor behaviour by the TIMP when the children are 45 days in the first 100 children. If we find an unexpected beneficial effect of vitamin B12 on the results of this test, the DSMB will consider stopping the trial. The TIMP was added solely based on the concerns raised by the IRB, and this motor test will mainly be used as a tool for the DSMB when deciding whether the study should continue or not. It should also be noted that before approving our protocols, the IRB engaged a second external expert who did not share the concerns regarding clinical equipoise.
The Government of Nepal, in partnership with different organisations such as WHO and Unicef, has initiated many programmes in mother and child care. There are great concerns that many children in low and middle-income countries fail to reach their developmental potential due to poverty-related factors such as malnutrition, micronutrient deficiencies, parental illiteracy, and lack of stimulation and learning opportunities.47 Results from our study will provide a valuable contribution to the field of early risk and development in disadvantaged children and their families, and may also help to further integrate the Government of Nepal programme on the first 1000 golden days.
Acknowledgments
We thank the Siddhi Memorial Foundation in Bhaktapur for providing excellent facilities to undertake this study.
References
Footnotes
Contributors TAS, IK, MH and RKC conceived the study, and contributed to study design, sample size calculations and analytical plans. TAS, RKC, IK and MH drafted the manuscript. MU, RKC, TAS, MS, SB and LS initiated the project, have assisted in developing the protocol and helped with implementation. All authors read and approved the final manuscript.
Funding This study has been granted funding from the Centre of Excellence Scheme and the University of Bergen (UiB), Norway to the Centre for Intervention Science in Maternal and Child Health (CISMAC; project number 223269).
Competing interests None declared.
Patient consent Obtained.
Ethics approval National Health and Research Council, Nepal and the Regional Committee for Medical and Health Research Ethics of Western Norway.
Provenance and peer review Not commissioned; externally peer reviewed.