Article Text

Abstract
Objective Provision of a discharge care plan and prevention therapies is often suboptimal. Our objective was to design and pilot test an interdisciplinary, organisational intervention to improve discharge care using stroke as the case study using a mixed-methods, controlled before–after observational study design.
Setting Acute care public hospitals in Queensland, Australia (n=15). The 15 hospitals were ranked against a benchmark based on a composite outcome of three discharge care processes. Clinicians from a ‘top-ranked’ hospital participated in a focus group to elicit their success factors. Two pilot hospitals then participated in the organisational intervention that was designed with experts and consumers.
Participants Hospital clinicians involved in discharge care for stroke and patients admitted with acute stroke or transient ischaemic attack.
Intervention A four-stage, multifaceted organisational intervention that included data reviews, education and facilitated action planning.
Primary and secondary outcome measures Three discharge processes collected in Queensland hospitals within the Australian Stroke Clinical Registry were used to select study hospitals: (1) discharge care plan; (2) antihypertensive medication prescription and (3) antiplatelet medication prescription (ischaemic events only). Primary measure: composite outcome. Secondary measures: individual adherence changes for each discharge process; sensitivity analyses. The performance outcomes were compared 3 months before the intervention (preintervention), 3 months postintervention and at 12 months (sustainability).
Results Data from 1289 episodes of care from the two pilot hospitals were analysed. Improvements from preintervention adherence were: antiplatelet therapy (88%vs96%, p=0.02); antihypertensive prescription (61%vs79%, p<0.001); discharge planning (72%vs94%, p<0.001); composite outcome (73%vs89%, p<0.001). There was an insignificant decay effect over the 12-month sustainability period (composite outcome: 89% postintervention vs 85% sustainability period, p=0.08).
Conclusion Discharge care in hospitals may be effectively improved and sustained through a staged and peer-informed, organisational intervention. The intervention warrants further application and trialling on a larger scale.
- stroke
- quality in health care
- clinical audit
- change management
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Hospitals offer the ideal environment to instigate individualised prevention management strategies for chronic conditions with a high risk of recurrence, such as stroke. However, few effective interventions are available to improve recommended and high-quality discharge care. A strength of this research is that is has begun to fill this important knowledge–practice gap.
The organisational intervention was carefully designed using theory, evidence, involvement of consumers and a broad range of clinical and implementation sciences experts.
Standardised and routinely collected data from a national clinical quality registry were used to ensure reliable comparisons over time, including ability to measure the long-term sustainability impact, the new frontier in quality improvement.
The effectiveness data (n=1289 episodes of care) were obtained from two hospitals and trialling in a larger number of hospitals to confirm the findings is needed.
Similar to other non-randomised studies, there is the potential for reporting and response bias.
Introduction
In terms of the total global burden of disease, neurological disorders combined with cerebrovascular disease represents 7.1% for all causes and ages.1 Stroke contributes to the majority of this burden, and similar to other chronic neurological conditions, patients are hospitalised for acute treatment. A hospital provides the ideal environment in which to instigate individualised prevention management strategies for chronic neurological conditions with a high risk of recurrence, such as stroke where the cumulative 10-year risk is about 40%.2 3
Because of the sudden impact of chronic disability that may be a consequence of stroke, comprehensive discharge planning, that involves the patient and family, is recommended to facilitate transition back into the community. The objective of interdisciplinary and formalised discharge planning is to reduce length of stay, improve the coordination of services following discharge and avoid readmission and long-term unmet needs.4 5 Unfortunately, evidence from national stroke audits and the Australian Stroke Clinical Registry (AuSCR) consistently show that less than three in five patients receive a discharge care plan or behavioural prevention education from clinicians, and prescription of prevention medication is suboptimal.6 7 This is despite the availability of standardised tools to help clinicians undertake these activities more efficiently in Australia such as the Stroke Foundation's ‘My Stroke Journey’ discharge pack that comprises an education booklet and care planning guide.8 A better understanding of clinician and hospital factors related to discharge care is needed to support the development of more effective interventions that target clinician practice to ensure optimal discharge care.9 10
The aims of this study were to design and pilot test an interdisciplinary, organisational intervention to improve discharge care using stroke as the case study. In particular, we sought to determine the preliminary effectiveness of the new intervention using routinely collected data from the AuSCR by comparing preimplementation and postimplementation adherence results (combined as a composite outcome and for individual processes of care) and the change in performance relative to benchmarks established for these processes across the different measurement periods (ie, referred to here as a change in performance gap score). We also sought to measure sustainability of any improvements over a 12-month time period, as sustainability outcomes are rarely reported.11–13 The primary outcome was the net change in the overall composite outcome and secondary outcomes were changes in individual scores and the gap score. Further details are provided below.
Methods
The description and reporting of our intervention is based on the Standards for QUality Improvement Reporting Excellence 2.0 guidelines to promote completeness of information, transparency and potential for replication in the field.14
Context
Acute care public hospitals located in Queensland and using the AuSCR for performance monitoring were the setting for the intervention. Discharge care involves different health professionals.5 In acute hospitals, where there is a high turnover of beds and short lengths of stay (average for stroke is about 5 days),7 omissions may occur. Designing interventions for achieving behaviour change can be challenging when health professionals are time poor or where roles and responsibilities for different aspects of care are shared. Furthermore, it remains unclear if multifaceted organisational interventions are more effective than single-component interventions or whether there is a dose–response relationship.15
Intervention development and design
This was a mixed-methods study that was iteratively undertaken whereby results of each stage were reviewed to inform the next stage.16 The basis of the intervention was to use external facilitation to raise awareness of areas of underperformance with local clinicians and workup strategies to leverage enabling factors and reduce barriers to successful implementation of the discharge processes relevant to the local context. The intervention development and pilot testing occurred over a 5-month period. A summary of each phase is provided below with additional detail provided in the online Supplemental methods.
Supplementary file 1
Preintervention design phase: understanding what works well at ‘top-performing’ hospitals
We included a preintervention design phase whereby two hospitals with the greatest adherence to the discharge processes were selected to provide information on the factors that made provision of discharge care successful at their site. These were defined as ‘top-performing’ or ‘exemplar’ hospitals. Qualitative data from these exemplar hospitals were subjected to thematic analysis and the factors that were found to influence adherence to the clinical care processes were mapped across the 14 domains of the theoretical domains framework (TDF).17 18 This provided a conceptual basis for describing the enablers and barriers to implementation.
Intervention design phase
The intervention was designed using complementary knowledge translation concepts and theory including elements of the ‘Promoting Action on Research Implementation in Health Services’ (PARIHS) framework, transtheoretical model of change; the plan–do–study–act method and the Ottawa model of research use.9 19–22 In an attempt to fast track strategy development at the pilot hospitals, successful techniques reported from the ‘exemplar’ hospitals were shared (online supplemental results, table I). An expert working group (n=9) that included decision-makers, clinicians, experts in knowledge translation and consumer representatives finalised the intervention with the project team via one face-to-face workshop and two teleconferences.
The final intervention, known as STELAR (Shared Team Efforts Leading to Adherence Results), was delivered in four discrete stages: pre-workshop survey (to gain a better understanding of current discharge processes and practices); two facilitated workshops (workshop 1: to discuss aspects of existing practices and gather consensus on the potential barriers that could be modified; workshop 2: an education component delivered by a ‘local opinion leader’ followed by a review of local AuSCR performance data by the external facilitator (DAC) and then development of a local action plan and appointment of a local ‘change champion’ who would facilitate implementation of the agreed strategies. The strategies aimed to maximise use of existing resources and processes, rather than increasing staff workloads) and ongoing telephone/electronic support by the programme team for 2 months after the second workshop. During this time, retraining in AuSCR data collection processes was also provided, as required. (figure 1 and online supplemental methods, figure I). A staged approach was used to improve knowledge of capability, motivation and opportunity within the settings, which have been recognised as fundamental to understanding the targeted behaviours.23 In brief, the delivery mechanisms included external facilitation; performance feedback with a gap analysis and a codesigned educational meeting using a local opinion leader, evidence from exemplar hospitals and a structured action planning activity. Participants were hospital staff involved in delivering the discharge processes including medical, nursing, pharmacy and allied health clinicians to be identified by the local opinion leader. The majority of these delivery mechanisms were informed by the literature.17 19 24
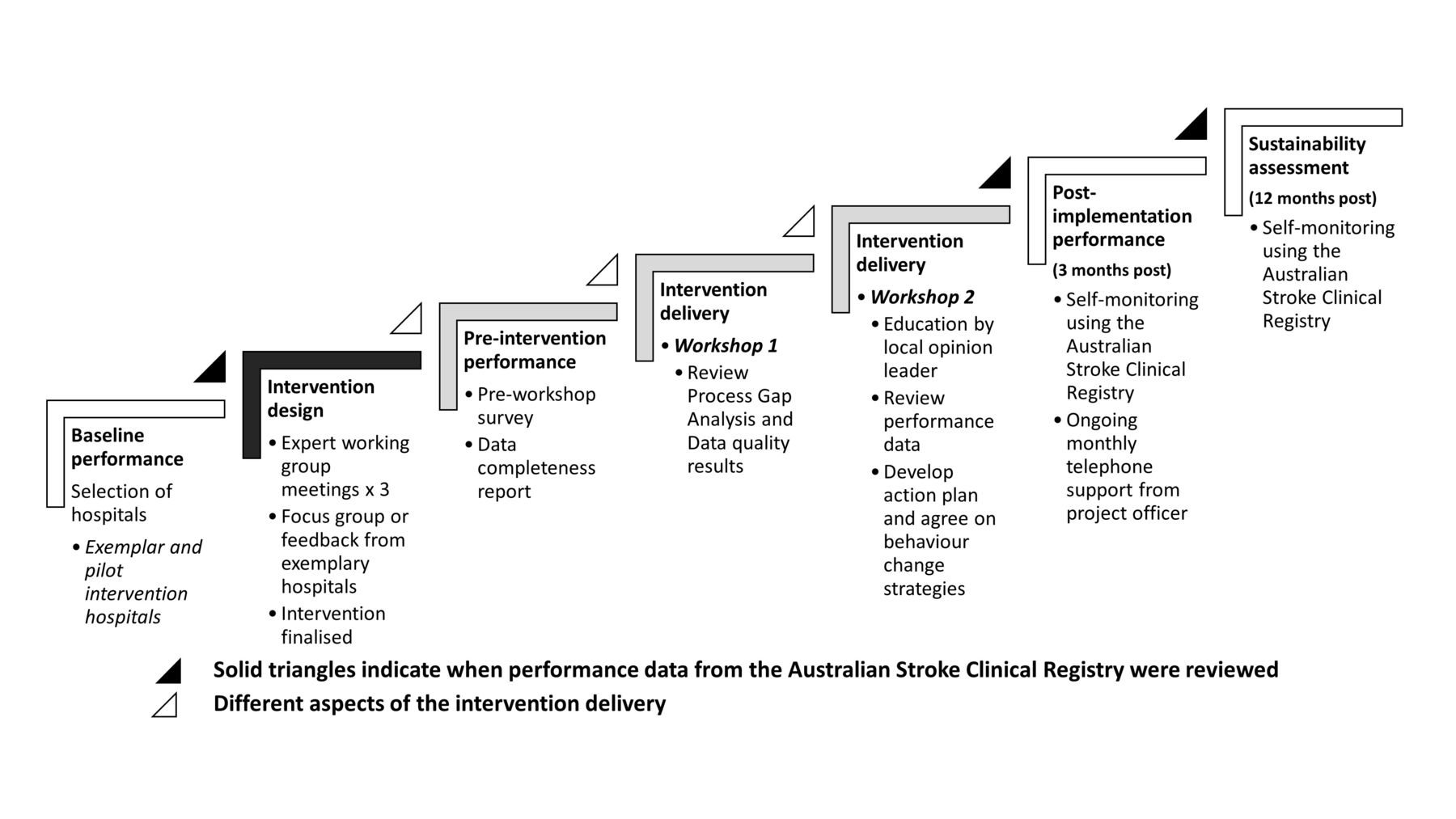
Project stages and evaluation periods.
Measures of intervention effectiveness
Hospital performance was measured using patient-level data entered into the AuSCR by clinicians at participating hospitals using a standardised approach.25 In brief, all patients admitted to hospital with stroke or transient ischaemic attack (TIA) are eligible to be included in this national clinical quality registry and an opt-out procedure is used, or waiver of consent for people who die in hospital, to reduce selection bias. Clinical performance data collected in relation to discharge care as part of the AuSCR in Queensland are: (1) provision of a discharge care plan developed with the interdisciplinary team and the patient and/or family; (2) prescribed antihypertensive medication at discharge from hospital or (3) if an ischaemic stroke or TIA, prescribed antiplatelet/anticoagulant medications at discharge from hospital.7 For a full description refer to online supplementary table II .
The primary effectiveness outcome used in this study was a composite score of adherence to each of the three discharge processes combined from both hospitals (referred to as the overall composite outcome). Adherences to individual processes were also evaluated, as was adherence relative to benchmarks for each of the processes and the composite outcome (referred to as performance ‘gap’ score) (see the Data analysis section and online supplementary figure II). Results from individual hospitals and in combination are presented.
Selection of hospitals
Public hospitals in Queensland that had registered at least 20 patients in the AuSCR between January 2012 and June 2013 were eligible (n=15; 82%). The two exemplar hospitals were chosen from sites that fell within the top 20th percentile for the composite gap score.
To pilot test this new intervention, we selected two hospitals that would benefit from improvement in adherence to these care processes (referred to here as ‘pilot hospitals’) and these were chosen from sites that fell within the bottom 20th percentile (online supplemental methods, figure III). One and half years of data were used to ensure that we identified sites with consistently high or low levels of performance. We also interrogated the data from the selected pilot sites to ensure that their results were not an artefact of missing or poorly entered data. As more than two hospitals met the criteria, hospital selection was also based on: relative performance across the individual care processes; the extent to which the hospital was representative of other similar hospitals to improve the generalisability of the results and ability to participate within our project time frame. Stroke unit medical directors of the eligible hospitals were sent an invitation letter in January 2014 and then consent to participate was obtained.
Ethical considerations
The project was approved by the Metro North Hospital and Health Service, The Prince Charles Hospital Human Research Ethics Committee (HREC/13/QPCH/279, November 2013) and governance approval was obtained from each participating hospital. Approval for the project was also granted by the AuSCR Research Task Group and governance committees.
Data analysis
Assessment of hospital performance for discharge care
Adherence of each hospital to the care processes was calculated as the number of patients who received the discharge process divided by the number of patients who were eligible for the care process. The composite outcome was calculated as the total number of patients who received the three discharge processes divided by the total number of patients eligible to receive the three care processes. Benchmarks were also calculated for each care process, based on a modified version of the Achievable Benchmarks of Care approach26 previously used in stroke by Hall et al,27 whereby the benchmark is calculated using at least 15% of the data.
The benchmarks were then used to calculate a gap score for each hospital for each discharge process and the composite outcome. To calculate this, adherence scores were divided by the relevant benchmark to provide the gap score (eg, if a site had an adherence score of 40% and the benchmark was 80%, the gap score would be 50% as they would be halfway towards meeting the benchmark) (online supplementary figure II provides an overview of the equations used). Separate benchmarks were calculated, using data from all 15 hospitals, for deriving the gap scores for each evaluation period. This approach accounted for the potential influence of other quality improvement activities being undertaken in Queensland between the different time periods used in the analyses and secular trends, as well as reducing issues of ceiling effects associated with individual care processes.
Changes in performance over time
Analysis of patient-level AuSCR data was used to determine the effectiveness of the intervention applying a historically controlled before–after design comparing the composite outcome scores. Time periods compared were: 3 months prior to the commencement of the intervention (preintervention period January to March 2014); 3 months after workshop 2 (postintervention period, October to December 2014) and 12 months after the postintervention period to assess if the programme had sustained effects (sustainability period, October to December 2015). Logistic regression was used to obtain ORs related to the proportion of patients who received each of the individual care processes at a site level. For the combined scores, we used multilevel analysis, with the levels defined as patient and hospital, to adjust for correlations between patients within hospitals. A secondary analysis was performed comparing the gap scores, and a sensitivity analysis was also performed to describe the differences between the baseline period (January 2012 to June 2013) and postintervention period (October to December 2014).
Descriptive statistics including Χ2 tests for comparisons of proportions between the different evaluation periods were used. Level of significance was set at p<0.05.
Results
Each invited hospital agreed to participate. Overall, 1298 episodes of care from the two pilot sites were included in the analysis (pre=419; post=438 and sustainability=432). Both pilot sites had a stroke unit which included co-located beds within a geographically defined ward staffed by a dedicated, multidisciplinary team with expertise in stroke. Site 1 was a 400-bed hospital and a regional hub for three small referring rural hospitals (catchment population 400 000). Site 2 was a 530-bed regional hospital providing services for a population of approximately 240 000 people, as well as tertiary-referral services for another 670 000. Site 1 admits approximately 450 patients with stroke and TIA per annum and site 2 admits approximately 250. Both offer a 24/7 thrombolysis service. Site 1 has a rapid-access TIA service staffed by a multidisciplinary team which can provide early rehabilitation. Both pilot hospitals have access to subacute and inpatient rehabilitation services. These hospitals are typical of most hospitals in Queensland contributing data to AuSCR.
Table 1 provides a summary of identified modifiable barriers that were common to both pilot hospitals, broadly described based on need for evidence, the context of care or where facilitation might be required. Common themes included habituation of practice and awareness of practice gaps. More specifically, inconsistent use of existing tools and systems, lack of pharmacist involvement as part of interdisciplinary care, inconsistent procedural knowledge associated with discharge planning, such as clinicians making assumptions about patient eligibility independent of other evidence, and suboptimal recording of data in the AuSCR and medical records were consistent areas identified for improvement. Importantly, it was recognised that existing processes and administrative systems could be leveraged by changing workflow processes. Common strategies included providing an example of a comprehensive discharge care plan for clinicians to refer to, using reminders (such as stickers in medical records) to facilitate prescription of medications, and regular reviews of data at team meetings. The health professionals also planned to empower patients and their families to use the My Stroke Journey 8 pack that was to be provided at time of admission to promote more effective and collaborative discharge care planning. There was recognition that when such interactions with patients and families occurred, this needed to be documented.
Common modifiable barriers in discharge practices identified at the pilot hospitals during workshop 1
Intervention effectiveness
Patient characteristics were generally similar from the participating hospitals relative to the non-participating hospitals during the preintervention and postintervention periods (online supplementary table III). Some exceptions were ability to walk on admission (site 2: pre 25%, post 75%, p<0.001 site 1: pre 50%, post 35%, p=0.04). The median age preintervention was 76 (Quandrant (Q)1 25th percentile: 67, Q3 75th percentile: 84) at site 1, 66 at site 2 (Q1: 58, Q3: 77) and 73 (Q1: 61, Q3:81) for the other Queensland sites combined. The proportion of women in the preintervention period was 43% for site 1, 44% for site 2% and 42% for non-participating sites, and the proportion of ischaemic stroke were 71% for site 1, 67% for site 2% and 68% for non-participating sites. There were some differences in discharge destinations with site 1 commencing initial subacute care within the stroke unit in approximately one-third of patients compared with none at site 2%, and 7% of non-participating sites.
Overall, the postintervention composite outcome (89%) significantly improved compared with the preintervention result from pilot sites (73%; p<0.001). This was mainly attributable to greater provision of discharge care plans which had the greatest scope for improvement (72% preintervention vs 94% postintervention) (table 2). Sustainability was achieved for all but one care process (prescribed antiplatelet therapy at discharge) which had a significant 7% reduction in adherence at 12 months after the intervention. A small non-significant reduction of 4% in the composite outcome occurred at 12 months (89% postintervention vs 85% at 12 months) representing the decay effect. Significant overall improvements were also achieved when the overall benchmark-derived gap scores were compared for the composite outcome (preintervention composite gap score 85% vs postintervention 94% p<0.001) and maintained during the 12-month sustainability period. Other results on the changes in different gaps scores are provided in online supplementary table IV.
Adherence to discharge processes before and after intervention implementation and 12 months after the intervention period
Despite overall improvements in the composite outcome and individual care processes, there were variations in the magnitude of improved performance between the pilot sites following the STELAR intervention (table 2). Results from our sensitivity analyses comparing the baseline (hospital selection period) composite outcome and postintervention outcomes showed much greater improvements than comparisons between the preintervention and postintervention periods, and in contrast to the non-participating hospitals (site 1, baseline composite outcome 37%; postintervention 86%, p<0.001 and site 2, baseline composite outcome 44%; postintervention 93%, p<0.001) (figure 2 and online supplementary figure IV).

{kind=link}
{kind=link}
Overall changes in adherence across different time periods for the pilot sites and non-participation hospitals. STELAR, shared team efforts leading to adherence results.
Discussion
Changing clinician behaviour to improve patient care will ultimately lead to better patient outcomes.10 19 24 28 The results from this project provide promising data on a new, theory and evidence-informed, multifaceted organisational intervention for improving discharge care after hospitalisation for acute stroke. Overall, significant and sustained improvements in adherence to the discharge processes were demonstrated following implementation of the STELAR programme. The net change in the composite outcome increased 16% after implementation with a non-significant decay effect at 12-month postimplementation (12% improvement compared with the preimplementation result or 4% decay effect). This case study in stroke is relevant to other neurological chronic conditions and provides information to support clinicians in how to design or deliver an organisational intervention that can be tailored to the local context.
The final design of the intervention included several stages since knowledge translation for healthcare professionals is more likely to be successful if stakeholders are involved in the process; readiness for change is achieved and the approach is informed by an assessment of the likely barriers and facilitators.10 29 Each pilot site had a change champion appointed, and we also used a local opinion leader to deliver the educational component of the face-to-face workshop. This is because local opinion leaders can influence rapid uptake of evidence.18 Similar to other authors,30 we found mapping the reported barriers and enablers to the TDF18 and corresponding behaviour change techniques17 to be a comprehensive approach to support targets for inclusion in an effective intervention. A particularly novel aspect was using experience from ‘exemplar hospitals’ to inform selection of strategies for inclusion in action plans.
The results are encouraging and accord with the most promising effect sizes for similar types of interventions reported in systematic reviews.10 24 If this intervention is considered a form of ‘audit and feedback’ methodology, then the feedback component we provided was consistent with the literature on the most effective methods for achieving a large effect. Feedback may be more effective when baseline performance is low; the provider of the feedback is a supervisor or a colleague; the data on performance are provided more than once and in verbal and written formats; and when it includes explicit targets and an action plan.19 Each of these elements was used in STELAR and provides further evidence that an absolute risk difference of 16%, consistent with the reported upper IQR from the included studies in the Ivers and colleagues’ review,19 is reproducible.
Strengths of our study include use of routinely collected and standardised data available from an established national clinical quality registry, the AuSCR, which facilitates routine and prospective monitoring and quality improvement.31 Importantly, we also incorporated reporting of sustainability, the new frontier in quality improvement.11 12 The programme was informed by the literature including relevant theoretical frameworks and systematic reviews of effective strategies to achieve clinician behaviour change. Each of the theoretical frameworks we used included the common elements of performance review against the evidence; and barrier management that takes into account local context or attempts to assess or account for the level of adoption.9 32 33 Previous authors have summarised the factors needed for successful knowledge translation, which include preparing for change, capacity for implementation including people and setting, resources, leverage, desirable implementation enabling features and achieving sustainability.34 Importantly, our design provided the possibility to align intervention components with the transtheoretical model of behaviour change: precontemplation (site identification—awareness raising), contemplation (recognising the gaps and considering possible causes (workshop 1)), preparing for action (action plan and change champion appointed), action (action plan implementation with external support) and maintenance (sustainability review) of change.22
Limitations included the potential for bias associated with observational studies, including reporting and response bias. Despite strong engagement with, and uptake of, the intervention at both sites, variability in the degree of change in adherence to the care processes at each site postintervention was noted (net change in composite outcome site 1: 7% and site 2: 33%). This may have been partly due to ceiling effects for some of the processes and the time delay between enrolment (when sites were made aware of potential for underperformance) and commencement of the interventions. This meant that sites were aware of the project 2 months prior to the start of the baseline data collection period and 9 months prior to the commencement of the intervention. Both sites had improved adherence between the baseline (hospital selection) and preintervention phase (net change in composite outcome site 1: 42% and site 2: 16%). Although we did not openly disclose if the hospital was an exemplar or pilot site at the time of the initial invitation, all could access online summary performance reports from the AuSCR at any time. The invitation may have prompted them to review their data. Other external factors such as presentation of data at the annual Queensland Stroke Clinical Network Forum in November 2013 may also have motivated efforts to improve discharge care, as the benchmark thresholds increased over time. If ‘awareness raising’ (invitation at baseline period) had been accounted for as part of the intervention, the overall results would have been more pronounced as demonstrated in the sensitivity analysis (both sites shifted 49 percentage points from baseline (invitation) to postintervention). Encouragingly, further improvements occurred and by the end of the study, both pilot sites were among the top-performing hospitals in Queensland for the measured care processes. We also acknowledge that the low baseline scores for the intervention pilot sites may have resulted in some regression towards the mean in our results. However, the magnitude of change in our pre-scores and post-scores was large and so would have been unlikely to have impacted on the significance of our results. We also acknowledge that type 1 errors from testing of multiple associations or outcomes may be possible, but given our large effect sizes (>2) and our small p-values, type 1 errors in our primary outcome, change in the combined composite score, are unlikely.35
In the area of stroke and other neurological conditions, few examples of interventions designed to effectively change clinician behaviour exist. These include multifaceted interventions such as the Get-With-The-Guidelines-Stroke programme36 37 and the Quality in Acute Stroke Care Trial that was a nurse-led intervention to improve management of fever, sugar and swallowing in acute stroke units through use of protocols.38 39 Similarly, there is a paucity of evidence for the hospital setting on the sustainability of practice improvement programmes. In a recent scoping review, only seven studies of programme sustainability had been conducted within a hospital environment.11 In our future planned work, it will be important to determine if this proposed STELAR intervention is reproducible in more hospitals, and can be extended to other care processes. We are currently undertaking a step-wedge designed study among 12 hospitals located in Victoria (Australia) where this type of intervention has not previously been used following funding obtained from the Ian Potter Foundation in 2016.
In conclusion, improving discharge care in hospitals through a staged, evidence-based, multifaceted intervention was effective and sustainable, and further testing of the intervention in more hospitals would be worthwhile. Importantly, we drew on the cumulative experience from the growing field of knowledge translation to design a programme for stroke, where little previous research has been undertaken. This research is relevant to other clinical domains, where variation in practice for discharge care is widespread.
References
Footnotes
Contributors DAC: conceptualisation and design of the study, drafting of the manuscript and interpretation of the data. NEA: drafting of the manuscript, literature review, analysis of data and interpretation of the data. ESS: revisions to the manuscript, contribution to literature reviews, study coordination and interpretation of the data. KH: revisions to the manuscript, contribution to intervention design and methods, and interpretation of the data. SM: revisions of the manuscript, contribution to intervention design and methods, and interpretation of the data. EH: consumer representative, revision of the manuscript, contribution to intervention design and methods, and interpretation of the data. IM: revisions to the manuscript, contribution to intervention delivery and interpretation of the data. SK: revisions to the manuscript, contribution to focus group and interpretation of the data. MRN: revision of the manuscript, contribution to intervention design and interpretation of the data. RG: revisions to the manuscript, contribution to intervention design and methods, and interpretation of the data.
Funding The Nancy & Vic Allen Stroke Prevention Fund supported this project which was also supplemented by grant funds from the National Health and Medical Research Council (NHMRC; 1034415). DAC (1063761 co-funded Heart Foundation) and NEA (1072053) received Research Fellowship support from the NHMRC.
Competing interests None declared.
Ethics approval Metro North Hospital and Health Service, The Prince Charles Hospital, Human Research Ethics Committee (HREC/13/QPCH/279, November 2013).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Unpublished programme evaluation data from this study may be available for mutually agreed use by contacting the corresponding author.