Article Text

Abstract
Objectives To investigate whether changes in psychosocial and physical working conditions are associated with subsequent psychotropic medication in ageing employees.
Methods Data were from the Helsinki Health Study, a cohort study of Finnish municipal employees, aged 40–60 years at phase 1 (2000–2002). Changes in psychosocial and physical working conditions were measured between phase 1 and phase 2 (2007). Survey data were longitudinally linked to data on prescribed, reimbursed psychotropic medication purchases (Anatomical Therapeutic Chemical) obtained from the registers of the Social Insurance Institution of Finland between the phase 2 survey and December 2013 (N=3587; 80% women). Outcomes were any psychotropic medication; antidepressants (N06A); anxiolytics (N05B); and sedatives and hypnotics (N05C). Cox regression analyses were performed.
Results During the follow-up, 28% of the participants were prescribed psychotropic medication. Repeated exposures to low job control, high job demands and high physical work load were associated with an increased risk of subsequent antidepressant and anxiolytic medication. Increased and repeated exposure to high physical work load, increased job control and repeated high job demands were associated with subsequent sedative and hypnotic medication. Age and sex-adjusted HR varied from 1.18 to 1.66. Improvement in job control was associated with a lower risk of anxiolytic, but with a higher risk of sedatives and hypnotic medication. Decreased physical work load was associated with a lower risk of antidepressant and anxiolytic medications.
Conclusion Improvement in working conditions could lower the risk of mental ill-health indicated by psychotropic medication.
- mental health
- longitudinal studies
- work stress
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Unlike previous studies, we were able to examine changes in both psychosocial and physical working conditions.
Data were derived from a well-characterised occupational cohort, which was deterministically linked to administrative medication records.
The use of register-based medication data allowed us to remove the prevalent cases and helped avoid the problems related to use of self-report measures such as recall and common method bias.
Due to relatively long interval between the two working conditions measurements, the study could have underestimated the effect of changing working conditions on subsequent psychotropic medication.
We did not have information about the clinical indication the examined medication was prescribed for.
Introduction
Mental ill-health is a growing concern in working populations.1 Adverse working conditions have been proposed as potentially modifiable risk factors for mental ill-health.2 Indeed, there is evidence that exposure to adverse psychosocial working conditions including low job control and high job demands are associated with an increased risk of mental ill-health.3–7 However, the majority of earlier studies have measured both exposure and outcome using self-reports, which can lead to inflated associations and common method bias.8 Other studies have avoided these problems by using register-based outcomes such as psychotropic medication, which is a commonly used marker of mental ill-health in a population.9–14
Most of the earlier studies have assessed exposure to adverse working conditions only at one time point, and there is a paucity of large-scale studies examining the association between changes in psychosocial working conditions and mental ill-health. Of a few studies that have separately assessed the effects of changes in job control and job demands on mental ill-health, three found that adverse changes in job demands had a stronger effect on the risk of self-reported mental ill-health than adverse changes in job control, whereas positive changes in these domains did not result in improvement in mental health.5 15 16 In a recent study, within-person increase in job control was associated with better self-reported mental health17; and in another study, both improvements and deterioration in job demands and job control predicted change in mental health.18 However, studies assessing the association between changes in job control and job demands and a more objective measure of mental ill-health, such as recorded psychotropic medication, are lacking.
Moreover, psychosocial working conditions have dominated the discussion about the work-related determinants of poor mental health, even though there is also evidence that physical working conditions are associated with mental ill-health. In the present cohort, increased and repeated exposure to repetitive movements and repeated exposure to awkward postures and rotation of back was associated with an increased likelihood of common mental disorders,16 desktop work was associated with purchases of sleeping pills among women,19 and computer work was a risk factor for disability retirement due to mental causes.20 In another study, deteriorating physical working conditions increased perceived mental strain.21 A review of the impact of working environment on mood disorders discussed the potential mechanisms; however, actual studies conducted in employee cohorts were rare.22 In a study among blue-collar workers’ exposure to noise intensified anxiety and depression in women.23
We set out this study to examine the associations between changes in psychosocial and physical working conditions and subsequent psychotropic medication.
Methods
Data
The data came from the Helsinki Health Study, which is a cohort study designed to investigate social-related and work-related determinants of health and well-being.24 The target population was the staff of the City of Helsinki, Finland. Phase 1 questionnaire surveys were collected in 2000, 2001 and 2002 among employees turning 40, 45, 50, 55 or 60 each year (N=8960, response rate 67%; 80% of participants women). Phase 2 survey data were collected in 2007 (N=7332, response rate 83%). Earlier non-response analysis showed that the participants broadly represent the target population.24 Survey data were linked to national records using a unique personal identification number for those respondents who had given written consent for the linkage (74%; N=6498). Consenting for the data linkage followed a similar pattern as the non-response, except that men provided consent slightly more often than women.24 25
In the present study, of those who consented to linkage, only participants who were still employed at phase 2 were included (N=4207). Men, manual workers and those who reported common mental disorders at phase 1 had slightly more often left the employment between the two phases (all p values <0.01, data not shown). Because of the age structure of the cohort, the majority (86%) of those who replied at phase 2 and stated that they were not employed had retired.
In addition, we excluded those with purchases of psychotropic medication in 3 months preceding phase 2 (n=337 for any psychotropic medication). Finally, we excluded those participants who had missing values for any of the study variables (n=283). The exclusions resulted in a final analytic sample of 3587 participants for the analyses examining any psychotropic medication.
Ethics
The Helsinki Health Study protocol was approved by the Ethics Committees of the Department of Public Health, University of Helsinki, and the health authorities of the City of Helsinki. The study conformed to the principles embodied in the Declaration of Helsinki.
Measurements
Working conditions
We used a version of Karasek’s Job Content Questionnaire26 to measure job control and job demands. Job control was assessed by nine and job demands by five items. The job control scale included items measuring skill discretion and decision authority. Job demands items assessed workload and work pace. Missing values were replaced by item modes for those having responded to at least eight job control and four job demands items, respectively. Job control and job demands were both dichotomised at the median.9 27
Physical work load, that is, uncomfortable postures, repetitive trunk rotation, repetitive movements, heavy physical exertion and lifting and carrying heavy loads, was assessed with an 18-item instrument developed at the Finnish Institute of Occupational Health.28 Missing values were replaced by item modes for those having responded to at least 14 items. Factor analysis showed that the questions loaded on three factors, of which the first one was interpreted to best measure physical work load. The items with the largest positive standardised scoring coefficients were the following: awkward working positions; rotation of the back; repetitive movements; and heavy physical effort or lifting and carrying heavy loads. Physical work load factor score was dichotomised at the highest quartile.29
Changes in psychosocial and physical working conditions were measured by a four-category variable for each of the three exposure variables: (1) repeated low exposure (low exposure at phase 1 and at phase 2); (2) increased exposure (low exposure at phase 1 and high exposure at phase 2); (3) decreased exposure (high exposure at phase 1 and low exposure at phase 2) and (4) repeated high exposure (high exposure at phase 1 and at phase 2).30
Psychotropic medication
Data on psychotropic medication were derived from the Finnish Prescription Register. This register is maintained by the Social Insurance Institution and it includes records of all prescribed psychotropic medication purchases reimbursed to Finnish residents in non-institutional settings. For each dispensed drug, the record includes the dispensing date, the WHO Anatomical Therapeutic Chemical (ATC) code, and the quantity prescribed and purchased as the number of defined daily doses.31 We extracted information on all purchases of antidepressants, anxiolytics, sedatives and hypnotics (ATC codes N06A, N05B and N05C, respectively; see online supplementary appendix 1) in our analytic sample, following phase 2 survey date (index date) during the follow-up until 31 December 2013. Dates of deaths were retrieved from Statistics Finland (the Causes of Death Register).
Covariates
All covariates were survey based and from phase 1. We measured age, sex and marital status (married/cohabiting vs other). Moreover, we measured current smoking (yes vs no), binge drinking (six or more units of alcohol on one occasion once a month or more often), low physical activity (<14 metabolic equivalent hours per week) and body mass index, which was categorised as non-obese (≤30 kg/m2) and obese (>30 kg/m2).
Statistical analysis
The associations between sex, age and psychotropic medication during the follow-up were first analysed using the Χ2 test. Cox proportional hazard models were fitted to examine the association between change in psychosocial and physical working conditions between phase 1 and phase 2 and subsequent psychotropic medication during the follow-up. We estimated HRs and their 95% CIs for psychotropic medication by changes in each working condition by first controlling for age and sex; then further controlling for marital status, smoking, binge drinking, low physical activity and obesity. In the first analysis, for each working condition, the reference group was the most favourable working condition (ie, repeated high control, repeated low demands and repeated high physical work load, respectively). To examine the effects of positive changes in working conditions, we conducted an additional analysis using the least favourable working condition as the reference group. The follow-up began from the date of the phase 2 survey response and ended at the first record of the psychotropic medication purchase, death, or on 31 December 2013, whichever came first.
We conducted the Therneau-Grambsch non-proportional hazards test, complementing it with the smoothed scatter plot of Schoenfeld residuals against explanatory variables. The visual inspection of the scatter plots supports the interpretation that the proportional hazards assumption was met. The scatter plots for any psychotropic medication are presented in online supplementary appendix 2. Moreover, the interaction terms between each working condition and logarithm of the follow-up period for any psychotropic medication as well as for each medication group were non-significant (all p>0.05), further confirming that the proportional hazards assumption was justified.
None of the gender interactions were statistically significant (all interaction terms sex*working condition p>0.05); we therefore analysed women and men together, adjusting for gender.
The analyses were conducted with SAS V.9.4 and R.
Results
Table 1 shows the distribution of the key study variables by any prescribed psychotropic medication during the follow-up. The mean age at baseline was 47.5 years. A total of 1008 participants (28%) recorded at least one purchase of prescribed psychotropic medication during the mean follow-up of 5.0 years. Psychotropic medication was more prevalent among women (29%) than among men (23%). Nineteen per cent of the participants received antidepressant medication during the follow-up. The corresponding figures for anxiolytics and for hypnotics/sedatives were 7% and 17%, respectively.
Distribution of demographics (phase 1; 2000–2002), working conditions (phase 1–phase 2; 2007) and any psychotropic medication* between phase 2 and 2013, the Helsinki Health Study, Finland (%) (n=3587)
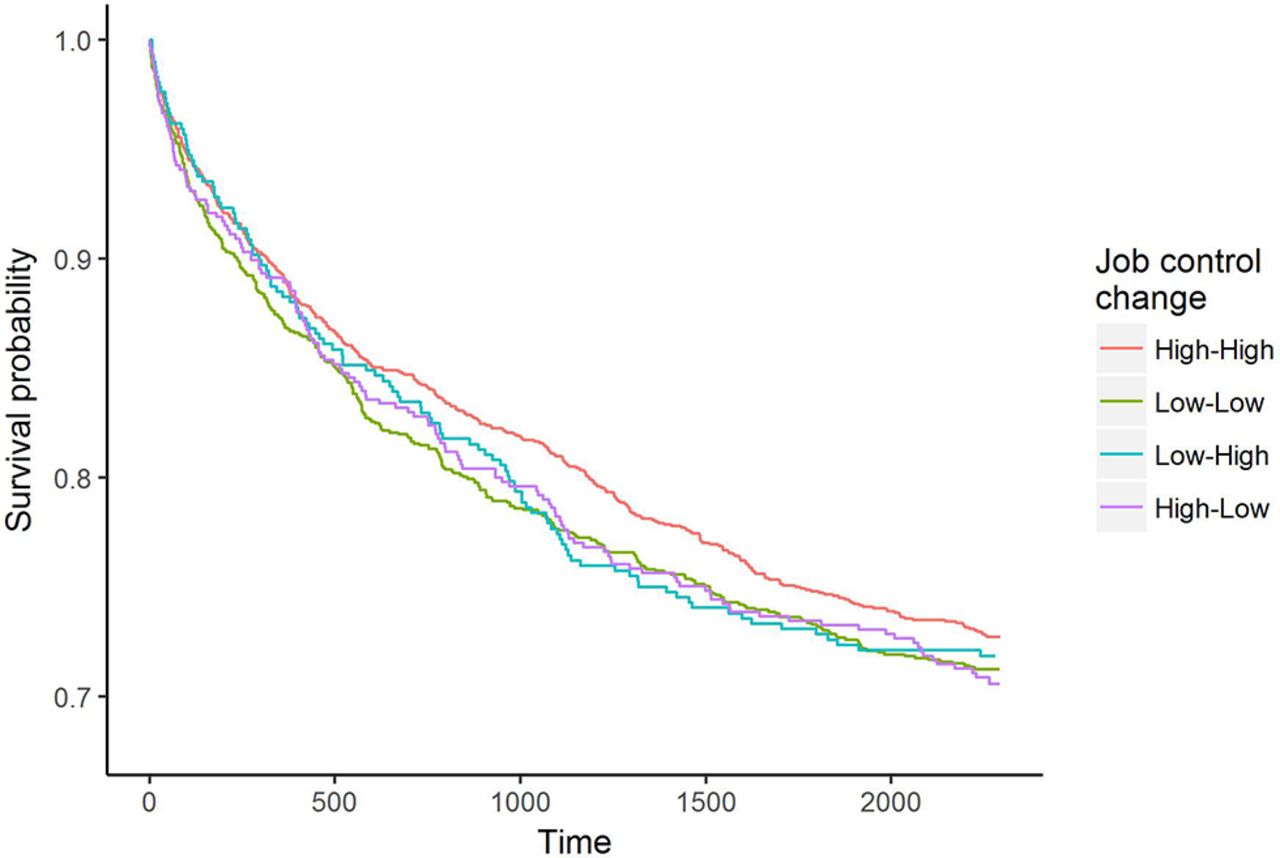
As displayed in table 2, after adjustment for age and sex, repeated high job demands (HR=1.22, 95% CI: 1.04 to 1.42) were associated with any psychotropic medication. The association between repeated high physical work load and any psychotropic medication was marginally statistically significant (HR=1.17, 95% CI: 0.98 to 1.39). Figures 1–3 show survival curves for any psychotropic medication by changes in working conditions.

Survival curves for any psychotropic medication by changes in job control.

Survival curves for any psychotropic medication by changes in job demands.

{kind=link}
{kind=link}
{kind=link}
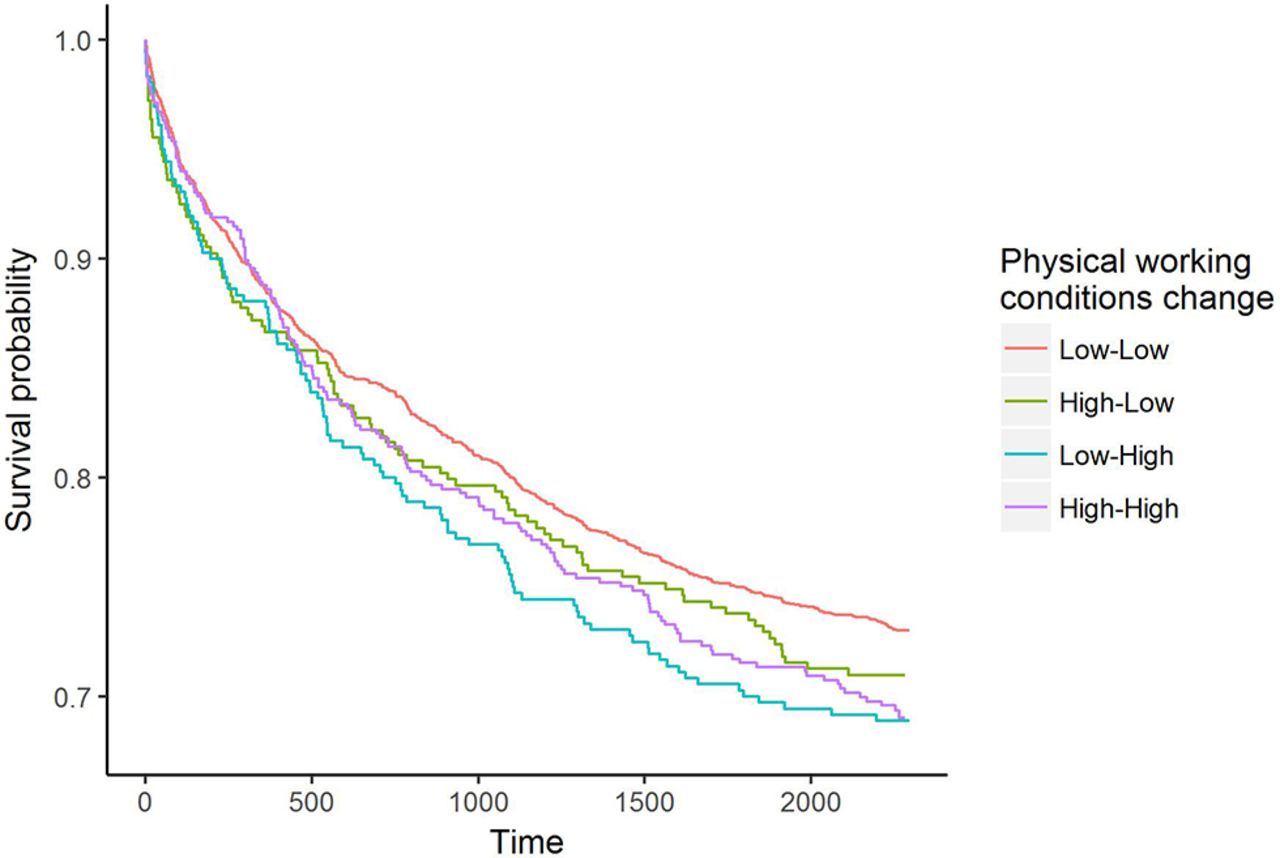
Survival curves for any psychotropic medication by changes in physical working conditions.
Age and sex-adjusted HRs and their 95%CIs for associations of changes in working conditions between phase 1 (2000–2002) and phase 2 (2007) and subsequent psychotropic medication between phase 2 and the end of 2013, the Helsinki Health Study, Finland
When the groups of psychotropic medication were examined separately, repeated high job demands (HR=1.20, 95% CI: 1.00 to 1.45) and repeated high physical work load (HR=1.30, 95% CI: 1.06 to 1.59) were associated with subsequent antidepressant medication, whereas repeated low job control (1.37, 95% CI: 1.05 to 1.79), repeated high demands (HR=1.33, 95% CI: 1.00 to 1.76) and repeated high physical work load (HR=1.66, 95% CI: 1.24 to 2.23) were associated with subsequent anxiolytic medication. Increased job control and increased physical work load were associated with subsequent sedative and hypnotic medication. Repeated high demands and repeated high physical work load showed associations with subsequent sedative and hypnotic medication. Further adjustment for marital status, health behaviours and obesity only marginally changed the HRs (data not shown).
We additionally tested whether favourable change in working conditions was associated with a lower risk of psychotropic medication, by using the least favourable working conditions as reference categories (table 3). Compared with repeatedly low job control, increased job control was associated with a lower risk of anxiolytic, but a higher risk of sedative and hypnotic medication. Compared with repeatedly high physical work load, decreased physical load was associated with a lower risk of subsequent antidepressant and anxiolytic medication.
Age and sex-adjusted HRs and their 95% CIs for associations of changes in working conditions between phase 1 (2000–2002) and phase 2 (2007) and subsequent psychotropic medication between phase 2 and the end of 2013, the Helsinki Health Study, Finland
Discussion
In this study, repeated and increased exposure to adverse psychosocial and physical working conditions was associated with subsequent psychotropic medication. It is notable that we found similar associations for both types of working conditions. However, the associations between adverse working conditions and subsequent psychotropic medication were modest. This is expected asthe aetiology of mental disorders—the main indication for psychotropic medication—is complex and multifactorial, involving multiple social, psychological and biological factors.32 Exposure to adverse working conditions or a positive or negative change in them is only one such factor.
Compared with employees with repeated low job demands, the employees whose job demands had increased had a higher risk of purchasing any psychotropic medication as well as antidepressant medication. Moreover, repeated exposure to high job demands was associated with subsequent antidepressant and anxiolytic medication, with anxiolytics showing a slightly stronger association. Antidepressant and anxiolytic medications are likely to reflect depression and other mental disorders such as anxiety disorders (including generalised anxiety disorder and panic disorder). A number of previous studies have shown a link between high job demands and an increased risk of mental ill-health.3 15 16 33
Previous results for job control have been mixed. In a meta-analytic review published in 2006, low decision latitude predicted common mental disorders.3 In terms of more objective outcomes, null results have been reported for psychotropic prescriptions,13 34 whereas one previous study showed an association between high decision authority and an elevated risk of hospital admissions due to mental disorders.35 In our study, increased job control was associated with a subsequent sedative and hypnotic medication. In a previous study, active jobs, that is, those with high levels of control and demands, were associated with a higher risk of depression and burn-out.36 It is possible that increased decision authority and high responsibility may become a burden for some employees. It is also possible that high job control reflects not only working conditions but also characteristics of a generally more active employee with a higher likelihood of seeking treatment.35
The result that increased job control was associated with a lower risk of anxiolytic, but a higher risk of sedative and hypnotic medication seems conflicting and is difficult to explain. It is possible that a switch between some anxiolytic benzodiazepine and hypnotic benzodiazepine could confound these associations. Unfortunately we had no information about the indication of the medication use.
When comparing with the least favourable working conditions, increased job control was associated with a lower risk of anxiolytic medication and decreased physical load was associated with a lower risk of antidepressant and anxiolytic medication. Two earlier studies did not find an association between favourable changes in psychosocial working conditions and a decreased risk of subsequent mental ill-health.15 37 However, in one previous study, both improvements and deterioration in job demands and control were associated with corresponding improvements or deterioration in mental health,18 and in another study, decrease of job strain was associated with a lower likelihood of repeated insomnia symptoms.38
Most of the earlier studies have investigated only psychosocial working conditions. In the present study, repeatedly high and increased physical work load were associated with subsequent psychotropic medication. In fact, the strongest association (HR=1.66 for anxiolytic medication) between working conditions and psychotropic medication was found for repeated high physical workload. Our findings thus support the earlier findings in the present and other cohorts, which have shown associations between exposure to adverse physical working conditions and common mental disorders,16 disability retirement due to mental disorders,20 purchases of sleeping pills19 and perceived mental strain.21
Methodological considerations
Certain limitations need to be acknowledged. First, because of the relatively long interval between the two working conditions measurements, this study could have underestimated the effect of changing working conditions on subsequent medication. Moreover, working conditions could have changed several times during the follow-up; this could have resulted in more conservative effect sizes.
Second, we were unable to assess the magnitude of change in working conditions; the use of these crude measures only assessed whether a participant had moved from one category to another. Furthermore, we did not have information about the prior duration of exposure to adverse working conditions. The use of thresholds may have led to underestimates of true effects of changing working conditions.5
Third, we did not have information about clinical indication the examined medication was prescribed for. Even if psychotropic medication is a recommended treatment for a number of mental disorders and prescription data derived from official registers can therefore be considered as a proxy for mental disorders requiring treatment, these medications are prescribed also for other conditions. On the other hand, it has been shown that mental disorders are underdiagnosed and undertreated.39
Fourth, we did not have information about the discontinuation and the pattern of use of psychotropic medication. Even if a participant had purchased the prescribed medication from the pharmacy, they could have discontinued the use. Discontinuation of psychotropic drugs can lead to different meanings: the discontinuation of antidepressants can be associated with either side effects or lack of follow-up controls, whereas sporadic use of anxiolytics and hypnotics can be due to temporary discomfort. Unfortunately we had no information about the pattern of use of the prescribed medication, that is, whether the medication was used sporadically or continuously.
Fifth, participants who left employment between phase 1 and phase 2 were not included in the study. It has been suggested that the age-related health selection may result in a more resilient older worker population.37 A healthy worker effect may thus have led to underestimation of the associations.
Finally, even if the data consisted of a broad range of both manual and non-manual occupations, the study population was not a representative sample of the total working population. Because the Finnish public sector workforce is female dominated, women were over-represented also in this sample. Moreover, the present sample consisted only of ageing employees with stable and secure long-term employment and working in the capital city. Therefore, the results may be generalisable, with caution, to the Finnish municipal sector, but might not be generalisable to other age groups, cohorts and industries.
Despite these limitations, the present study has a number of strengths. The main strengths are the use of prospective design which enabled us to examine changes in working conditions, data derived from a well-characterised occupational cohort, minor attrition, deterministic linkage to administrative medication records and an ability to examine changes in both psychosocial and physical working conditions. Psychotropic medication data were based on a physician’s prescription and covered virtually all reimbursed psychotropic prescriptions for the analytic sample. The use of register-based medication data allowed us to remove the prevalent cases and helped avoid the problems related to use of self-report measures such as recall and common method bias. Extensive non-response analyses were available and showed only small non-participation bias. We were able to adjust for a number of important covariates such as health behaviours and obesity.
Conclusion
To conclude, this study showed that established psychosocial risk factors such as repeated exposure to high job demands and low control are associated with subsequent psychotropic medication in midlife and older employees. Furthermore, the results also showed that repeated and increased exposure to adverse physical working conditions may contribute to subsequent psychotropic medication. Identification of these potentially modifiable risk factors implies possibilities for prevention.40 Theory-based, organisationally focused interventions to tackle adverse working conditions might be beneficial. Evidence for this is emerging. An intervention study in Canadian hospitals showed an intervention to reduce work stress was able to produce beneficial long-term effects on hospital employees’ emotional well-being, in particular through reducing professional burn-out.41 However, well-designed randomised controlled trials with reliable and valid objective indicators of working conditions are needed to reliably test whether intentional workplace interventions can prevent employee mental ill-health.
References
Footnotes
Twitter @AKouvonen @helsinkiuni
Contributors AK directed the implementation of the study, led all aspects of the work, and drafted the article. AK and OP performed the data analysis. TL, EL, OP and OR contributed to acquisition of data. MM, TL, OP, EL and OR contributed to designing the study’s analytic strategy, interpreting findings, reviewing the article and revising it critically for important intellectual content. All authors jointly designed and conceptualised the study and approved the manuscript’s submission for publication.
Funding This work was supported by the Finnish Work Environment Fund (grant 112231), the Academy of Finland (grants 1129225, 1257362 and 1294514) and the University of Helsinki. AK was supported by the Economic and Social Research Council (ESRC) (grant ES/L007509/1). MM was supported by the Finnish Work Environment Fund (grant 115182) and the Juho Vainio Foundation. TL was supported by the Academy of Finland (grant 287488).
Competing interests None declared.
Ethics approval The Ethics Committees of the Department of Public Health, University of Helsinki, and the health authorities of the City of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.