Article Text

Abstract
Objective The occupational risk for Legionella infection among dental healthcare workers (DHCWs) is conjectured because of the risk of routine inhalation of potentially contaminated aerosols produced by the dental instruments. Nevertheless, occupational epidemiology studies are contrasting. This meta-analysis assessed the level of scientific evidence regarding the relative occupational risk for Legionella infection among DHCWs.
Methods Literature search was performed without time and language restrictions, using broad data banks (PubMed, Scopus, Web of Science, GOOGLE Scholar) and generic keywords (‘legionella’ AND ‘dent*’). Analytical cross-sectional studies comparing prevalence of high serum Legionella antibody levels in DHCWs and occupationally unexposed individuals were considered. The relative occupational risk was assessed through prevalence ratio (PR) with 95% CI. Between-study heterogeneity was assessed (Cochran’s Q test) and was used to choose the meta-analytic method. Study quality (modified Newcastle-Ottawa Scale) and publication bias (Begg and Mazumdar’s test, Egger and colleagues’ test, trim and fill R0 method) were assessed formally and considered for the sensitivity analysis. Sensitivity analysis to study inclusion, subgroup analyses (dental staff categories; publication year, before vs after 1998, ie, 5 years after the release by the Centers for Disease Control and Prevention of the infection control guidelines in dental healthcare setting) were performed.
Results Seven studies were included (2232 DHCWs, 1172 occupationally unexposed individuals). No evidence of publication bias was detected. The pooled PR estimate was statistically non-significant at 95% level (1.7; 95% CI 0.8 to 3.2), study-quality adjustment did not change the PR considerably (PR, 1.5; 95% CI 0.5 to 4.1). PR was statistically significant before 1998 and no longer significant after 1998. Subgroup analysis according to DHCW categories was inconclusive.
Conclusions There is no scientific evidence that DHCWs are at high occupational risk. The differences between former and recent studies could be due to different characteristics of municipal water systems and the infection control guideline dissemination.
- Legionella
- dentist
- occupational and industrial medicine
- dental healthcare setting
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The evidence-based occupational risk for Legionella infection among healthcare workers has never been assessed. Yet, some healthcare working categories, such as hospital staff and dental healthcare workers, are routinely exposed to the risk of Legionella inhalation. This is the first study in this important field.
The strategy to use broad databases and to include any kind of publication written in any language and without time restrictions allowed to locate a comprehensive number of primary studies.
The explanation provided for the current limited evidence of occupational risk to dental healthcare workers, that is, the widespread acknowledgement of the infection control guidelines in dental healthcare settings released by the US Centers for Disease Control and Prevention, is only a conjecture due to missing information.
Using these data and those reported by the studies on hospital staff, it was possible to speculate that the occupational risk for Legionella infection to healthcare workers was low and that infection was more likely associated to local climatic and geographic characteristics.
Introduction
The risk for Legionella infection in dental healthcare settings was conjectured in 1981, only 5 years after the first Legionnaires’ Disease (LD) outbreak reported in 1976 in Philadelphia. Indeed, according to one of the first LD case series, 10% sporadic cases had a history of dental infections and probably sought for dental healthcare.1 In 1986, the first survey on dental offices was performed in Austria and reported that Legionella pneumophila serogroup 1 was detectable in waterlines of 10% dental units.2 In 1985, a study performed in a US dental school reported that prevalence of high serum Legionella antibody level in dental healthcare workers with at least 2 years of clinical experience was higher than in occupationally unexposed subjects (23% vs 16%), thus suggesting that the dental staff could be at occupational risk for Legionella infection.3 In 1995, the case of a dentist who died from LD was reported and legionellae were detected in the dental unit water system of his office.4 These and other studies on dental unit water system contamination with legionellae and on Legionella antibody seroprevalence in the dental staff collectively suggested that dental healthcare workers could be at occupational risk, but scientific evidence was inconclusive.5
Data regarding other healthcare settings also are inconclusive. In France, for example, Pontiac fever-like incidence in the nursing home personnel was not associated to Legionella detection in the shower water.6 A Danish study, which found that Legionella seroprevalence was higher in hospital healthcare workers than in blood donors (45% vs 23%), failed to associate high Legionella antibody levels with direct exposure to contaminated hospital shower water.7 According to an Italian study, there were minimal differences in seroprevalence between ward and office staff in a Milan hospital (35% vs 27%) and between hospital ward staff and blood donors in a Naples hospital (49% vs 44%).8
Several reviews, editorials and discussion papers warn that the occupational risk of Legionella infection to the dental staff is high (Refs 9–11 are only recent examples). The arguments in support of this hypothesis are essentially four. The principal is the frequent detection of legionellae in dental unit water systems. A multicentre European study found 4% dental unit water systems contaminated with Legionella microorganisms (lowest detection limit, 1 colony-forming unit (CFU) per mL),12 but according to local studies such a proportion could be higher, namely, 15% in Italy (lowest detection limit, 1 CFU per L),9 28% in Germany (lowest detection limit, 1 CFU per 10 mL)13 and 33% in South Africa (lowest detection limit, 1 CFU per mL).14 The second argument is that dental instruments, such as air–water syringe, dental turbine and ultrasonic scaler handpieces, produce aerosols. Thus, if dental unit water is contaminated with legionellae, these microorganisms could be spread in the environment during dental therapy and inhaled by patients and staff. The third is that four sporadic cases of LD transmission in dental healthcare settings are reported.4 15–17 The fourth is that some occupational epidemiology studies reported that the dental healthcare workers yielded higher Legionella antibody seroprevalence than unexposed controls.3 8 18 These arguments suggest that dental unit water systems contaminated with legionellae may expose the dental staff to Legionella infection and even LD.
These arguments are not entirely agreeable. Indeed, the conjectured spread of Legionella microorganisms in the environment is in contrast with the low Legionella contamination level of air, since only one study reported one positive air sample (<5% of all samples),19 while the remaining studies did not.9 20–22 As for the sporadic cases of LD, the recent discovery that human-to-human LD transmission is possible,23 along with the considerations that L. pneumophila may colonise the oropharynx24–26 for up to 2 months27 and that oropharyngeal flora is detected into dental unit water systems after dental therapy,28 29 suggests that the dental unit water systems can be contaminated by colonised or infected patients during dental therapy. Therefore, the chicken–egg dilemma (ie, strain-typing matches of isolates from the environment and the patient do not demonstrate where the organism occurred first) regarding environmental pathogens also applies to these reports.30 31 As for the last argument, some reports showed that dental healthcare workers did not yield higher Legionella antibody seroprevalence than controls.32 33
Assessing the occupational risk of Legionella infection to dental staff is not a marginal question, since the number of individuals who could be occupationally exposed is high. Indeed, the numbers of practising dentists in Europe and the USA are 330 00034 and 200 000,35 respectively. In addition, there is an equal number of other working categories, such as dental assistants and hygienists. Thus, the problem of occupational risk of Legionella infection may interest 1–2 million healthcare workers globally.
Therefore, this meta-analysis was finalised at investigating the relative occupational risk of Legionella infection to dental healthcare workers.
Methods
Search strategy
Legionella colonisation of artificial water systems is strongly associated to climatic and geographic factors.36 37 Therefore, Legionella antibody seroprevalence in the general population is not steady, and high absolute seroprevalence in dental healthcare workers could be not indicative of an occupational risk if the general population seroprevalence is concurrently high and vice versa. For this reason, a relative estimate of the occupational risk of Legionella infection was preferred to absolute estimates, such as incidence or prevalence rates.
Literature search was undertaken trying to locate the highest possible number of primary studies that reported or allowed to estimate the relative occupational risk, trying to minimise publication and selection biases. There were no restrictions in publication year and language, while broad data banks that could help locate congress proceedings and doctoral theses also were considered. The data banks used were PubMed, Scopus, Web of Science and GOOGLE Scholar. Relatively generic keywords were chosen, namely, ‘legionella’ AND ‘dent*’ in all fields (PubMed), title/abstract/keywords (Scopus), topic (Web of Science) and anywhere in the paper (GOOGLE Scholar). As for GOOGLE Scholar, papers were sorted in order of relevance and the 500 most relevant titles were considered (further details in online supplementary appendix 1). GOOGLE Translate was used to handle articles published in languages other than English.
Supplementary file 1
Literature search was performed by one author (SP), expert in meta-analysis of observational studies, who also screened titles and abstracts of the identified studies. Full texts of the studies that could fall into the inclusion criteria were searched, and eligibility was assessed by the two authors together. Totally and partially overlapping studies and studies that did not fall into the inclusion criteria were excluded. Corresponding authors of studies who could be eligible, but reported incomplete information, were contacted to seek for missing data. Reference lists from full texts also were checked to detect potentially missing eligible studies.
Inclusion and exclusion criteria
Legionellae are almost ubiquitous where there are artificial water systems, such as offices, apartments, gyms, schools and even churches, but are more frequent in specific settings, such as hospitals and nursing homes, hotels, cruise ships and thermal springs.38–40 Subject selection in occupational epidemiology is based on occupational exposure status.41 Therefore, excluding the category of dental healthcare workers, under investigation, occupationally exposed individuals were those working in hospitals, nursing homes, hotels, cruise ships and thermal springs,42 whereas occupationally unexposed individuals were subjects working or living in settings where artificial water systems are not frequently contaminated. Also, occupationally unexposed individuals were subjects who could occasionally, or for reasons different from their jobs, attend settings where contamination is frequent.
With these assumptions regarding occupational and non-occupational exposure, inclusion and exclusion criteria were the following:
1. Study design. All studies in occupational epidemiology that assessed or provided enough data to estimate the risk ratio between dental healthcare workers and occupationally unexposed individuals were considered. Therefore, cohort, case–control and analytical cross-sectional studies were eligible, while case reports and series, editorials, reviews, discussion papers and meta-analyses were excluded.
2. Dental healthcare workers. Given the relatively high frequency of dental unit water systems contaminated with legionellae,9 12 13 it was arbitrarily assumed that any dental healthcare worker with enough clinical experience was in some way exposed to legionellae coming from the dental unit water systems during daily practice. Therefore, occupationally exposed individuals were dental healthcare workers with any level of clinical experience, such as general dental practitioners, specialists, dental hygienists, assistants and dental students with clinical experience. Excluded were dental healthcare working categories without clinical experience, such as dental students from first years and administrative staff.
3. Occupationally unexposed individuals. These subjects could be selected from any setting but must not be exclusively selected from the abovementioned occupationally exposed categories, namely, healthcare workers practising in hospitals and nursing homes,7 43 water service providers, water system maintenance workers and subjects working in hotels, thermal springs and cruise ships.42
4. Legionella infection. Individuals with high serum level of Legionella antibodies (IgG) assessed with any laboratory method were classified as seropositive. The study was excluded if information regarding Legionella infection was assessed anamnestically.
Study quality
The quality of occupational epidemiology studies is necessarily lower than in other epidemiology studies for the aforementioned drawbacks in assessing exposure level and duration.41 In addition, assessing quality and susceptibility to bias of observational studies is not easy, as there are almost 100 quality assessment tools, none of them rigorously developed, evidence based, valid, reliable and easy to use at the same time.44 For these reasons, study quality was assessed but was considered only for sensitivity analysis, instead of incorporating study-quality weights into the analysis or using quality scores as inclusion/exclusion criteria.
The tool used in the present study was the Newcastle-Ottawa Scale (NOS), specifically designed for cohort and case–control studies45 and adapted for analytical cross-sectional studies with eight items instead of nine.46 Although NOS has been criticised for several reasons,47 it was preferred to the remaining tools because it is simple and easy to use. Following previously adopted methodology, low-quality studies (NOS scores, 0–2) were given a score of 0.25, medium-quality studies (NOS scores, 3–5) were given a score of 0.5 and high-quality studies (NOS scores, 6–8/9) were given a a score of 1.0.48 Quality assessment was performed by the two authors together. Since NOS was not validated in the field of occupational epidemiology, the study quality scores were expected to be low.
Data extraction and risk ratio assessment
It is anticipated that there were no cohort and case–control studies among the selected primary studies, but only analytical cross-sectional studies. For this reason, prevalence ratio was chosen as relative risk estimate.
For every primary study, prevalence ratio adjusted for confounders, when available, was extracted. When this measure was unavailable, the crude prevalence ratio was extracted or was calculated using the prevalence rates of subjects with high serum Legionella antibody levels in dental healthcare workers and in occupationally unexposed individuals.
Data were extracted or calculated by the two authors independently, they were compared and the differences were reconciled through discussions.
Meta-analytic methodology
Publication bias was investigated, and it was assumed that its effect in occupational epidemiology could be even more pervasive than in general epidemiology, since the publication of studies reporting lack of association between exposure and occupation is unlikely. The funnel plot with the ln(prevalence ratio) in the x-axis and precision, that is, 1/[SE ln(prevalence ratio)], in the y-axis was initially drawn. An asymmetrical plot was suggestive of high degree of publication bias. Formal publication bias investigation was performed with the test of Begg and Mazumdar49 and the test of Egger and colleagues.50 In addition, the trim-and-fill method, based on the assumption that there is an additional k0 number of relevant studies that were not located or published, was applied. The R0 method was employed to identify the k0 studies. If missing studies were detected, they were added to the primary-study set and the funnel plot was redrawn and compared with the plot drawn without missing studies to check whether symmetry improved.51 52
The pooled prevalence ratio was assessed. The meta-analytic method was chosen on the basis of the level of between-study heterogeneity, which was estimated with the Cochran’s Q, a χ2 test with (k-1) df, where k is the number of primary studies. For Q≤(k-1), the level of heterogeneity was low enough and the fixed-effects method was preferred, with the inverse of the variance of ln(prevalence ratio) as study weight. For Q>(k-1), the level of heterogeneity was high, and the more conservative random-effects method, which provided wider 95% CI, was used.53
Sensitivity analysis to study inclusion was performed to investigate whether a single study influenced the pooled prevalence ratio estimate excessively. The contribution of each study to the overall weight was assessed as a per cent of the total weight. Each study was then excluded in turn, and the pooled prevalence ratio was re-estimated and compared with the overall pooled prevalence ratio. If 95% CI of the two pooled prevalence ratio estimates did not overlap, the results of the meta-analysis were regarded as not robust enough.53
Subgroup analysis was performed to explore the reasons of between-study heterogeneity, a frequent problem in meta-analysis of occupational epidemiology.54
Subgroup analysis according to working categories: this analysis was performed to test whether there were differences between categories in the degree of occupational risk. More specifically, dentists could be at higher occupational risk than the other categories because they work closer to the dental instruments than the dental assistants and have spent more years in practising than dental students. Therefore, data regarding working categories were extracted, when possible, and the pooled prevalence ratios were estimated and compared between categories.
Subgroup analysis according to publication year: this analysis was performed to test whether the dissemination and general acknowledgement of the infection control guidelines in dental healthcare settings, released for the first time in 1993 by the Centers for Disease Control and Prevention (CDC)55 had any effect on the occupational exposure to Legionella infection. Studies were, therefore, subgrouped according to the year of publication, into former and recent studies. The threshold year of publication chosen was 1998, that is, 5 years after the release of the infection control guidelines, a period arbitrarily considered long enough to permit guideline acknowledgement at global level. The pooled prevalence ratios of former and recent studies were assessed and compared. In addition, weighted metaregression was performed, using the inverse of the variance as weight, with the logarithm of prevalence ratio in the x-axis and a dummy variable, namely, before 1998 (y=1) and after 1998 (y=2) in the y-axis. From the regression coefficient, the pooled prevalence ratios for former and recent studies were estimated and compared.
StatView 5.0.1 (SAS Institute, North Carolina, USA) and MedCalc 14.8.1 (MedCalc Software BVBA, Ostend, Belgium) were used for the statistical analyses. The significance level of statistical tests was α=0.05. This paper followed the flow of information proposed by the PRISMA statement for the study search,56 the MOOSE guidelines for reporting meta-analyses of observational studies57 and the recommendations provided by the review of practice of meta-analysis in occupational epidemiology.54
Results
The last literature search was performed on 2 March 2017. Screening provided 32 papers (figure 1); 18 of them were excluded after full text reading because they were not relevant. Of the remaining 14 studies, 7 were excluded. Two of them provided data overlapping with other studies already included in the analysis,58 59 one focused on respiratory illness,60 two did not include an occupationally unexposed group61 62 and two did not discriminate between different occupationally exposed categories.63 64 The corresponding authors of the latter studies were contacted to obtain specific data regarding dental healthcare workers. The corresponding author of the first study replied that they were unavailable, the corresponding author of the second study did not reply. At the end of the study selection procedure, seven primary studies remained. Three were published between 1985 and 19883 18 65 and one in 1992,66 while the remaining three were published between 2003 and 2008.8 32 33 The study of Borella and colleagues8 was split into two because it was a multicentre study. These studies collectively included 2232 dental healthcare workers and 1172 occupationally unexposed individuals.

Flowchart of article selection process (last updated 2 March 2017) according to PRISMA.
The dental healthcare workers were mostly dentists, clinical-level students and assistants. Occupationally unexposed individuals were extracted from the general population or were white-collar workers, blood donors and volunteers (table 1). Last-year medical students and young doctors were used by Oppenheim and colleagues as occupationally unexposed individuals and were not considered occupationally exposed by the authors.65 Therefore, this study was not excluded.
Characteristics of the primary studies and prevalence ratios of high serum Legionella antibody (IgG) level assessed using extracted data
As anticipated, the generally low primary-study quality scores were not surprising (online supplementary appendix 2). Nevertheless, all studies made clear distinctions between dental healthcare workers and occupationally unexposed individuals and adopted reliable diagnoses of Legionella infection based on serologic tests, namely, ELISA,3 33 rapid microagglutination test65 and indirect immunofluorescence test.8 18 32 66 One study, however, showed higher quality because it was performed on a representative sample of dentists and reported the response rate.32 The point prevalence ratios in the eight settings ranged between 0.2 and 7.1 (table 1), with generally higher values in former studies.
Supplementary file 2
The funnel plot (online supplementary appendix 3) was apparently not symmetrical. Nevertheless, the Kendall’s τ of the test of Begg and Mazumdar resulted −0.43 (p=0.13), the intercept of the test of Egger and colleagues resulted 1.12 (p=0.52) and the trim-and-fill method failed to identify potentially missing studies (R0=0). However, the presence of publication bias could not be excluded because there were few primary studies and in these circumstances the power of formal tests is too low to distinguish between chance and real symmetry.67
Supplementary file 3
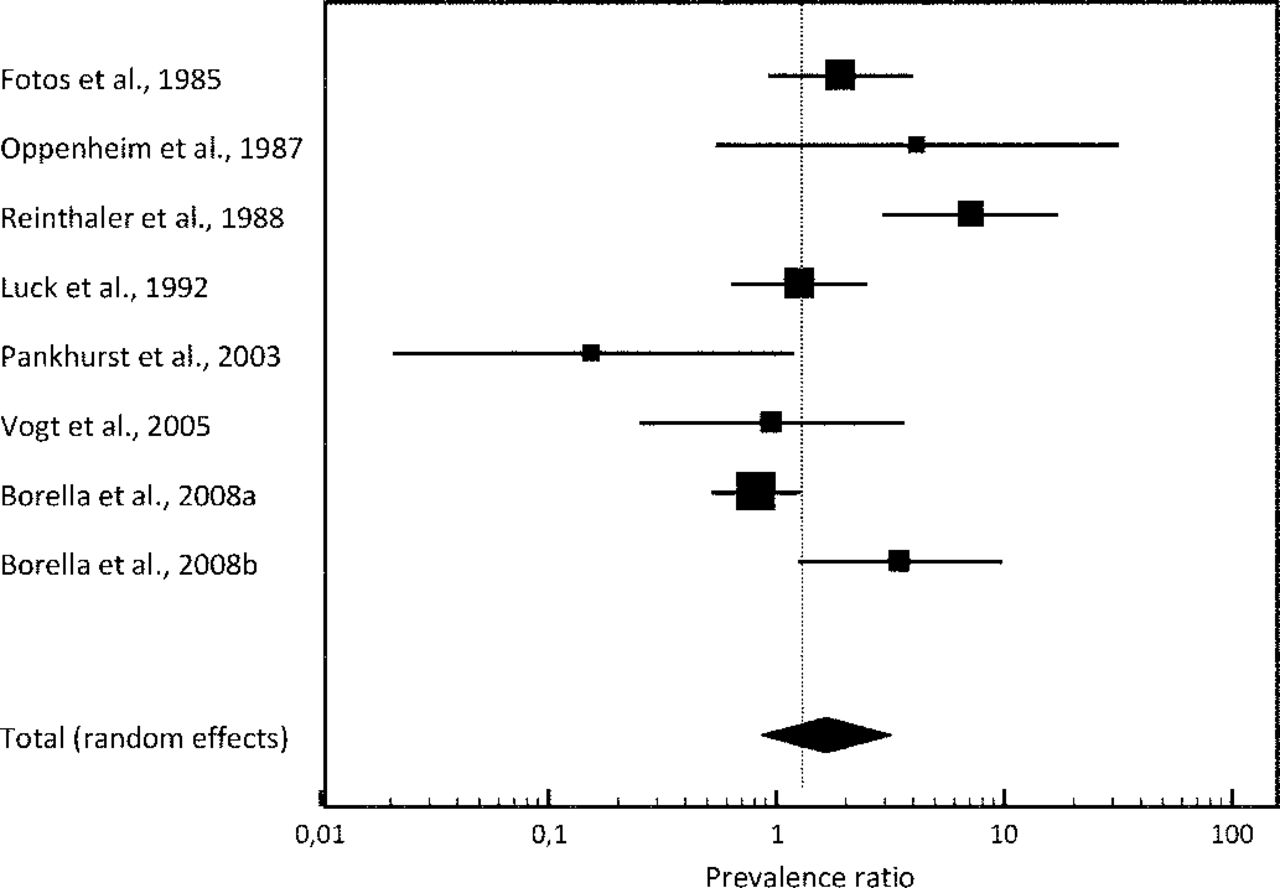
The forest plot (figure 2) shows that the prevalence ratio estimates were largely different in both precision (ie, width of 95% CI) and direction (ie, to the left or to the right with respect to the neutral value of 1), thus suggesting that the between-study heterogeneity was high. This idea was confirmed by the high Cochran’s Q (table 2), and therefore, the random-effects method was used to estimate the pooled prevalence ratio. The pooled prevalence ratio including all the studies was 1.7, with 95% CI 0.8 to 3.2, statistically non-significant at 95% level. Adjustment for study quality caused a drop in between-study heterogeneity (Cochran’s Q-test χ2 7df passed from 28.72 to 16.13) and an increase in CI width but did not change the pooled risk estimate considerably (pooled prevalence ratio, 1.5; 95% CI 0.5 to 4.1).
Pooled prevalence ratio of high serum Legionella antibody level in dental healthcare workers

{kind=link}
{kind=link}
Forest plot of the prevalence ratios estimated using the data extracted from the primary studies and pooled prevalence ratio estimated with the random-effects method.
Sensitivity analysis to study inclusion (online supplementary appendix 4) showed that the weight of three studies3 8 66 accounted for almost three-fourths of the overall weight. However, the exclusion of these studies in turn did not produce a significant change in the pooled prevalence ratio estimate.
Supplementary file 4
As for subgroup analysis stratified for working categories (table 2), the pooled prevalence ratio estimate regarding dentists (pooled prevalence ratio, 1.4; 95% CI 0.5 to 3.9) was based on six studies published during a 20-year interval, while analyses on dental assistants and dental students were based on only two studies. These results were, therefore, inconsistent.
The difference between former and recent studies was not significant at 95% level (table 2). This subgroup analysis, however, showed that there was a significant Legionella infection occupational risk before the year 1998 (prevalence ratio, 2.6, 95% CI 1.1 to 6.2), while after the year 1998, such a situation changed and the pooled point prevalence ratio estimate was neutral (ie, value of 1). The weighted metaregression analysis (footnotes in table 2) provided more conservative estimates, with similar point estimates as those obtained with the random-effects method, but wider CIs and the prevalence ratio of studies published before 1998 was no longer significant at 95% level.
Discussion
Meta-analyses of observational studies in occupational epidemiology yield relatively low external validity due to several forms of bias, some of them inherent to the observational studies used for the analysis and some inherent to the meta-analytic methods. More specifically, occupational epidemiology often relies on studies performed on small samples and affected by information bias regarding exposure.41 54 Thus, a meta-analysis may help overcome this problem, provided that literature search is comprehensive enough, that sensitivity analysis is performed and that results are considered as an aid rather than a measure of the occupational risk, due to the possibility to produce spurious risk estimates.68
All the primary studies used in this meta-analysis had a certain degree of information bias regarding exposure assessment to legionellae coming from the dental unit water systems. This, however, is a difficult problem to overcome even performing routine water controls, since Legionella contamination level is not stable, depending on climatic variations69 and other environmental factors.70
Another problem of this analysis is that there were few primary studies. Despite the efforts to detect all the published material, only seven studies with eight settings were located. This made it impossible to assess the presence and the degree of publication bias reliably. Indeed, the statistical tests used to investigate funnel plot asymmetry yield low power when there are less than 10 primary studies67 (online supplementary appendix 3).
Due to the aforementioned study limits, the present pooled prevalence ratio estimate must be interpreted with caution and considered as an indication, rather than a measure of the occupational risk.54 68
The main strength of this meta-analysis was its comprehensiveness. The use of broad data banks allowed to detect poster presentations and studies published in languages different from English without restrictions in publication year. It is likely, therefore, that this study was based on almost all the current available information.
The present analysis suggests that there is no scientific evidence that dental healthcare workers are at high occupational risk of Legionella infection. Such an inference is corroborated by other occupational epidemiology studies. One was performed on more than 5000 US dentists. A total of 10% showed high L. pneumophila antibody levels, a value similar to the population prevalence rate. High seroprevalence was not associated with age, years in practice and hours worked per week. High L. pneumophila antibody level was even not higher in participants who did not test and did not use any method to control dental unit water quality.62 Another study reported that Legionella species in hospital dental unit water systems and in seropositive dental healthcare workers were different, thus suggesting that these subjects likely developed Legionella infection outside the hospitals where they were practising.8 In addition, LD outbreaks in dental healthcare settings were never reported71 despite billions of treatments provided each year, thus suggesting that there is strong scientific evidence of minimal LD outbreak risk to both dental staff and patients.72 73 Even the aforementioned sporadic LD cases cannot be confirmed. Indeed, one dentist died from LD in 1995, but legionellae were detected in both the dental unit and the domestic water systems, thus making it impossible to discern which of the two systems was the source of infection and which was contaminated by the infected dentist.4 A receptionist working in a dental office located in a healthcare facility developed LD. However, legionellae were detected in several areas of the healthcare facility and were undetected in the dental section, thus suggesting that the source of LD infection was outside the dental office.17 Two patients developed LD few days after a dental visit.15 16 Since both patients were in critical conditions before the dental visit, they could be already affected by LD. Indeed, it was not possible to demonstrate where the microorganisms occurred first, that is, whether patients were infected by contaminated water systems or the water systems were contaminated by the infected patients.30 31 74
It seems that dental healthcare workers were at occupational Legionella infection risk in the 80s and 90s (table 2), and three of the four studies published in this period reported point prevalence ratios higher than 1 (table 1), while since the 2000s such an occupational risk was negligible (table 2), and three of the four study settings reported point prevalence ratios lower than 1 (table 1). Such a difference could be due to the release in 1993 of the CDC’s infection control guidelines in dental healthcare settings,55 which are periodically updated.75 The success of these and similar guidelines in terms of acceptance among dental healthcare workers was great in most, but not all, developed countries and contexts.76
The primary studies used for this analysis were not consistent and differed in both absolute and relative risk to dental healthcare workers. For example, Borella and colleagues8 in Turin found high (ie, 27%) absolute L. pneumophila antibody seroprevalence and a point prevalence ratio of 0.8, while Oppenheim and colleagues65 reported low (ie, 6%) absolute seroprevalence and a point prevalence ratio of 4.1. These discrepancies could be reconciled on the basis of some considerations. First, US dentists practising in the Mid-Atlantic states had the highest seroprevalence rate, whereas the lowest rates were found in the Pacific and East Central divisions. These differences between rates were consistent with the differences in LD incidence rates reported by the CDC’s passive surveillance.62 Second, seroprevalence in Latvia was higher in populated areas, apartment buildings, buildings with municipal hot water supply systems and areas served by non-renovated water supply systems.63 Third, different serological tests produce different false positive rates due to cross-reactivity between Legionella and other bacterial species.77 These considerations suggest that there are some factors that influence the absolute Legionella antibody seroprevalence, such as climatic factors,62 the characteristics of municipal and building water systems63 and the accuracy of the serological tests.77
Other considerations may help explain the disagreements between relative risks. Indeed, early environmental studies detected high Legionella loads in various artificial water systems78 79 and in dental unit water systems,2 4 65 as high as 10 000–1 000 000 CFU/L. This situation was probably due to the characteristics of the old municipal and building distribution water systems, which promoted stagnation into tanks. At that time, water stagnation and Legionella overgrowth were even more frequent in dental healthcare settings, due to the lack of waterborne infection prevention strategies. Therefore, the dental healthcare workers were both occupationally exposed to Legionella during their daily practice and non-occupationally exposed in apartments and in other indoor settings. Absolute and relative risks were consequently high.3 18 However, if water distribution systems did not permit stagnation, the absolute risk could be low, while the relative risk remained high,65 66 due to the lack of infection control measures. Nowadays, although Legionella remains ubiquitous, high loads are hardly detected both in indoor environments,38 40 80 due to the generally improved characteristics of the distribution systems, and in dental offices9 12–14 (with exceptions in less-controlled contexts),81 due to the success of infection control guidelines. Therefore, dental healthcare workers would be at low absolute and relative risks.32 33 However, non-renovated municipal and building water distribution systems, along with climatic factors may promote Legionella overgrowth and lead to high absolute seroprevalence with concurrent low or high relative risk, according to the implementation of infection control guidelines.8 This hypothesis would explain the observed variation in both absolute Legionella antibody seroprevalence and in occupational risk but could be confirmed or rejected only through longitudinal studies that assess Legionella level in the environment and serum Legionella antibody levels in occupationally exposed and unexposed individuals.
Data on other healthcare settings are few. Indeed, according to the Italian multicentre study Legionella antibody prevalence was non-significantly higher in hospital staff than in blood donors (prevalence ratio, 1.2; 95% CI 0.9 to 1.6, assessed merging data from the four towns), while seroprevalence was better explained by increasing age and geographic differences.8 A Danish study on hospital staff found that occupational exposure, such as showering patients, taking personal showers in hospital and surgical hand washing, did not increase the risk of seropositivity, while relevant Legionella infection predictors were age, inversely associated and the routine use of air-condition in private car.7 In 82% of the French nurses who reported Pontiac-fever-like episodes, legionellae were not detected in the hospital environments where they were practising. Pontiac fever was associated with the use of immunosuppressants and, inversely, with age and years in practice.6 A study on more than 2000 Latvian individuals found that seroprevalence rate in occupationally exposed subjects, including dentists and hospital staff, was similar to the rate in unexposed individuals. The main risk factors were living in town and in apartments located in buildings.63 Bulgarian healthcare workers had higher L. pneumophila antibody levels than occupationally unexposed individuals. However, all the subjects in the sample, both the healthcare workers and the occupationally unexposed subjects, resulted positive to the L. pneumophila antibody test, suggesting that infection was widespread.64
These data, along with the hypothesis regarding dental healthcare workers’ occupational risk, could be helpful to formulate speculations regarding the occupational risk for Legionella infection to healthcare workers in general. Indeed, such an occupational risk would be low, while infection is more likely explained by geographic and climatic differences and, perhaps, individual factors such as immunosuppressant therapy, use of air condition in private car, living in apartments located in buildings and younger age. Therefore, it seems plausible that it is the responsibility of each country, even every region within a country, to do their own assessments.
Conclusion
In conclusion, the present analysis suggests that there is limited evidence of occupational risk for Legionella infection to dental healthcare workers. It seems that such a risk could be minimised through modern water distribution systems and acknowledging infection control guidelines in dental healthcare settings.
Acknowledgments
The authors are indebted to Dr Lidia Socci for manuscript editing.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
Footnotes
Contributors This study was conceived, designed, performed and written by SP and MV.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional unpublished data are available for this study.