Article Text

Abstract
Objectives To examine associations between maternal pregnancy-specific stress and umbilical (UA PI) and middle cerebral artery pulsatility indices (MCA PI), cerebroplacental ratio, absent end diastolic flow (AEDF), birthweight, prematurity, neonatal intensive care unit admission and adverse obstetric outcomes in women with small for gestational age pregnancies. It was hypothesised that maternal pregnancy-specific stress would be associated with fetoplacental haemodynamics and neonatal outcomes.
Design This is a secondary analysis of data collected for a large-scale prospective observational study.
Setting This study was conducted in the seven major obstetric hospitals in Ireland and Northern Ireland.
Participants Participants included 331 women who participated in the Prospective Observational Trial to Optimise Paediatric Health in Intrauterine Growth Restriction. Women with singleton pregnancies between 24 and 36 weeks gestation, estimated fetal weight <10th percentile and no major structural or chromosomal abnormalities were included.
Primary and secondary outcome measures Serial Doppler ultrasound examinations of the umbilical and middle cerebral arteries between 20 and 42 weeks gestation, Pregnancy Distress Questionnaire (PDQ) scores between 23 and 40 weeks gestation and neonatal outcomes.
Results Concerns about physical symptoms and body image at 35–40 weeks were associated with lower odds of abnormal UAPI (OR 0.826, 95% CI 0.696 to 0.979, p=0.028). PDQ score (OR 1.073, 95% CI 1.012 to 1.137, p=0.017), concerns about birth and the baby (OR 1.143, 95% CI 1.037 to 1.260, p=0.007) and concerns about physical symptoms and body image (OR 1.283, 95% CI 1.070 to 1.538, p=0.007) at 29–34 weeks were associated with higher odds of abnormal MCA PI. Concerns about birth and the baby at 29–34 weeks (OR 1.202, 95% CI 1.018 to 1.421, p=0.030) were associated with higher odds of AEDF. Concerns about physical symptoms and body image at 35–40 weeks were associated with decreased odds of neonatal intensive care unit admission (OR 0.635, 95% CI 0.435 to 0.927, p=0.019).
Conclusions These findings suggest that fetoplacental haemodynamics may be a mechanistic link between maternal prenatal stress and fetal and neonatal well-being, but additional research is required.
- doppler ultrasound
- small for gestational age
- pregnancy-specific stress
- perinatal mental health
- umbilical artery
- middle cerebral artery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- doppler ultrasound
- small for gestational age
- pregnancy-specific stress
- perinatal mental health
- umbilical artery
- middle cerebral artery
Strengths and limitations of this study
This study benefits from comprehensive, repeatedly collected stress and haemodynamic data, inclusion of cerebroplacental ratio and absent end diastolic flow analyses, and clinically useful dichotomisation of normal or abnormal haemodynamic outcomes.
Moreover, this study benefits from the inclusion of neonatal outcomes, the provision of novel insights into specific stressors faced by women with complicated pregnancies and the inclusion of ethnicity and deprivation index scores as potential confounding variables.
This study is limited by inconsistent sample sizes at each time point, unavailability of stress data for the full Prospective Observational Trial to Optimise Paediatric Health in Intrauterine Growth Restriction cohort, data collection primarily occurring late in pregnancy and a lack of a comparison group of women with appropriate for gestational age pregnancies.
Moreover, this study is limited by the relatively low pregnancy-specific stress reported by the sample, which can make it difficult to detect clinically significant differences, and by the many statistical tests conducted, which increase the risk of type I error.
Introduction
Pregnancy-specific stress is characterised by concerns about fetal health, diet, physical symptoms, labour, mothering and relationship changes.1 2 Pregnancy-specific stress is a distinct clinical entity,3 and pregnancy-specific stress measures are more sensitive than general stress measures in predicting preterm birth,4 5 fetal behaviour6 and childhood development.7–11 Although evidence links pregnancy-specific stress and fetal and infant outcomes, potential mechanistic pathways such as fetoplacental haemodynamics remain relatively unexplored. A recent systematic review reported 12 studies of prenatal stress and haemodynamics in pregnancy as measured by Doppler ultrasound;12 only three measured pregnancy-specific stress.13–15 There is therefore an evidence gap regarding potential associations between pregnancy-specific stress and fetoplacental haemodynamics.
Doppler ultrasound indirectly measures fetoplacental haemodynamics16 by insonating the umbilical artery (UA) and fetal middle cerebral artery (MCA).17 Poor placentation results in increased resistance to blood flow in the UA,18 leading to a higher pulsatility index (PI), resistance index and systolic/diastolic ratio. Increased UA resistance is associated with intrauterine growth restriction (IUGR), fetal distress and adverse neurodevelopmental outcomes.19 In more extreme cases, resistance to UA blood flow rises enough that blood flow is no longer observed during fetal cardiac diastole, at which point absent end diastolic flow (AEDF) is diagnosed. Increased fetal MCA blood flow can indicate fetal cardiovascular distress, hypoxia or anaemia, and an abnormally low MCA PI can indicate fetal ‘brain-sparing’ due to severe hypoxia and acidosis.20 Fetal brain-sparing can also be indicated by an abnormal cerebroplacental ratio (CPR), the ratio of MCA PI to UA PI, which may be a more sensitive predictor of adverse perinatal outcomes than either the UA or MCA PI alone.21–24
The Prospective Observational Trial to Optimise Paediatric Health in Intrauterine Growth Restriction (PORTO) was conducted in 2010–2012 in the seven academic obstetric centres in Ireland and Northern Ireland. This study involved serial ultrasound assessments of 1116 women with small for gestational age (SGA) pregnancies25 and presents a unique opportunity to explore pregnancy-specific stress in relation to a broad range of Doppler ultrasound values.
The aim of this secondary analysis of PORTO data was to explore potential relationships among pregnancy-specific stress, fetoplacental haemodynamics and neonatal outcomes in women with SGA pregnancies. It was hypothesised that higher pregnancy-specific stress would be associated with abnormal fetal circulation (UA PI, MCA PI, CPR and AEDF), prematurity, birth weight < 2500 g, admission to a neonatal intensive care unit (NICU) and adverse perinatal outcome.
Materials and methods
PORTO study
The primary aims of PORTO were to evaluate multivessel Doppler changes in SGA fetuses (estimated fetal weight (EFW) < 10th percentile) and correlate them with paediatric morbidity. Eligibility criteria included singleton pregnancies 24+0–36+6 weeks gestation with EFW < 10th percentile for GA.26 Fetuses with major structural and/or chromosomal abnormalities were excluded. Institutional Review Board approval was obtained through each centre: the Rotunda Hospital Ethics Committee, the Belfast Health and Social Care Trust, the Coombe Women’s University Hospital Ethics Committee, Cork University Maternity Hospital Ethics Committee, University Hospital Galway Ethics Committee and the National Maternity Ethics Committee, and participants gave written informed consent. PORTO recruited 1200 consecutive ultrasound-dated singleton pregnancies; 32 (3%) were excluded due to chromosomal and/or structural abnormalities, 13 (1%) withdrew consent, 13 (1%) delivered outside of Ireland and 26 (2%) were lost to follow-up, leaving a final sample of 1116 women. A recruitment flow chart can be found in figure 1. A sample size calculation for PORTO study indicated that depending on the baseline rates of outcomes considered, the study had sufficient power (80%) with a sample size of 1100; all women who completed a Prenatal Distress Questionnaire (PDQ) at some point during their participation in PORTO were included in the analyses described here.

Prospective Observational Trial to Optimise Paediatric Health in Intrauterine Growth Restriction (PORTO) flow chart. EFW, estimated fetal weight; PDQ, Prenatal Distress Questionnaire.
Clinic visits
Referral for enrolment in PORTO occurred if there was clinical suspicion of SGA. A PORTO research sonographer confirmed EFW < 10th percentile and performed a detailed evaluation of fetal anatomy. Data collected included maternal and obstetric characteristics, delivery and birthweight outcomes, and perinatal morbidity and mortality. At enrolment, expectant mothers underwent health assessments that included blood pressure, height, weight, body mass index (BMI) and smoking and alcohol intake data collection. Parity and previous miscarriage were recorded; however, data about existing psychiatric illnesses, whether pregnancies were planned or unplanned or whether participants had a history of exposure to domestic violence were not recorded for PORTO. Obstetric management, including fetal surveillance, was standardised across all seven centres. This consisted of fetal growth assessment and more frequent evaluation with UA Doppler, biophysical profile and/or cardiotocography. Decision to deliver was at the discretion of the individual consultant obstetrician and was generally based on abnormal cardiotocography findings. Antenatal corticosteroids were administered between 24+0–36+0 weeks gestation if delivery was thought to be likely within 1 week. Outcomes of infants admitted to NICU were recorded by neonatal medical or nursing staff; outcomes for infants not admitted to NICU were recorded by research sonographers.
Ultrasound examination
Ten research sonographers performed all Doppler evaluations. Prior to study commencement, structured training was provided by maternal-fetal medicine specialists, and quality assurance assessments were conducted at regular intervals. Surveillance included evaluation of amniotic fluid volume, biophysical profile scoring and multivessel Doppler of UA, MCA, ductus venosus, aortic isthmus and myocardial performance index at every subsequent contact with research sonographers. CPRs were also calculated for each fetus.27 In the event of AEDF, testing was increased at the discretion of the consultant obstetrician. All prenatal and ultrasound data were recorded on the ultrasound software system (Viewpoint; MDI Viewpoint, Jacksonville, Florida, USA) and uploaded onto a live, web-based, consolidated database. All sonographic findings were recorded in patient case files and were available to managing clinicians. All Doppler data were interpreted using published, standardised references.28
Pregnancy-specific stress
The PDQ was introduced approximately halfway through PORTO in a staggered fashion to five of the seven participating study centres: Coombe Women and Infants’ University Hospital, the National Maternity Hospital, the Rotunda Hospital, the Royal Jubilee Maternity Hospital in Belfast, Cork University Hospital and University Hospital Galway. University Hospital Limerick and Our Lady of Lourdes Hospital in Drogheda did not participate in this aspect of PORTO data collection. Women completed the 12-item PDQ by responding to each item on a five-point Likert scale ranging from ‘not at all worried’ to ‘extremely worried’. The PDQ provides an overall score and three factor scores.29 Factor 1 measures concerns about birth and the health of the baby, factor 2 measures concerns about physical symptoms and body image and factor 3 measures concerns about emotions and relationships. PDQ scores were collected from women repeatedly across gestation, and scores were binned into three equal 5-week intervals to allow for time-specific exploration of the associations between maternal pregnancy-specific stress and fetal and neonatal outcomes.
Clinical outcome definitions
Vermont Oxford Network definitions30 were used to define adverse perinatal outcomes. Abnormal UA PI was defined as > 95th percentile,31 abnormal MCA PI as < 5th percentile32 and CPR < 1.08 was considered abnormal.33 Adverse perinatal outcome was defined as a binary composite outcome of any of the following outcomes: intraventricular haemorrhage, periventricular leukomalacia, hypoxic ischaemic encephalopathy, necrotising enterocolitis, bronchopulmonary dysplasia, sepsis or death. Prematurity was defined as delivery before 37 weeks gestation.
Deprivation index
The 2011 HP All-Island deprivation index uses three primary dimensions of disadvantage: demographic profile, social class composition and labour market situation, and provides 2011 Relative Index Scores that range from −40 (most disadvantaged) to 40 (most affluent) with a mean of 0 and an SD of 10.34
Statistical analyses
Binary logistic regression analyses were performed to evaluate associations between pregnancy-specific stress, fetoplacental haemodynamics and neonatal outcomes. For each analysis, the p < 0.05 significance threshold was used. SPSS V.22 was used for data management and statistical analyses. Because the literature suggests that maternal smoking,35–39 drinking,40 41 ethnicity,42–44 BMI,16 45 blood pressure,16 46 47 socioeconomic status48–53 and age43 45 can contribute to changes in fetoplacental haemodynamics or neonatal outcomes and parity can affect maternal psychological distress during pregnancy,54 these variables were included in the adjusted models. Although the literature also suggests that experience of previous miscarriage can affect maternal psychological distress during pregnancy,54–57 previous miscarriage and maternal pregnancy-specific stress were not associated at any time point in this sample, so miscarriage was not included in the statistical models. In order to reduce the number of variables used in the models, mean arterial pressure was calculated as 2/3(diastolic blood pressure)+1/3(systolic blood pressure). The NICU admission model was also adjusted for prematurity. PORTO participants with missing data relevant to these analyses were excluded from the original database.
Results
Participants
Of 376 recruited women who completed at least one PDQ over the course of the PORTO study, 45 (12%) were excluded: 2(0.5%) delivered outside of Ireland, 4 (1%) were recruited outside of the 24+0–36+6 GA recruitment window, 6 (2%) did not meet the EFW < 10th percentile inclusion criterion, 12 (3%) had pregnancies with congenital anomalies and 21 (6%) had incomplete data collection. This resulted in a total of 331 women completing the full study protocol; a recruitment flow chart is presented in figure 1. A total of 82 women completed at least one PDQ within the first time point bin, 205 women completed at least one PDQ within the second time point bin and 213 women completed at least one PDQ within the third time point bin; 42 women completed at least one PDQ within all three time point bins. The mean maternal age was 29.9 years, and 86.1% of mothers were of Western European origin. The mean GA at enrolment was 29.6 weeks, and the mean GA at delivery was 38.2 weeks. Maternal demographics and fetal characteristics are summarised in table 1. Women in these analyses differed from the total PORTO cohort in several ways: women in these analyses were enrolled in PORTO study earlier in their pregnancies (p=0.003), had higher systolic blood pressure (p=0.048), were more likely to be of European extraction (p=0.044), were less likely to have pre-eclampsia (p=0.035) and gave birth later (p=0.016) to babies with higher birthweights (p=0.014). Moreover, women in these analyses were less likely to have their infant admitted to the NICU (p=0.023) and had babies with significantly higher 5 min Apgar scores (p=0.001). Demographic and clinical characteristics of the current sample can be found in table 1, and comparisons between women in the overall PORTO cohort and those in these analyses can be found in online supplementary table 1.
Characteristics of participants
Pregnancy-specific stress in this sample
Participants reported surprisingly low levels of pregnancy-specific stress considering that they were informed that their pregnancies were high risk. Mean PDQ scores in this sample ranged from 11.0 (SD 6.64) at 35–40 weeks to 12.7 (SD 8.07) at 23–28 weeks (table 2). As described in table 3, women with AEDF diagnoses reported more concerns about eating healthy foods and a balanced diet for the baby (p=0.023) and having a healthy baby (p=0.013), and more fear about the possibility of premature delivery (p<0.001) than women without AEDF diagnoses. Interestingly, there were no item-level differences between women with normal or abnormal UA PI.
Pregnancy-specific stress in this sample
Differences in Pregnancy Distress Questionnaire (PDQ) items between women with normal and abnormal umbilical artery pulsatility index (UA PI) and absence or presence of absent end diastolic flow (AEDF)
Pregnancy-specific stress and fetoplacental haemodynamics
The following sections outline associations found before and after adjustment between maternal pregnancy-specific stress and abnormal UA PI, MCA PI, absent end diastolic flow and abnormal CPR.
Umbilical artery
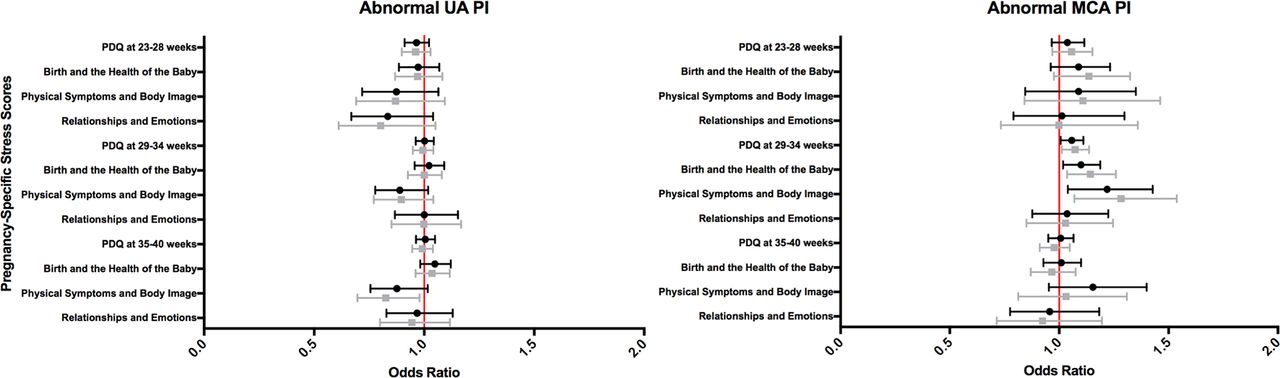
There were no significant associations between PDQ scores or factor scores and abnormal UA PI at any time point before adjustment for confounders. After adjustment, concerns about physical symptoms and body image at 35–40 weeks were significantly associated with lower odds of abnormal UA PI (OR 0.826, 95% CI 0.696 to 0.979, p=0.028).
Middle cerebral artery
Before adjustment, PDQ score (OR 1.058, 95% CI 1.007 to 1.111, p=0.026), concerns about birth and the health of the baby (OR 1.100, 95% CI 1.018 to 1.188, p=0.015) and concerns about physical symptoms and body image (OR 1.219, 95% CI 1.040 to 1.428, p=0.015) at 29–34 weeks were significantly associated with increased odds of abnormal MCA PI. After adjustment, PDQ score (OR 1.073, 95% CI 1.012 to 1.137, p=0.017), concerns about birth and the baby (OR 1.143, 95% CI 1.037 to 1.260, p=0.007) and concerns about physical symptoms and body image (OR 1.283, 95% CI 1.070 to 1.538, p=0.007) at 29–34 weeks were significantly associated with higher odds of abnormal MCA PI.
Absent end diastolic flow
Before adjustment, PDQ score (OR 1.082, 95% CI 1.005 to 1.166, p=0.037) and concerns about birth and the health of the baby (OR 1.216, 95% CI 1.074 to 1.376, p=0.002) at 29–34 weeks were significantly associated with increased odds of AEDF. After adjustment, only concerns about birth and the health of the baby at 29–34 weeks (OR 1.202, 95% CI 1.018 to 1.421, p=0.030) were significantly associated with higher odds of AEDF.
Cerebroplacental ratio
There were no significant associations between PDQ or factor scores and CPR <1.08 before or after adjustment. The results of the unadjusted and adjusted binary logistic regression models for pregnancy-specific stress in relation to abnormal fetoplacental haemodynamics are shown in online supplementary table 2. Figure 2 depicts the abnormal UA PI and MCA PI analyses.

Abnormal umbilical artery pulsatility index (UA PI) and middle cerebral artery (MCA) PI as predicted by pregnancy-specific stress. ORs >1.0 represent increased odds of the outcome occurring, while ORs <1.0 indicate decreased odds of the outcome occurring. Points represent ORs and brackets represent 95% CIs. Unadjusted models are represented in black. Adjusted models (grey) include maternal smoking, drinking, Western European origin, body mass index, mean arterial pressure, deprivation index score, parity and age at enrolment in the Prospective Observational Trial to Optimise Paediatric Health in Intrauterine Growth Restriction. PDQ, Pregnancy Distress Questionnaire.
Pregnancy-specific stress and neonatal outcomes
The following sections outline associations found before and after adjustment between maternal pregnancy-specific stress and prematurity, NICU admission, birth weight < 2500 g and composite adverse perinatal outcome.
Prematurity
Concerns about birth and the health of the baby at 29–34 weeks were significantly associated with greater odds of prematurity before adjustment (OR 1.084, 95% CI 1.008 to 1.166, p=0.031), but this association was no longer present following adjustment.
NICU admission
Before adjustment, concerns about birth and the health of the baby at 29–34 weeks (OR 1.096, 95% CI 1.023 to 1.175, p=0.009) were associated with increased odds of NICU admission, while concerns about physical symptoms and body image at 35–40 weeks (OR 0.724, 95% CI 0.541 to 0.969, p=0.030) were associated with decreased odds of NICU admission. After statistical adjustment, concerns about physical symptoms and body image at 35–40 weeks remained associated with decreased odds of NICU admission (OR 0.635, 95% CI 0.435 to 0.927, p=0.019).
Birthweight < 2500 g
Concerns about birth and the health of the baby at 29–34 weeks were associated with greater odds of birthweight < 2500 g before (OR 1.080, 95% CI 1.012 to 1.153, p=0.020) but not after adjustment.
Adverse perinatal outcome
There were no significant associations between pregnancy-specific stress and adverse perinatal outcome. The results of the unadjusted and adjusted binary logistic regression models for pregnancy-specific stress in relation to birthweight and NICU admission are provided in figure 3, and the unadjusted and adjusted analyses regarding neonatal outcomes are provided in online supplementary table 3.

{kind=link}
{kind=link}
{kind=link}
Birthweight < 2500 g and NICU admission as predicted by pregnancy-specific stress. ORs >1.0 represent increased odds of the outcome occurring, while ORs <1.0 indicate decreased odds of the outcome occurring. Points represent ORs and brackets represent 95% CIs. Unadjusted models are represented in black. Adjusted models (grey) include maternal smoking, drinking, Western European origin, body mass index, mean arterial pressure, deprivation index score, parity and age at enrolment in the Prospective Observational Trial to Optimise Paediatric Health in Intrauterine Growth Restriction. Adjusted neonatal intensive care unit (NICU) admission models also include adjustment for prematurity. PDQ, Pregnancy Distress Questionnaire.
Discussion
Pregnancy-specific stress was associated in this sample with increased odds of AEDF and abnormal MCA PI, and decreased odds of abnormal UA PI and NICU admission. However, these associations were small and varied according to the timing and nature of stress reported. Only three studies have explored associations between pregnancy-specific stress and Doppler ultrasound parameters, and this is the first exploration of associations between pregnancy-specific stress and MCA PI, CPR and AEDF in women with SGA pregnancies.
The association between concerns about physical symptoms and body image at 35–40 weeks and decreased odds of NICU admission is surprising. Women with higher concerns about physical symptoms and body image may be more conscious about nutrition and physical activity; however, this cannot be explored further as nutrition and exercise data were not collected for PORTO. It may be of interest in future studies to collect nutrition, physical activity and health-related behavioural data.
Associations between pregnancy-specific stress and both decreased odds of abnormal UA PI and increased odds of AEDF may appear contradictory. It is possible that women with healthier pregnancies, who may therefore be experiencing lower concerns about birth and the health of the baby, might instead have more concerns about physical symptoms and body image, which were associated with lower odds of abnormal UA PI. Moreover, women with AEDF were informed of their further increased medical risk, admitted as inpatients, and provided with a premature delivery plan, and therefore represent a unique population within this study. In order to determine whether there were associations between pregnancy-specific stress and subsequent AEDF, it would have been necessary to collect baseline PDQ data before diagnosis. AEDF diagnosis may also have increased pregnancy-specific stress; women with AEDF had higher mean PDQ scores and reported more concerns about eating health foods and a balanced diet for the baby, having an unhealthy baby and the prospect of premature delivery than women without AEDF (table 3). It is also possible that greater concerns about birth and the health of the baby may result in reduced concerns about other aspects of pregnancy. Increased monitoring or participation in PORTO may also have partially but not entirely ameliorated stress associated with AEDF diagnosis. Women with AEDF may represent a particularly vulnerable population that would benefit from additional support. It would be useful in future studies to include comparison groups of women with low-risk pregnancies to determine whether regular monitoring or study participation ameliorates pregnancy-specific stress, and whether this differs by medical risk severity.
Maternal pregnancy-specific stress may also trigger an inflammatory state characterised by increased nitric oxide (NO) and corticotrophin-releasing hormone (CRH), which may result in decreased resistance to blood flow in the UA. Research suggests that stress triggers an NO upregulation, chronic stress is associated with vasodilation, NO inhibition increases umbilical-placental vasoconstriction and decreases umbilical blood flow, and abnormal UA Doppler waveforms are associated with lower NO activity.58–63 Similarly, CRH, a peptide hormone that plays an important role in stress, is also found in human placentas,64 is partly mediated by NO65 and is one of the most potent fetal vasodilators.66 There may be an adaptive placental mechanism in which increased CRH release to the fetus is triggered by fetal hypoxia or acidosis.67–69
Due to insufficient studies that comprehensively measure biopsychosocial factors in relation to haemodynamics in pregnancy, it is only possible to theorise about reasons for associations between pregnancy-specific stress and fetoplacental haemodynamics. Because pregnancy-specific stress was not measured in the current study prior to recruitment to a study about higher-risk pregnancy, and women in PORTO were not blinded to their Doppler results, it is not possible in the current analyses to determine whether increases in pregnancy-specific stress caused the haemodynamic changes or adverse neonatal outcomes observed. Future studies would benefit from measuring maternal mental health variables prior to the first Doppler ultrasound assessment. There is also a need for additional research examining potential associations among psychosocial data, haemodynamics and biomarkers. Future studies would also benefit from a more multidimensional approach to prenatal stress,70–72 measuring racism exposure,4 73–75 chronic stress, major life events,76 health-related behaviours,71 domestic violence exposure,77–79 resilience80 and partner/social support.76 80–82 Such studies would contribute to a more nuanced, biopsychosocial model of obstetric research. Moreover, future studies assessing associations between maternal mental health and fetal and infant well-being in the context of SGA or growth-restricted pregnancy would benefit from including fetal biometry, uterine artery Doppler velocimetry and analysis of placental histomorphology.
This study has several limitations. Inconsistent sample sizes at each time point limit immediate clinical utility, result in varying statistical power and prevent analyses for all outcomes at all time points. Because the PDQ was not introduced until approximately halfway through PORTO and was not collected in all centres, stress data were not available for the full PORTO cohort and many women did not have stress data collected until late in pregnancy. This may have resulted in selection bias and does not permit generalisation of these findings to other stages of pregnancy. Differences in key clinical characteristics, including pre-eclampsia, GA at delivery, birthweight, Apgar scores at 5 min and NICU admission, suggest that women included in these analyses may have been experiencing somewhat healthier pregnancies than the rest of the PORTO cohort. Relatively low pregnancy-specific stress reported also limits detection of associations between maternal stress and fetal or neonatal outcomes. Women with appropriate for GA pregnancies were also not included in PORTO; these findings may therefore not be generalisable to the general obstetric population. Medication use, illicit substance use, psychiatric diagnoses, domestic violence exposure and whether pregnancies were planned or unplanned were also not recorded. Only three studies linking prenatal stress and haemodynamics in pregnancy excluded women taking psychiatric medication;15 83 84 this is a limitation in the evidence on this topic.85 Likewise, although unplanned pregnancy has been associated with maternal depression and anxiety86–88 and intimate partner violence during pregnancy has been associated with an increased risk of low birthweight and prematurity,89 90 these factors are rarely considered in similar studies.
Importantly, conducting many statistical tests increases the likelihood that significant findings may be false positives. However, the Bonferroni correction was determined to be overly conservative for these analyses for two reasons. First, pregnancy-specific stress was highly correlated across gestation and the tests were therefore highly dependent, which was confirmed in this sample using Pearson’s correlations among the three binned PDQ scores. Second, this is the first repeated, time-sensitive analysis of associations between pregnancy-specific stress and fetoplacental haemodynamics or neonatal outcomes, and in the interest of avoiding type II errors, multiple comparison corrections were not performed. The results presented here should therefore be considered potential targets for future research rather than conclusive indications of the time-specific impact of pregnancy-specific stress on fetal well-being or neonatal outcomes.
This study also has several strengths. Comprehensive, repeatedly collected stress and haemodynamic data were available for a relatively large sample of women, CPRs could be calculated and there were sufficient women with AEDF to allow analysis for most time points. Although analysing stress at three time points reduces statistical power, it allows for time-specific insights into the effects of pregnancy-specific stress on Doppler ultrasound parameters and neonatal outcomes currently lacking in available studies. The overall sample size and sample sizes at each time point in the current study are also relatively large within the context of the available literature on prenatal stress and fetoplacental Doppler velocimetry.12 Moreover, because this was an SGA sample, it was possible to examine associations between maternal stress and abnormal Doppler findings, while most studies to date have reported statistically but not clinically significant associations with continuous outcomes. None of the 12 studies reporting associations between prenatal stress and Doppler ultrasound also reported neonatal outcomes.12 Factor scores also permit novel insights about stressors faced by women with complicated pregnancies. This study further benefited from including ethnicity and deprivation index scores as potential confounding variables. Despite evidence linking socioeconomic status and pregnancy complications,48–53 few of the 12 previous studies adjusted for socioeconomic factors.
In summary, this study presents findings that pregnancy-specific stress was associated with increased odds of AEDF and abnormal MCA PI and reduced odds of abnormal UA PI and NICU admission in 331 women with SGA pregnancies. This study represents a valuable addition to research into associations between maternal prenatal stress and fetal and neonatal outcomes due to its relatively large sample sizes, comprehensive data collection, repeated design, clinically useful dichotomisation of normal/abnormal blood flow and analysis of both overall stress and three specific stressors. These findings suggest that pregnancy-specific stress can be associated with fetoplacental haemodynamics and neonatal outcomes in women with SGA pregnancies, and merits further research attention.
Acknowledgments
The authors thank the women who participated in the PORTO study, Dr Fiona Lynn for pregnancy-specific stress data entry, Dr Oliver Perra for data analysis guidance and the team of Perinatal Ireland research sonographers: Amanda Ali, Annette Burke, Fiona Cody, Emma Doolin, Phyl Gargan, Azy Khalid, Cecelia Mulcahy, Hilda O’Keefe, Wendy Ooi and Edel Varden.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
Footnotes
Contributors TAL made substantial contributions to the analysis and interpretation of the data for this manuscript, drafted the initial manuscript, revised it critically for important intellectual content, approved the final version for publication and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. REG, FAA and FMMcA made substantial contributions to the analysis and interpretation of the data for this manuscript, revised the manuscript critically for important intellectual content, approved the final version for publication and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. FAA and FMMcA also made substantial contributions to the conception and design of the work and the acquisition of the data for this manuscript. RS made substantial contributions to the analysis and interpretation of the data for this manuscript, revised it critically for important intellectual content, approved the final version for publication and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. SD, MPG, MMK, KO’D, AH, JJM, GB, PD, ECT and FDM made substantial contributions to the conception and design of the work and the acquisition of the data for this manuscript, revised it critically for important intellectual content, approved the final version for publication and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding TAL held a PhD studentship from Queen’s University Belfast in Northern Ireland, UK. The PORTO study was conducted by the Perinatal Ireland Research Consortium, a nationwide collaborative research network comprising of the seven largest academic obstetric centers in Ireland. The study was funded by the Health Research Board (HRB).
Competing interests None declared.
Ethics approval Institutional Review Boards at all participating centres.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors welcome requests for any unpublished data associated with this study.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with 'BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected theseerrors and the correct publishers have been inserted into the references.