Article Text

Abstract
Introduction Older patients frequently undergo operations that carry high risk for postoperative complications and death. Poor preoperative communication between patients and surgeons can lead to uninformed decisions and result in unexpected outcomes, conflict between surgeons and patients, and treatment inconsistent with patient preferences. This article describes the protocol for a multisite, cluster-randomised trial that uses a stepped wedge design to test a patient-driven question prompt list (QPL) intervention aimed to improve preoperative decision making and inform postoperative expectations.
Methods and analysis This Patient-Centered Outcomes Research Institute-funded trial will be conducted at five academic medical centres in the USA. Study participants include surgeons who routinely perform vascular or oncological surgery, their patients and families. We aim to enrol 40 surgeons and 480 patients over 24 months. Patients age 65 or older who see a study-enrolled surgeon to discuss a vascular or oncological problem that could be treated with high-risk surgery will be enrolled at their clinic visit. Together with stakeholders, we developed a QPL intervention addressing preoperative communication needs of patients considering major surgery. Guided by the theories of self-determination and relational autonomy, this intervention is designed to increase patient activation. Patients will receive the QPL brochure and a letter from their surgeon encouraging its use. Using audio recordings of the outpatient surgical consultation, patient and family member questionnaires administered at three time points and retrospective chart review, we will compare the effectiveness of the QPL intervention to usual care with respect to the following primary outcomes: patient engagement in decision making, psychological well-being and post-treatment regret for patients and families, and interpersonal and intrapersonal conflict relating to treatment decisions and treatments received.
Ethics and dissemination Approvals have been granted by the Institutional Review Board at the University of Wisconsin and at each participating site, and a Certificate of Confidentiality has been obtained. Results will be reported in peer-reviewed publications and presented at national meetings.
Trial registration number NCT02623335.
- communication
- question prompt list
- geriatric surgery
- shared decision making
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Each year, many of the 500 000 older Americans having high-risk surgery1 2 will do so without fully understanding how it will impact them. Given operative trends for patients age 65 and older,3 4 this number is expected to grow as the US population ages. Although major surgery has potential to prolong life and improve symptoms, it can have unwanted outcomes for older adults, including reduced quality of life,5 more hospitalisations6 7 and potential suffering at the end of life.8 9 Furthermore, 50% of patients 65 and older have one or more chronic conditions,10 putting them at greater risk than younger patients for death and postoperative complications11 12 that necessitate intensive care or lengthy hospitalisations.13 14 Therefore, a decision to proceed with surgery can initiate a care trajectory that is ultimately inconsistent with personal preferences and goals, for example confinement in a nursing home or prolonged life support in an intensive care unit. Patients whose postoperative expectations are not met may suffer as they try to make sense of their situation, feel a loss of control and assume self-blame.15 For these reasons, the decision-making process for older patients considering high-risk surgery is complicated, and because the consequences of these decisions also affect family members, the stakes are high.
Current communication practices inadequately support preoperative decision making about major surgery. According to the Institute of Medicine,16 most patients prefer to share in decision making; however, ‘they are often not afforded the chance to participate’ (ch3, p38),16 and studies suggest that surgeons rarely employ a cooperative decision-making process.17–19 Instead, surgeons rely on best practices, specifically informed consent, to disclose procedural risks and help patients make choices. However, existing decision-making standards do not adequately engage patients in deliberation, and the process of informed consent fails to explain how a patient might actually experience complications, or even expected downstream outcomes, such as the need for additional invasive treatments or predictable changes in functional status.20 21 To make value-laden decisions, patients and families need to know what the outcomes of surgery mean for them and how surgical treatment can be understood in the context of their overall prognosis, particularly for patients with other chronic illnesses.22 23 To be successful, this process requires partnership; surgeons need patients to share what matters to them, and patients need surgeons to help them compare treatment options and evaluate their effectiveness based on patients’ values and goals.
We designed a multisite, cluster-randomised trial of an intervention to improve preoperative communication between surgeons and older adults considering major vascular or oncological operations. Our study evaluates a question prompt list (QPL) intervention for use in the surgical clinic that our research group developed with input from patients, families and surgeons who have experience with high-risk surgery. The intervention aims to encourage patients and families to ask questions that allow them to compare treatment options and get information about how surgery might impact their lives. First, we discuss the rationale and theoretical foundations of the surgical QPL intervention. We then describe the research protocol together with details of study design, data collection, outcomes and analysis plan.
Current gaps in communication about high-risk surgery
To gain a better understanding of usual practice, our research group analysed over 90 preoperative conversations between surgeons and patients considering high-risk cardiovascular, oncological and neurosurgical procedures as part of a multi-institutional study.18 21 24 Analysis of these conversations revealed three primary barriers to decision making. One, surgeons employ a ‘fix-it’ model25 by describing the patient’s disease as an isolated abnormality linked directly with a surgical solution. This model supports an implicit message about the ‘benefits’ of surgery: the reason to operate is to fix what has been identified as broken, and the language implies the patient will return to ‘normal’ after the problem has been fixed. However, this ‘fix-it’ model lacks an explicit description about what surgery might mean more broadly, for example how surgery will impact the patient’s functional independence or other health problems. Lack of context regarding their overall health state makes it challenging for patients to understand the need to deliberate about the value of surgery given their chronic health conditions and quality-of-life preferences.18 Two, surgeons present their own evaluation of the trade-offs associated with the proposed intervention. Surgeons struggle to elicit patient preferences, and efforts to encourage questions are often ineffective as patients regularly respond with logistical or technical concerns, for example what time surgery will take place or whether stitches or staples will be used. The result is surgeon-generated assumptions about the value of specific outcomes and acceptability of trade-offs.18 Three, informed consent requires surgeons to convey risks that are typically described as objective estimates of isolated physiological harms, for example a 45% chance of renal failure. However, this approach does not describe outcomes in a way that allows patients and families to understand what life might be like after surgery.21 These three barriers highlight the need to bridge the gap between what surgeons know and what patients understand about treatment outcomes. These findings complement work by Blazeby and colleagues who have observed that surgeons emphasise in-hospital risks and technical aspects of the procedure rather than long-term functional outcomes.26 27
We also drew from our previous work using physician surveys28–31 and qualitative interviews with surgeons32 to identify a fourth problem with preoperative communication. Our research group has previously described ‘surgical buy-in’, whereby surgeons operate under an assumption that the patient has agreed to both the surgical procedure as well as all postoperative care anticipated by the surgeon, including life-supporting treatments.28 32 While this implicit contract is understood by surgeons, it is not recognised by patients who may desire treatment limitations based on their evaluation of certain health outcomes.24 This disconnect can result in postoperative conflict between surgeons, patients and families33 34 when patients or surrogates on behalf of patients request to forgo aggressive treatments which the surgeon believes the patient agreed to preoperatively.
Development of an intervention to improve preoperative communication
QPLs have proven efficacy for improving patient–doctor communication. QPL interventions can effectively change how patients and families communicate with physicians, improve patients’ and family members’ psychological outcomes, and better meet patients’ informational needs.35–37 Effective QPL interventions require physicians to endorse and support the patient’s use of the question list, but do not require resource-intensive adjuncts like patient navigators or patient coaching.38 For patients considering surgery39 and those with life-limiting illness,40 QPLs effectively increase the number of questions about prognosis and facilitate better alignment between treatment expectations and likely outcomes. These interventions also produce behaviour change in physicians, including surgeons,39 so that patients receive more information about treatment alternatives and attention to personal preferences.41
We met regularly for 10 months with a dedicated group of patients and family members to design a QPL specifically targeting the preoperative decisional needs of patients considering high-risk surgery.42 Our research group gathered over 300 questions from publicly available ‘questions to ask your surgeon’ and focused on three patient-mediated targets identified by our patient and family advisors: ‘Should I have surgery?’, ‘What should I expect if everything goes well?’, and ‘What happens if things go wrong?’ (figure 1). We discarded questions that were either redundant or irrelevant to these targets and used feedback from our patient, family, surgeon and hospital stakeholders to refine the list to create a surgical QPL brochure containing 11 questions. Details of the QPL development have been previously published.42

Patient and family stakeholder-proposed question prompt list targets and resulting goals.
Theoretical framework underlying the QPL intervention
Based on the theories of self-determination43 and relational autonomy44 45 described by Elwyn et al,46 QPLs aim to overcome structural and interactional barriers and promote patient activation, thereby increasing patient engagement in decision making. Given the transactional nature of the patient experience,47 activated patients will receive more patient-centred care and take part in more collaborative decision making, even within the same provider. By supporting patients’ need for autonomy and relatedness, interventions — such as a QPL — to help patients gain knowledge about treatment options offer a strategy to promote patients’ self-perceived capacity to engage in treatment decisions.48
Randomised comparative effectiveness study
Our intervention consists of the surgical QPL and a brief letter from the surgeon endorsing its use, mailed to the patient in advance of the clinic appointment. The intervention targets patients and family members in the preoperative period and seeks to impact (1) patient engagement in decision making for high-risk surgery, (2) psychological well-being and post-treatment regret for patients and family members and (3) interpersonal and intrapersonal conflict relating to treatment decisions and received treatments (figure 2). We hypothesise that through patient activation the intervention will:
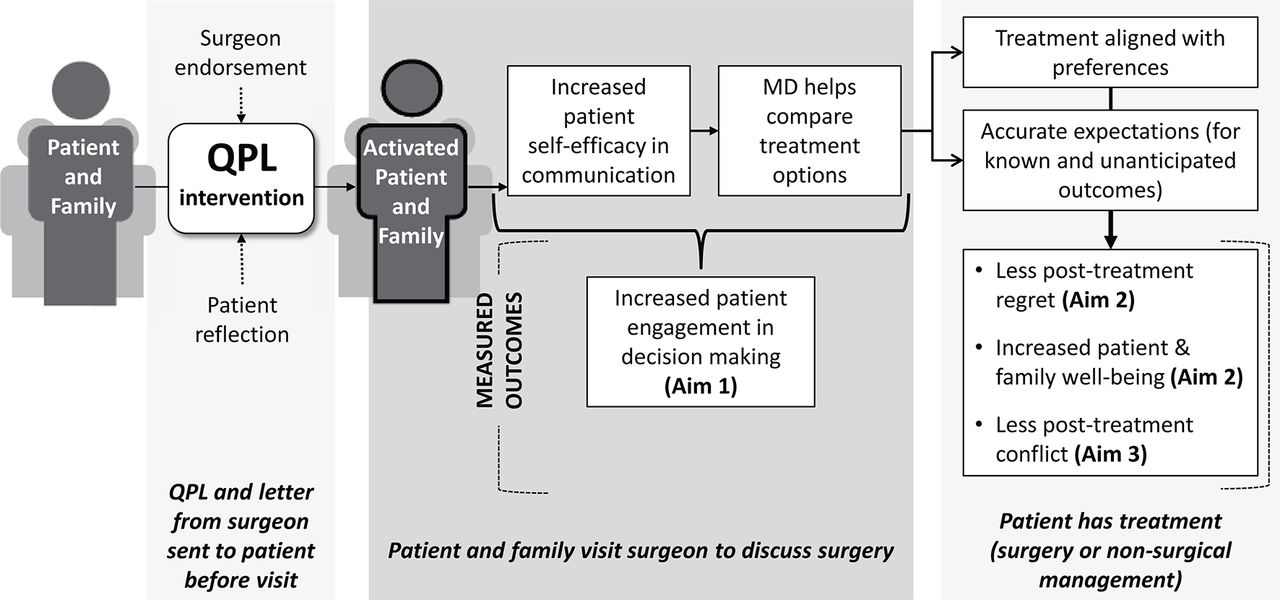
Theoretical framework behind the QPL intervention and the study design. MD, medical doctor; QPL, question prompt list.
improve patient self-efficacy in communication so patients can engage with surgeons in deliberation over treatment options
enable patients to share in decision making so that treatment decisions are aligned with their preferences
promote accurate patient expectations for both known and unanticipated outcomes
reduce post-treatment regret for patients and family members through increased participation in decision making
increase patient’s and family member’s psychological well-being
reduce postoperative conflict between surgeons, patients and families for patients who have an unwanted outcome.
Methods and analysis
Setting and design
This study is a multisite, prospective, cluster-randomised trial using a stepped wedge design49 to compare the effectiveness of the surgical QPL intervention with usual care for older patients considering high-risk vascular and oncological procedures. We are conducting the study in the outpatient surgical clinics at five high-volume academic medical centres across the USA: University of Wisconsin Hospital and Clinics (Madison, Wisconsin), University of California San Francisco (San Francisco, California), Brigham and Women’s Hospital (Boston, Massachusetts), Rutgers New Jersey Medical School/The University Hospital (Newark, New Jersey) and Oregon Health Sciences University Hospital and Clinics (Portland, Oregon). We selected these five sites to represent distinct geographical regions and demographic groups in order to capture diverse experiences with surgical decision making.
Participating surgeons from these five centres routinely perform high-risk oncological or vascular surgery. Patients and family members are invited to participate as dyads. However, patients may participate alone while family members can only enrol with a corresponding patient. We will enrol patients in each surgeon’s clinic according to a stepped wedge design implemented in six 4-month waves over a 24-month period (table 1). In wave 0, all patients will receive usual care. With each subsequent wave, 8 of the 40 enrolled surgeons will cross over into the intervention group. Once a surgeon has entered the intervention arm, all patients scheduled to see that surgeon in clinic to discuss a new surgical problem will receive the QPL intervention. We will audio-record the surgeon–patient conversation in clinic, and patients and family members will complete questionnaires at three subsequent predefined time points. In addition, we will perform qualitative interviews with a subset of participants who experienced serious postoperative complications.
Stepped wedge study design: 40 surgeons at five sites
Participants
Attending surgeons at participating sites who routinely perform high-risk vascular (peripheral, neurological or cardiovascular) or oncological operations on older patients will be invited to participate. Eligible patients are age 65 years and older with one or more chronic health conditions who have an outpatient consultation with a study-enrolled surgeon to discuss a new surgical problem. The surgical problem must be vascular or oncological in nature and could be treated with one of the 227 ICD-9-coded procedures our research group previously defined as high risk.50 For each enrolled patient, we will approach one family member to participate who is present during the conversation with the surgeon in clinic. Eligible participants must be English-speaking or Spanish-speaking and able to converse with the surgeon without an interpreter (aside from Spanish-speaking participants who may use an interpreter), have self-reported visual acuity and literacy skills sufficient to read a newspaper, and be able to provide written informed consent. Patients who do not have a problem that can be potentially treated with surgery, for example an aneurysm that does not meet size guidelines for operative repair, will be excluded based on chart review or previsit determination by the surgeon.
Recruitment
At each study site, all eligible surgeons will receive an invitation via e-mail by the site principal investigator. Surgeons who do not opt out will be chosen first based on surgical subspecialty to capture variability in high-risk procedures and second by random selection of surgeons within a given subspecialty. Surgeons will not receive incentives for participation. We aim to enrol 40 surgeons in total, with the number of surgeons selected to be approximately proportional to the surgical volume at each site.
Study staff will review the clinic schedule of each enrolled surgeon and identify eligible patients based on chart review and clinic intake forms. On the day of clinic, study staff will meet with interested patients and family members to explain the study and obtain informed consent prior to the conversation with the surgeon. Patients and family members will receive financial incentives valued at $55 for participation. To avoid over-representation of any one surgeon, after each surgeon has two patients enrolled within the 4-month wave, recruitment will cease for that surgeon’s patients until the next wave begins. We aim to enrol a total of 480 patients across all five sites, with 12 patients per surgeon.
We will use stratified purposeful sampling to identify a subset of enrolled patients (and family members, if applicable) who underwent surgery and experienced a serious postoperative complication, as determined by chart review. Serious complications include prolonged hospitalisation (more than 8 days postoperatively), prolonged length of stay in intensive care (greater than 3 days), prolonged mechanical ventilation, myocardial infarction, major cerebral vascular accident, new-onset dialysis or death.12 38 We will invite these patients and family members to participate in a face-to-face qualitative interview within 30 days after surgery. We will continue to interview patients until we reach saturation, meaning that data from subsequent transcripts become redundant with developed concepts. We anticipate this will occur with a sample of approximately 20 patients per study arm based on previous studies.18 21
Randomisation and blinding
Surgeons will be stratified by study site and randomly assigned within each site to cross over from usual care to the QPL intervention in different study waves. On study commencement, a master’s level statistician established a step-wise randomisation using a computer-generated randomisation schedule for the list of enrolled surgeons by site. The schedule determined the crossover wave for each surgeon and was designed to balance transitions to the intervention arm across sites in each wave according to the design in table 1. Surgeon crossover will occur in one direction only, and each within-site change will happen once every 4 months during the 24-month duration of the study. A 2-week hiatus in data collection at the start of the crossover will be instituted in transitioning clinics to ensure patients in the intervention group have had the opportunity to receive the QPL and endorsement letter from the surgeon. Study staff will notify enrolled surgeons prior to the upcoming crossover as the intervention is dependent on surgeon endorsement. We expect negligible contamination between study arms as the intervention requires surgeon endorsement of the QPL. Only patients whose surgeons have crossed over into the intervention arm will receive the QPL and surgeon endorsement letter in the mail prior to consultation. Although patients in the control arm may access question lists from outside sources, our prior observational studies confirm surgeons do not routinely endorse the use of question prompts.
Whereas surgeons are not blinded to the intervention, every effort will be made to maintain blinding for patients and family members. Participants will be told the goal of the study is to evaluate communication between surgeons and patients, but they will not be informed about the distribution of the QPL. Transcriptionists and qualitative interviewers will be blinded to the intervention status of each encounter. Study staff are tasked with assuring the QPL has been sent and providing regular reminders to the surgeon to endorse the QPL with all new patients. Study staff will not know if the patient has received the QPL at the time of enrolment but will not be blinded during data collection. In an attempt to insulate study staff from group assignment during data collection, they will strictly adhere to a script and enquire about receipt of the QPL (with all patients regardless of group assignment) 1 day after enrolment following administration of the first questionnaire. Furthermore, data collected from chart abstraction will be reviewed by a blinded clinician for 10% of the sample to ensure accuracy of data entry.
Intervention
Our intervention consists of the QPL brochure and a letter from the patient’s surgeon encouraging its use. The surgical QPL contains 11 questions to help patients and families (1) make treatment decisions in line with their values and goals, (2) anticipate and make sense of postoperative outcomes and (3) experience less postoperative conflict about treatment of serious complications. Once a surgeon has crossed over into the intervention arm, all of his or her patients with a new vascular or oncological problem will receive the QPL intervention via US mail prior to the scheduled clinic appointment. To ensure that there is sufficient time for patients to receive the QPL intervention, we will only recruit patients who have been identified as eligible at least 5 days in advance of their appointment. This timeframe will remain consistent for both control and intervention patients as those who are scheduled more urgently may be systemically different.
Data collection
Audio recording
We plan to audio-record and transcribe verbatim one conversation between the attending surgeon, patient and accompanying family member(s). In order to capture the primary decision-making conversation, this may occur during either the first or second clinic visit depending on the usual practice pattern of each surgeon. Prior to study commencement, each surgeon will select their usual approach: either (1) treatment decisions are typically made during the first clinical encounter, or (2) treatment decisions are typically made during the second clinic visit.
Patient and family member questionnaires
After the primary decision-making conversation with the surgeon, patients and family members will receive three questionnaires. Study staff will conduct follow-up phone interviews to administer the first questionnaire within 24–48 hours of the patient’s clinic visit. Patients and family members will complete these questionnaires independently. Administration of two subsequent questionnaires will be linked to the treatment plan and administered via phone or e-mail based on patient preference. For patients who receive surgery, questionnaires will be administered at 1–2 weeks and 6–8 weeks postoperatively. For those who undergo medical management or observation, questionnaires will be given at 6–8 weeks and 12–14 weeks following the clinic visit. We deliberately chose this timing to create similar administration schedules regardless of whether the patient pursues surgery (figure 3). We allow for up to six contact attempts at each time point.

{kind=link}
{kind=link}
{kind=link}
Screening, recruitment, enrolment and data collection points for patients in the control and intervention arms at each site.
Chart review
Study staff will use chart review to record clinical data, treatments received and outcomes of treatment. Data collected will be limited to clinical information pertaining to surgical care from the initial visit through to administration of the final survey. Data collected from chart review and questionnaires will be stored using the REDCap (Research Electronic Data Capture) software hosted at the University of Wisconsin.51
Qualitative interviews
For patients who suffer serious postoperative complications, a trained interviewer from each centre will perform a face-to-face interview with the patient, if able, and/or the family member. Interviews will be audio-recorded and transcribed verbatim.
Outcomes
Aim 1: patient engagement
To assess patient engagement in decision making, we will use direct observation and patient report measured using a coding scheme established by Walczak and colleagues35 and the Perceived Efficacy in Patient–Physician Interactions (PEPPI-5) scale as our primary outcome measures. From transcriptions of the clinic conversations, two blinded and trained coders will independently count all questions, cues and concerns mentioned by the patient and all family members, friends or other caregivers present during the conversation. Our secondary outcomes for patient engagement include the Observing Patient Involvement score52 53 used for the recorded conversation, and the Health Care Climate Questionnaire (HCCQ)54 administered to patients and family members at the time of the first questionnaire 24–48 hours after the visit with the surgeon. We adapted both the PEPPI-5 and the HCCQ for use by family members (table 2).
Primary and secondary outcome measures (items in bold are primary outcomes)
Aim 2: psychological well-being
We selected psychological well-being as an important outcome based on feedback from our patient and family stakeholders who reported significant emotional harm; specifically they felt ‘blindsided’ when surgical results did not match their expectations. The primary outcome measures to assess psychological well-being are the Measure Yourself Concerns and Wellbeing (MYCaW) and patient-reported post-treatment regret. MYCaW is a patient-reported outcome measure originally designed for patients with cancer and their family members, which we have adopted for use with patients who have vascular disease. MYCaW allows patients and family members to identify their own most pressing health concerns and rate their well-being. We will administer the MYCaW at the three time points. Patients and family members will report their initial responses to the MYCaW at the time of the first questionnaire, 24–48 hours after the clinic visit. Participants will independently rescore their initial concerns and well-being at the two subsequent time points corresponding to the second and third questionnaires; the difference in scores describes improvement or deterioration in their well-being. To assess treatment-associated regret, we will ask patients and family members at the time of the third and final questionnaire — ‘Looking back, is there anything about your treatment/your family member’s treatment that you would do differently?’ — and transform responses into a dichotomous variable (regret, no regret) for analysis.55 We will also analyse these responses qualitatively.
Secondary outcome measures include validated measures from the Patient-Reported Outcomes Measurement Information System (PROMIS) to assess the psychological impact of illness from the patient’s perspective.56 Patients will receive the Psychosocial Illness Impact-Neg 4a, Psychosocial Illness Impact-Pos 4a and Anxiety 4a; family members will be asked to complete Anxiety 4a and PROMIS short form (SF) Global Health. Because studies of other interventions that support shared decision making show that in some situations informed patients elect more conservative treatment,57 we will compare the total number of operations scheduled and performed on enrolled patients by their study surgeon between the control and intervention groups. We will also collect information about potential mediating variables and covariates described in table 3.
Mediating variables and covariates
Aim 3: postoperative conflict
In qualitative interviews with a subset of participants who suffered a serious postoperative complication, we will use questions designed to explore the content of patient and family experience with perioperative conflict. The interview guide is structured around open-ended questions about perioperative events, including ‘Tell me the story of your experience with surgery’.58 The interviewer will follow up the respondents’ narrative description with probing on the following domains: patient and family values and goals, decision making, interpersonal relationships (between surgeons and patients/family members, between treating physicians and between family members) and intrapersonal conflict (relating to post-treatment regret and self-blame). We will use feedback during concurrent coding and analysis to prompt additional questioning on emerging themes and trends.
Planned analyses
Quantitative analyses
Our primary analysis will compare the effectiveness of the QPL intervention relative to usual care in regard to patient engagement and patient psychological well-being. We will use an intention-to-treat analysis with all available data from participants based on group assignment. The intervention effect will be tested in the framework of generalised linear mixed-effects models59 60 with a treatment dummy variable, surgeon random effect and site-by-time dummy variables to control for site-specific secular trends. We will use linear mixed-effect models for continuous responses such as self-efficacy (PEPPI-5) and well-being (MYCaW), logistic random-effects models for binary responses such as post-treatment regret, and log-linear random-effect models for count-dependent variables such as the number and type of questions asked during the preoperative visit. For linear models, we will adjust for prespecified covariates to increase the statistical precision of our treatment effect estimation.
Our secondary analyses will examine other patient endpoints such as psychological well-being (PROMIS measures) and nature of treatment received. These analyses will also test for intervention effects in family member outcomes such as PEPPI-5, HCCQ, MYCaW, post-treatment regret and psychological well-being. We will use the generalised linear mixed modelling framework used in primary analyses for these outcomes. All models will be estimated and tested using PROC MIXED or PROC NLMIX in SAS V.9.3.
We will perform additional analyses to test and quantify whether and to what extent the effect of the QPL intervention on patient engagement outcome measures is mediated by the presence of a family member during the visit with the surgeon. Exploratory analysis of family-reported outcomes will occur independently of patient-reported outcomes. To accomplish this, we will compare the indirect effect with the total effect in joint linear structural equation models for the endpoint and the mediator, including correlated random surgeon effects for each of the mediator and endpoint parts of the models. In addition, we anticipate treatment effect could vary across subpopulations defined by the following covariates: indication for surgery, patient comorbid illness and insurance status. Therefore, we will test the effect of treatment separately in subpopulations defined by these variables.
To decrease missing data, we limited the number of questions in the follow-up questionnaires and will provide a bonus incentive for participants who complete all three questionnaires. At the time of analysis, we will develop a comprehensive description of the missingness patterns and develop a plan for imputation that leverages the available data and concentrates on the data most heavily subject to missingness. If data are missing on predictor variables of interest, values will be imputed using multiple imputation techniques (ie, chained equations imputations).61 62 If dropout is substantial, we will again use multiple imputation, including exploiting responses from the first two time points (day of clinic visit and 24–48 hours postvisit), to impute responses from the final two questionnaires, to maximise statistical efficiency and to minimise bias.
Sample size and power calculation
Each arm will contain 240 patients, for a total of 480 patient participants. Based on our prior work, we expect about 70%–80% of patients will have a family member present who will participate. Therefore, we estimate 384 family members from all sites will partake, although we will enrol up to 480 family members if all patients have a family member interested in participating. Assuming all enrolled patients enrol with a family member, the maximum number of all possible participants (surgeons, patients and family members) is 1000.
For each quantitative aim, we desire a family-wise two-sided type I error rate of α=0.05; under a Bonferroni correction, tests will be conducted with nominal α=0.05/2=0.025 because there are two primary endpoints for aim 1 and aim 2 (table 2). Using patient satisfaction data at one site, we found that between-surgeon variance accounts for only 5% of the total variance. Because power in the stepped wedge design is slightly degraded with greater variance between (vs within) surgeons, we assumed a worst-case scenario between-surgeon variance of 30%. We interpreted this as the interclass correlation between multiple patients of the same surgeon at a given site and included a surgeon-level random effect in our calculation, anticipating between 5% and 30% of the total variance to be accounted for by surgeon effects (ie, interclass correlation (ICC) =0.05–0.30). Extending the information-based method of computing power for a basic stepped wedge design49 to the case of our multisite stepped wedge design, we custom-programmed power calculations using R V.3.2.1 (R Foundation for Statistical Computing).
With this method, we computed power of 82% to detect small-to-medium and 93% to detect medium effect sizes of Cohen’s d63=0.425 and d=0.5, respectively. Assuming the SD for PEPPI-5 within each treatment arm is 4.3,64 we will have 93% power to detect effects as small as 2.15 points. For the number of patient questions, we assumed a mean difference of 1.4 questions between arms.40 Assuming overdispersion of two relative to Poisson data, within arm SD=2.7, yielding d=1.4/2.7=0.52, which we are well powered to detect. For the MYCaW well-being scale, Jolliffe et al65 found SD=1.26 at 6 weeks, and a 6-week versus baseline mean difference of 0.59. We will also have 93% power to detect an MYCaW difference as small as 0.5×1.26=0.63, comparable with the difference over time in Jolliffe et al.65 For regret, we assume the upper bound risk of the presence of regret is 0.3,55 yielding SD=0.46; we will have over 90% power to detect a regret risk difference of 0.23. Nearly identical power results were obtained via a continuous latent liability model for a binary event (regret).66 To account for clustering within sites, this calculation includes fixed effects terms for site, time (wave) and site-by-time, reflecting our a priori analysis plan.
Qualitative analysis
We will use directed content analysis67 to compare interpersonal and intrapersonal conflict between study arms as it relates to the phenomenon of surgical buy-in.28 32 68 To gain understanding of the trajectory of each patient’s story, we will triangulate data sources by linking the audio tape of the surgeon–patient decision-making conversation and the patient’s clinical history from chart review with the follow-up interview. We have previously shown that surgeons see preoperative conversations as a significant event, a time when a two-way agreement is made whereby the surgeon commits to operating and the patient commits to endure potentially burdensome postoperative care.28 We will use this understanding of surgical buy-in to code and analyse preoperative clinic visits and postoperative interview transcripts with the goal of understanding how the contractual relationship that surgeons perceive is experienced by patients. We will explore how postoperative complications were discussed during the initial patient–surgeon interaction with and without the QPL and whether this interaction has impact on subsequent treatment decisions, interpersonal and intrapersonal conflict.
Ethics and dissemination
Ethical review
All participants will provide written informed consent and may withdraw from the study at any time without affecting the medical care they receive from the clinical team. For surgeons, study participation will not affect their professional standing. Institutional review board approval has been granted at each of the five sites, and a Certificate of Confidentiality has been granted in order to offer enrolled surgeons protection from legal demands, such as subpoenas and court orders for study data. Identifying information on recorded transcripts will be redacted prior to analysis, and all audio recordings and hard copies of data will be destroyed after analysis is complete and manuscripts are submitted. The aims of the study meet the criteria for minimal risk. We will follow accepted adverse event monitoring procedures including regular review by the Data Monitoring Committee.
Relevance and dissemination
The design of the QPL intervention addresses important gaps in preoperative communication between surgeons and older adults facing a decision about high-risk surgery. The results of this study will inform our understanding of how interventions to confront interactional barriers between doctors and patients affect patients’ capacity to participate and share in decision making. The engagement of a variety of stakeholders and incorporation of deeply held concerns of patients and families into the development of the QPL are strengths that create potential for significant impact. Furthermore, should we find the intervention superior to usual care, it is inexpensive and easily scalable to facilitate widespread dissemination in all outpatient clinics where high-risk surgery is considered. We anticipate these results will be generalisable to other surgical settings as well as encounters for patients who have been referred specifically for discussion of other types of treatment, for example in medical or radiation oncology clinics.
Efficacy, however, is contingent upon a letter of endorsement from the surgeon that accompanies the QPL brochure. Furthermore, durable changes in surgeon behaviour as a result of questions and attitudes the QPL engenders in their patients may contribute to the effectiveness of the intervention over time. As such, our dissemination strategies will be targeted primarily at surgeons. We have support of leadership at the American College of Surgeons (ACS) and anticipate dissemination through various ACS portals, including the National Surgical Quality Improvement Program and the Coalition for Quality in Geriatric Surgery, as well as distribution of the intervention and description of the implementation processes on the ACS website. In addition, based on feedback from our patient and family advisors who felt dissemination of results to patients and families is critically important, we will provide study updates and distribute study results via a study website. We plan to present study results at the annual ACS Clinical Congress and local chapter meetings. We plan to publish the main trial outcomes in a peer-reviewed journal. We will follow the CONSORT reporting standards for pragmatic69 and cluster-randomised70 trials. Study results will be released to participating surgeons, patients, families and the general medical community.
Acknowledgments
The authors would like to thank Betty Kaiser, PhD, RN, and Gay Thomas, MA, of the Wisconsin Network for Research Support for guidance in creating and planning the Patient and Family Advisory Council. They would also like to acknowledge the patients and family stakeholders who provided invaluable feedback throughout the development of the QPL intervention and development of study materials.
References
Footnotes
Contributors MLS is the principal investigator for this study. She developed the original study design and protocol together with PJR, who provided study design and biostatistical support, and the site principal investigators ZC, AnaB, ACM, EF and KJB. NJ provided guidance in study design specific to the qualitative components. QZ provided biostatistics support. AnneB is the study coordinator and has the primary responsibility of coordinating development of all study materials. LJT drafted this manuscript and along with JLT helped with development of study materials. JLT and NMS synthesised input from patient and family stakeholders and contributed to study design. All authors reviewed and approved this manuscript.
Funding Research reported in this work was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (CDR-1502-27462). MLS was also supported by (1) Training Award KL2TR000428 from the Clinical and Translational Science Award program, in part by Grant UL1TR000427 to UW ICTR from NIH/NCATS; (2) through the University of Wisconsin-Madison School of Medicine and Public Health’s Wisconsin Partnership Program, WPP-ICTR Grant #3086; and (3) the Greenwall Foundation Kornfeld grant. LJT is supported by a Training Award T32CA090217 from the NIH. AnaB is supported by the New Jersey Medical School Hispanic Center of Excellence, Health Resources and Services Administration through Grant D34HP26020. This content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors or Methodology Committee.
Competing interests None declared.
Ethics approval The trial protocol and all study forms and material have been approved by the University of Wisconsin Institutional Review Board, as well as the institutional review boards at each participating site.
Provenance and peer review Not commissioned; externally peer reviewed.