Article Text

Abstract
Objectives This study examines in a cross-sectional study ‘the tobacco control environment’ including tobacco policy implementation and its association with quit ratio.
Setting 545 communities from 17 high-income, upper-middle, low-middle and low-income countries (HIC, UMIC, LMIC, LIC) involved in the Environmental Profile of a Community's Health (EPOCH) study from 2009 to 2014.
Participants Community audits and surveys of adults (35–70 years, n=12 953).
Primary and secondary outcome measures Summary scores of tobacco policy implementation (cost and availability of cigarettes, tobacco advertising, antismoking signage), social unacceptability and knowledge were associated with quit ratios (former vs ever smokers) using multilevel logistic regression models.
Results Average tobacco control policy score was greater in communities from HIC. Overall 56.1% (306/545) of communities had >2 outlets selling cigarettes and in 28.6% (154/539) there was access to cheap cigarettes (<5cents/cigarette) (3.2% (3/93) in HIC, 0% UMIC, 52.6% (90/171) LMIC and 40.4% (61/151) in LIC). Effective bans (no tobacco advertisements) were in 63.0% (341/541) of communities (81.7% HIC, 52.8% UMIC, 65.1% LMIC and 57.6% LIC). In 70.4% (379/538) of communities, >80% of participants disapproved youth smoking (95.7% HIC, 57.6% UMIC, 76.3% LMIC and 58.9% LIC). The average knowledge score was >80% in 48.4% of communities (94.6% HIC, 53.6% UMIC, 31.8% LMIC and 35.1% LIC). Summary scores of policy implementation, social unacceptability and knowledge were positively and significantly associated with quit ratio and the associations varied by gender, for example, communities in the highest quintile of the combined scores had 5.0 times the quit ratio in men (Odds ratio (OR) 5·0, 95% CI 3.4 to 7.4) and 4.1 times the quit ratio in women (OR 4.1, 95% CI 2.4 to 7.1).
Conclusions This study suggests that more focus is needed on ensuring the tobacco control policy is actually implemented, particularly in LMICs. The gender-related differences in associations of policy, social unacceptability and knowledge suggest that different strategies to promoting quitting may need to be implemented in men compared to women.
- Tobacco environment
- Tobacco control policy
- Social unacceptability
- Knowledge of tobacco harms
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study provides data from communities from a wide range of countries, particularly low income and middle income countries that have ratified the Framework Convention of Tobacco Control (FCTC), on measures of actual tobacco policy implementation.
It demonstrates that associations of measures of tobacco policy implementation with quit ratio differed by gender. This suggests that different strategies to promote quitting smoking may need to be implemented in men compare to women.
The 17 countries involved were a convenience sample of countries that had diverse economic levels and cultures. The communities in some countries were also convenience samples, from urban and rural regions, designed to capture within-country diversity.
The findings of this study confirm that implementation of tobacco control policies is weak, especially in poorer countries. While the associations described are cross-sectional, they do indicate that more extensive policy implementation, greater social unacceptability and higher levels of knowledge of smoking harms were associated with higher quit ratios
Introduction
Tobacco is one of the leading avoidable causes of death globally.1 An individual's choice to smoke or not is influenced by the environment of the community in which they live. Thus it may be easier to choose to smoke or choose not to quit in a community where tobacco is accessible and the sociocultural norms support smoking.2 A large evidence-base supports the notion that significant reductions in tobacco use require implementation of comprehensive control policies,3 as set out in the Framework Convention on Tobacco Control (FCTC).4 Much of the existing research focuses on the effect of discrete tobacco control measures such as taxation policy,5 ,6 and most studies that examine comprehensive packages of tobacco control look only at individual measures within a single jurisdiction.7 ,8 There are a few exceptions that examine combinations of measures; the US National Cancer Institute's Strength of Tobacco Control (SOTC) index captures tobacco control intensity at state level and correlates with smoking prevalence.9 Similarly the European ‘Tobacco Control Scale’ also correlates with smoking prevalence.10
Tobacco use is growing fastest in low-income countries. Nearly 80% of the world's one billion smokers live in low-income and middle-income countries.11 Yet few studies look beyond high-income countries (HIC) to measure the level of implementation of tobacco control policies or assess whether they are effective in different contexts.12
We sought to add to the literature in the range of tobacco control measures examined and the geographical scope of the research. Consequently, our objective was to examine implementation of comprehensive tobacco control policies in 545 communities in 17 countries in the Americas, Europe, Asia and Africa, at all levels of development and their association with quit ratios (rate of former to ever smokers), focusing primarily on measures specified in the FCTC.
Methods
Study design and data collection
The Prospective Urban Rural Epidemiology (PURE) study, previously described,13 ,14 is a prospective, standardised collaborative study which, initially, involved 17 countries: 3 HIC: Canada, Sweden, United Arab Emirates (UAE); 7 Upper middle-income countries (UMIC): Argentina, Brazil, Chile, Malaysia, Poland, South Africa, Turkey; 3 Lower middle-income countries (LMIC): China, Colombia, Iran and 4 Low income countries (LIC): Bangladesh, India, Pakistan and Zimbabwe. Economic level was based on World Bank data from 2006.15 This definition followed the convention for papers published from the PURE study which maintained the country classification according to when each country joined PURE. India was one of the first countries beginning recruitment in 2003 and at the time was classified as a LIC.13 All except Zimbabwe (acceded March 2015) had signed the FCTC at the time of the study and, of those that have signed all except Argentina have ratified it. Communities within countries were selected purposively to ensure inclusion of urban and rural settings at diverse socioeconomic levels.13 We have previously described in detail the community definition for the PURE study. In PURE, a community is a group of people who have common characteristics and reside in a defined geographical area. A standard definition was difficult to apply globally, and hence a set of rules were followed to define this for each region.13 Previously analyses of the PURE cohort quantitatively demonstrated that characteristics of participating individuals are broadly representative of countries in which they live.14
The Environmental Profile of a Community's Health (EPOCH) study assesses environmental factors plausibly associated with chronic non-communicable disease risks and includes only communities with 30 or more participants. Here, we report on the 545 of 628 PURE (86.8%) communities with complete EPOCH data. The instruments are described elsewhere,16 ,17 with tobacco-related variables based on our earlier literature.2 In brief, EPOCH assessments have two parts: EPOCH-1 is an objective environmental audit tool with trained researchers directly observing and systematically recording physical aspects of the environment. Tobacco variables consisted of: a 1 km walk in a central community service district in which tobacco outlets, protobacco and antitobacco marketing (health promotion signs about the adverse effects of smoking and promoting quitting) and signs prohibiting smoking (‘no smoking signs’) are counted and a single tobacco outlet is visited to obtain information on point-of-sale (POS) protobacco and antitobacco marketing and signs prohibiting smoking, price of the lowest cost pack of 20 cigarettes and sale of cessation aids. The term antismoking signage refers to the combination of antitobacco marketing and signs prohibiting smoking. EPOCH-1 data were collected between 2009 and 2014, with the majority (94.9%) in 2009–2010.
EPOCH-2 is interviewer administered, capturing perceptions about the community from a random subsample of ∼30 individuals (men and women) among PURE participants demonstrated to be a sufficient sample to reliably characterise measures at the community level.17 It includes social unacceptability of smoking: self-reported observations of smoking in public spaces, intolerance to smoking indoors, disapproval of adults (men or women), youth and children smoking. EPOCH-2 also assesses knowledge of health effects of smoking and asks whether respondents were current, former or never smokers.
Outcome variable
Smoking status was self-reported by EPOCH-2 respondents as current (using cigarettes every/most days), former (having quit prior to the survey) or never smokers. Our primary outcome was quit ratio—ratio of former to ever smokers (current and former smokers combined) at the level of the community, assessed in adults aged 35–70 years participating in EPOCH-2. Complete data were available from 12 805 (of 12 842, 99.7%) individuals in the 545 communities (table 1).
Distribution of communities and participants in the EPOCH 2 study sample
Explanatory variables
EPOCH-1 and EPOCH-2 measures were combined into three scores of different aspects of the tobacco environment. The first score, measuring the main components of FCTC policy implementation, drew on Joossens and colleagues' Tobacco Control Scale (table 2a).10 However, we assessed implemented policies ‘on the streets’ rather than policies on the books. As with Joossens' scale, we allocated most points to price, and roughly equal points to each of ‘comprehensive bans on promotion’, ‘public information’ and ‘direct health warnings’ and a smaller proportion of points to ‘support to quit’.10 However, we added ‘availability’, using numbers of outlets selling tobacco per community, as outlet density and proximity may influence smoking rates and cessation.18 ,19 Our measures used direct observation of whether policies had been enacted in communities while Joossens' ‘public information campaigns’ domain measured national spending on public information. Thus, ours counted signage prohibiting smoking and antitobacco advertisements.⇓
Scores to summate environmental factors related to smoking
The second score (table 2b) captured social unacceptability of smoking in a single measure. We used responses to four items in the EPOCH 2 survey for smokers and non-smokers: (1) more smoking observed in public places indicated higher acceptance of public smoking (2) intolerance of indoor smoking, (3) disapproval of youth smoking and (4) disapproval of adult (men or women) smoking. These were converted into a score (table 2) with responses of smokers and non-smokers equally weighted (to avoid the potential imbalance that might arise where there are many more smokers in some communities than others).
Our third score (table 2b) captured responses to 10 questions on knowledge of health effects of smoking. Knowledge was calculated as average percentage of correct responses, separately for smokers and non-smokers and then averaged.
Each score was divided into quintiles (figure 1). To create an overall score, we ordered communities based on the combination of their 3 scores: we converted the quintile distributions to points (1 to 5) and added these together. Thus, a community in the bottom quintile for 3 scores would have an overall score of 3 but if in the top quintile for 3 scores, the overall score would be 15. We then divided the combined score into fifths based on quintiles of the combined variable.

Distribution of community-level tobacco scores for tobacco policy implementation, social unacceptability and knowledge of smoking health effects by country income group.
Statistical analyses
We conducted descriptive statistics and compared groups using χ2 tests for categorical data and analysis of variance for means. The relationship between community summary scores and quitting was measured using a multilevel regression framework where individuals (level 1) were hierarchically nested in communities (level 2). Logistic regression was used to estimate determinants of the binary response of quitting (y, former smoker vs current smokers) for individual i in community j. Quitting, Pr (yij=1), was assumed to be binomially distributed  with probability
with probability  related to each quintile of the summary scores (
related to each quintile of the summary scores ( ), adjusted for covariates X (age, education) and a random effect for each level by a logit link function:
), adjusted for covariates X (age, education) and a random effect for each level by a logit link function:
 .
.
The term  in brackets represents community level random effects, assumed to be independently and identically distributed with variance
in brackets represents community level random effects, assumed to be independently and identically distributed with variance  .20
.20
Two sets of multilevel models were specified. First, associations between each score and quitting were assessed in age-adjusted models for men and women. Given large sex differences in quit ratios in several countries, we stratified all models by sex following an examination of sex interactions in the effect of scores on quit ratio. A second set of models included education as a proxy for socioeconomic status and a potential mediating factor.
Results
The distribution of communities and participants with smoking rates and quit ratios are in table 1. The overall response rate to the EPOCH 2 surveys was 81% and the mean number of participants per community was 24 and this varied between 7 and 35 by country with 15/17 countries having >20 participants per community.
Policy implementation, social unacceptability and knowledge scores
Average tobacco control policy score was greater in HIC, with a positive skew, while LICs and LMICs showed a negative skew. Social unacceptability scores (higher scores indicate greater social unacceptability or less social acceptability) were greater in HICs with some positive skew, more normally distributed in UMIC and LMIC and were broadly spread in LICs. The Pearson correlation between policy implementation and social unacceptability scores was 0.17. Knowledge of health hazards of smoking score was greater and positively skewed in HIC and UMIC compared to LMIC and LIC (figure 1). Variation in components of each score is described in table 3.
Characteristics of the tobacco environment—community measures
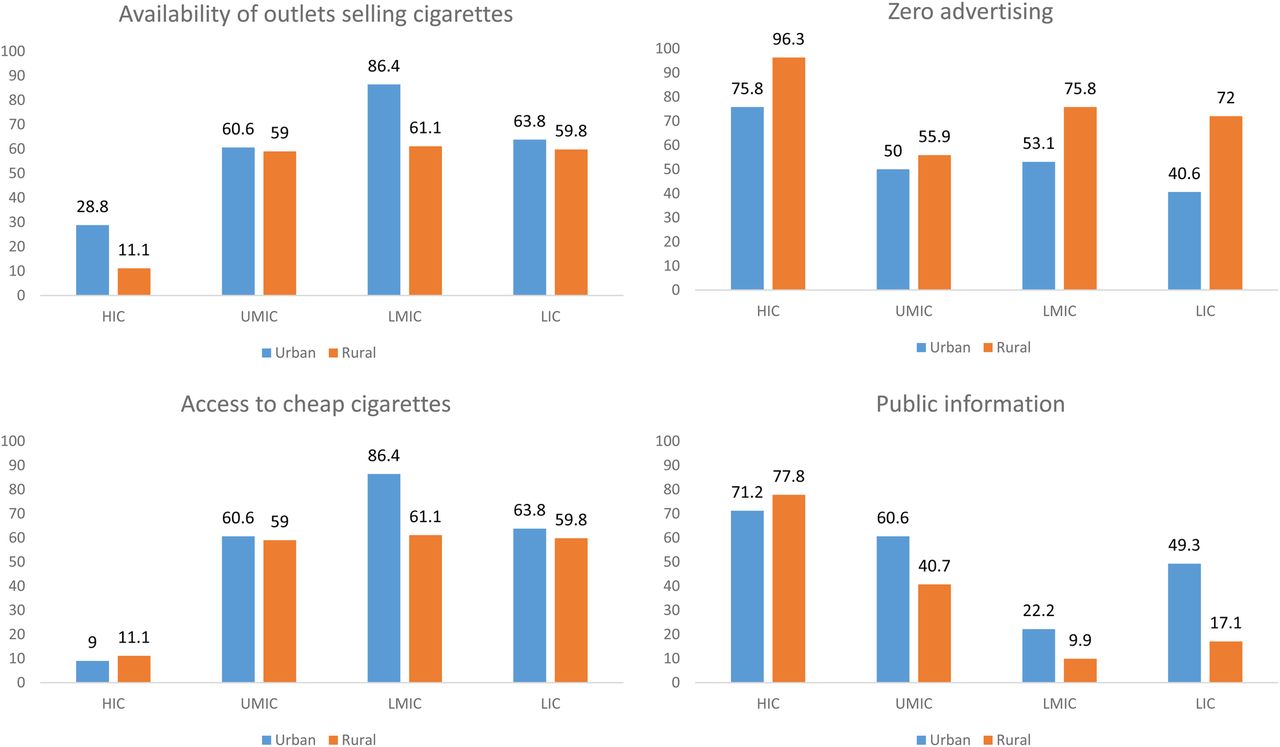
Overall 28.6% (154/539) communities sold cheap cigarettes (<5cents PPP adjusted/cigarette), and 56.1% (306/545) had access to >2 outlets. Access to cheap cigarettes was greater in lower income countries. Effective tobacco bans (no tobacco advertising) were observed in 54.6% (154/282) of communities, and this was greatest in HIC 81.7% (76/93). Antismoking signs were observed in 38.3% (207/541) of communities; 73.1% (68/93) of HIC, 51.2% (64/125) UMIC, 15.7% (27/172) LMIC and 31.8% (48/151) LIC. Urban–rural differences were generally inconsistent, though tobacco advertising was consistently less in rural communities (figure 2).

Tobacco policy in urban and rural communities of high-income, middle-income and low-income countries.
Intolerance of smoking indoors was greater than in public places in UMIC, LMIC and LICs but in HICs intolerance of smoking in public places was greater (eFigure 1). There was overall high disapproval of youth smoking, especially in HIC (92.2%) compared to 75.0% in UMIC, 85.8% in LMIC, 63.7% in LIC (p<0.0001) (eFigure 2).
Average percentage correctness on knowledge items was 74.3%, 87.4% in HIC, 78.9% in UMIC, 66.5% in LMIC and 71.6% in LICs (p<0.001 for trend and p<0.001 for all basic comparisons across economic groups). Knowledge was greater in urban than rural areas, in 60.3% (170/282) of urban communities the average score was >80% compared to 35.7% (94/263) in rural regions. In 97.0% of urban communities from HIC the average score was >80% compared to 22.0% of rural communities from LIC (eFigure 3).
ORs and 95% CIs were obtained from sex stratified, age-adjusted multilevel logistic regression models of the associations between quintiles of each of the 4 tobacco environment scores and individual quitting.
Association with quit ratio
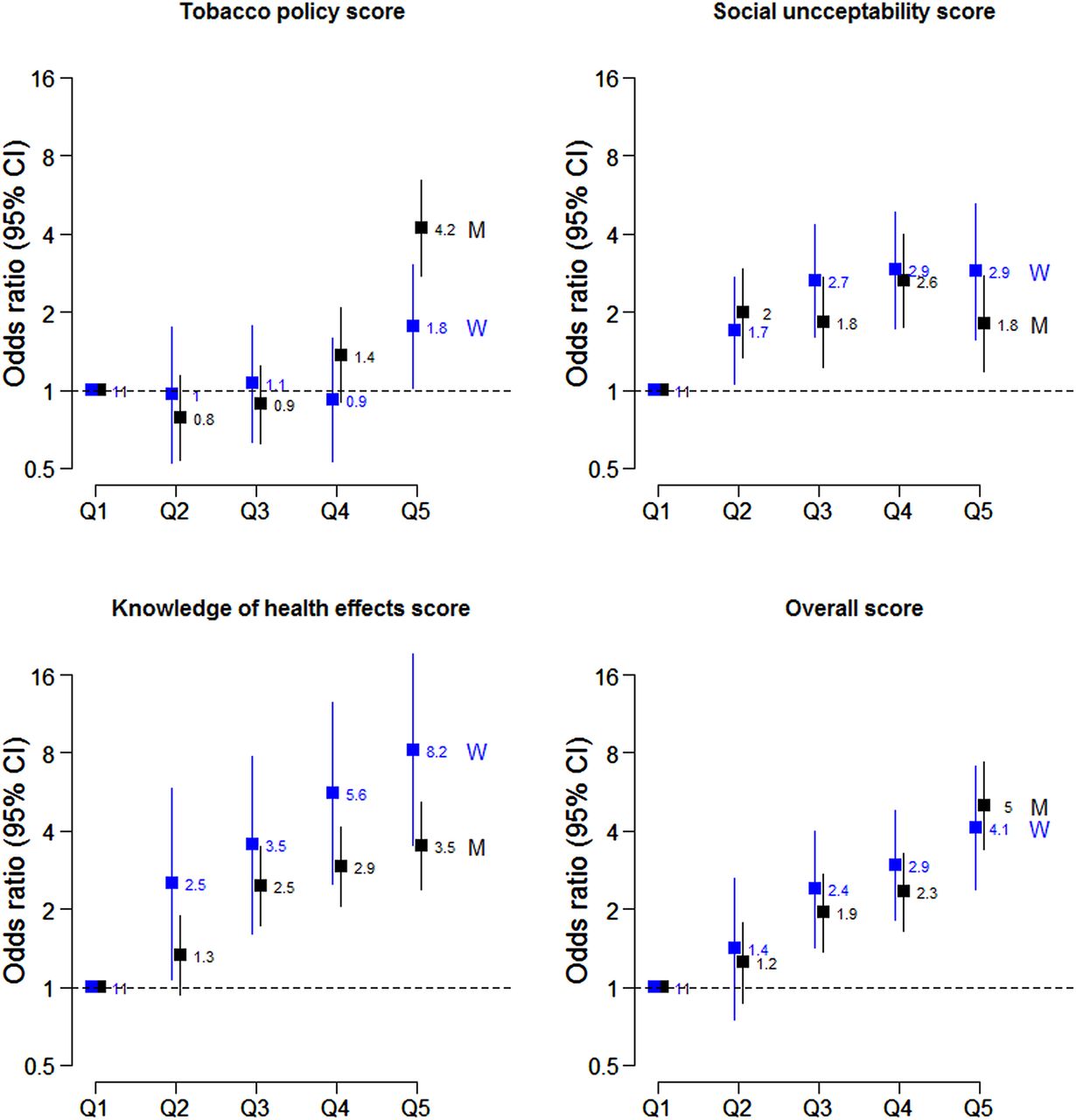
Age adjusted sex stratified models: The odds of quitting increased with increases in all four scores in both genders. There were sex interactions (p<0·001). Communities in the highest quintile of the tobacco policy implementation score had 5.4 times the quit ratio in men (OR 5.4, 95% CI 3.5 to 8.2) and 3.3 times the quit ratio in women (OR 3·3, 95% CI 1.9 to 5.9) (eFigure 4). Higher quintiles of social unacceptability and knowledge scores were both associated with greater quit ratios, with the gradient of association steeper for women than men. The quit ratio in communities in the highest quintile of social unacceptability was 5.0 (95% CI 2.6 to 9.5) times the reference in women and 2.2 (95% CI 1.4 to 3.5) times in men. The quit ratio for women in communities in the highest quintile of knowledge of smoking harms score was 15.1 (95% CI 6.4 to 35.8) times the reference, and for men 4.3 (95% CI 2.9 to 6.4) times.
Age and education adjusted sex stratified models: Additional multilevel logistic regression models were specified for associations between each of the tobacco environment scores and quitting, adjusted for age and education (figure 3). The direction of the associations were largely consistent with age adjusted models, although there was some attenuation in the ORs in some models, particularly for women. This indicates that some of the community level tobacco environmental effects on the quit ratio are mediated by education, particularly in women.

{kind=link}
{kind=link}
{kind=link}
The odds of quitting for quintiles of tobacco environment scores from multilevel logistic regression models adjusted by age and education (M=men and W=women). ORs from multilevel logistic regression models of quitting with random effects specified for communities. Models are age and education adjusted and stratified by sex with separate models fitted for each score. Sex interactions for the effect of summary scores on quitting were p<0.001 in all models.
Finally, the relationship of the overall score to quit ratio showed higher quit ratios for each quintile increase in overall score in men and women as shown in the 4th panel, figure 3. Communities in the highest quintile of the combined scores had 5.0 times the quit ratio in men (OR 5.0, 95% CI 3.4 to 7.4) and 4·1 times the quit ratio in women (OR 4.1, 95% CI 2.4 to 7.1).
Discussion
Summary of findings
This is a cross-sectional study examining the tobacco control environment compared to the rates of quitting smoking in 545 communities selected non-randomly from 17 high-income, middle-income and low-income countries. The key findings are that implementation of tobacco policy is poor and when related to quitting of smoking indicates that more extensive policy implementation, greater social unacceptability and higher levels of knowledge of smoking harms are associated with higher quit ratios. The main limitations are that the associations are cross-sectional and hence it is not possible to determine the direction of causality; also the selected community sampling limit the generalisability of findings.
Despite ratification of the FCTC by 16 of the 17 countries studied, implementation of tobacco policy is poor, especially in middle-income and low-income countries. Comprehensive bans on advertising are not enforced, POS advertising was prevalent, minimum standards in cigarette pack labelling have not been met and cheap and single cigarettes are sold. Social unacceptability is greatest in HICs and knowledge of the health effects of smoking is greater in HICs and UMICs. Communities in the highest quintile of comprehensive tobacco control implementation achieved higher quit ratios, as did those with higher social unacceptability scores and knowledge of health effects of tobacco. Associations with gender were heterogeneous, with tobacco policy scores more strongly associated with quit ratio in men and social unacceptability and knowledge scores more closely associated with quit ratio in women. However, combining all scores, communities achieving higher combined scores had higher odds of quitting in men and women, showing a positive graded association with quit ratio.
What is known and what are the gaps
The FCTC calls for comprehensive tobacco control policies, including raising taxes and prices, restricting marketing, warning about the dangers of smoking and offering help to quit.21 It is not, however, sufficient to enact policies. They must also be implemented and enforced effectively.22 Yet the tobacco industry frequently violates tobacco control legislation, including that restricting its marketing practices23 ,24 and facilitates smuggling to undermine increased taxation.25
While previous research shows that tobacco control policies,26–28 social unacceptability of smoking29 ,30 and knowledge,31 ,32 are all linked to smoking patterns and cessation, it is limited in several ways. Most literature examines the impact of policies without taking account of implementation and enforcement,10 ,33 and examines either individual policies or aspects of the tobacco control environment (eg, social unacceptability alone).33 ,34 Most importantly, given the shift of the tobacco epidemic to LMIC, there has been very little work examining the impact of implementation, social unacceptability and knowledge of harms in LICs. Our findings address these gaps.
What did we observe and how is this significant?
Our main findings support the need to enact comprehensive tobacco control strategies, and to ensure that they are implemented to increase quitting. While quitting rates only became significantly higher once communities reached the highest quintile on the Tobacco Policy Score, the combined score showed a graded increase with quit ratio. Implementation was lower in LMICs, though there was considerable variation within country blocks. There are many possible explanations, going beyond the scope of this paper, but include legislative capacity and governance performance.35 In LMIC, policies can be undermined by the realities of the informal market, illicit trade and tobacco industry behaviour.36 ,37 There may also be differential responsiveness to tobacco control policies. For example, data from China38 suggests less responsiveness of smoking rates to price, compared to other countries such as Korea.39 This may be also due to the changing relative affordability of tobacco compared to a broader basket of goods.40
Second our findings of differing effects by gender may have implications for how and which policies should be prioritised, especially in countries in which there are large differences between male and female smoking rates and quitting rates. We noted a higher overall quit rate in women compared to men, despite it being generally accepted that women are considered to be earlier in the tobacco epidemic, especially in LMIC/LICs. Women's quitting behaviour may also be more responsive to certain policy or environment factors, such as knowledge and social unacceptability. We observed that the degree of social unacceptability and knowledge of the health impacts of smoking are clearly important overall in motivating quitting, but especially so for women. Our findings of gender-related differences are consistent with previous studies,27 ,41–43 and suggest that different strategies to promote quitting smoking may need to be implemented in men compared to women.
Third the argument frequently used by the tobacco industry that everyone now knows the harmful effects of smoking is clearly not true in the global context,44–46 given that only about half of the participants in LIC gave a majority of correct answers on the knowledge of health effects questions, compared with 94·6% in HIC. While education on smoking harms may have reached a ceiling in HICs, the clear and linear trend demonstrated for increasing knowledge of health harms in the population studied here that was dominated by countries from low-income and middle-income regions, shows that promotion of knowledge of the adverse health effects of smoking is likely to be very important in these regions. Knowledge of health effects is greater among those who are generally more highly educated, and while there was attenuation of the association with quitting when adjusting for education, the association of knowledge of smoking harms with quitting was still strong and statistically significant indicating that factors beyond education (but which track with it) are also important influences.
Finally, our findings highlight the importance of measuring actual policy implementation. Limiting assessment of tobacco control policies to assessment of the formal existence of policies is likely to be superficial and poor surrogate measure of policy enactment in many of the regions studied here.
Limitations
First, this study was conducted in a convenience sample of communities and countries participating in the PURE study, where infrastructure existed to enable the necessary data collection. However, convenience sampling is unlikely to impact the finding of associations or the direction of associations found in this study between factors influencing quitting. However, it could potentially impact estimates of the strengths of the various associations and their generalisability across regions. For example, the prevalence of outlets selling tobacco in HIC is only representative of the communities studied and not all communities in HICs. However, unlike earlier studies that have typically been concentrated in a few selected communities from HIC, the sample included communities and countries at all levels of development. This, however, did mean that we had to draw on known constructs to describe the tobacco control environment, most of which have been derived from HICs.10 Our scores have not been formally validated or assessed for reliability, though the scores show face validity based on the literature and measures included in the scores have undergone reliability testing in the development of the EPOCH instruments.16 ,17 The outcome measures of quit ratio are derived from self-reported measures of current smoking and ex-smoking and it was not possible to validate this with objective measures such as salivary cotinine in this large study. However, previous studies indicate that self-reported smoking and quitting is reasonably reliable.47
Second there may be other country/cultural or unmeasured factors, such as political upheaval, that may explain differences in response to tobacco control policies that cannot be completely accounted for by adjustment. On the other hand, our approach, in comparison with other literature that measures policies through secondary data sources, has the advantage that, by directly observing communities, we have been able to capture the ‘implementation’ of tobacco control policies in communities rather than the mere existence of policy which may exist on the books but are not enforced.
Third, as this is an observational cross-sectional study, it cannot on its own establish causality, although the findings are consistent with theory, observational data from other settings, and studies using interrupted time-series analysis and related methods. However, it is possible that some of the associations we observed are bidirectional, for example, greater social unacceptability leading to reduced smoking which in turn reduces acceptability further.
Summary
Despite ratification of the FCTC by most countries, there are major policy implementation gaps with a gradient indicating that the chance of quitting is much greater with more comprehensive policy implementation, greater social unacceptability and knowledge of health effects of smoking. This suggests that evidence from HICs on the impact of these aspects of the tobacco control environment on smoking patterns and quitting also apply to LMICs.
supplementary appendix
Acknowledgments
The authors list here the personnel contributing to the PURE and EPOCH studies at all study sites.
Project office (Population Health Research Institute, Hamilton Health Sciences and McMaster University, Hamilton, Canada): S Yusuf* (Principal Investigator).
S Rangarajan (Project Manager); K K Teo, C K Chow, M O'Donnell, A Mente, D Leong, A Smyth, P Joseph, S Islam (Statistician), M Zhang (Statistician), W Hu (Statistician), C Ramasundarahettige (Statistician), G Wong (Statistician), L Dayal, A Casanova, M Dehghan (Nutritionist), G Lewis, J DeJesus, P Mackie, SL Chin, D Hari, L Farago, M Zarate, I Kay, D Agapay, R Solano, S Ramacham, N Kandy, J Rimac, S Trottier, W ElSheikh, M Mustaha, T Tongana, N Aoucheva, J Swallow, E Ramezani, A Aliberti, J Lindeman
Core Laboratories: M McQueen, K Hall, J Keys (Hamilton), X Wang (Beijing, China), J Keneth, A Devanath (Bangalore, India).
Argentina: R Diaz*; A Orlandini, B Linetsky, S Toscanelli, G Casaccia, JM Maini Cuneo; Bangladesh: O Rahman*, R Yusuf, AK Azad, KA Rabbani, HM Cherry, A Mannan, I Hassan, AT Talukdar, RB Tooheen, MU Khan, M Sintaha, T Choudhury, R Haque, S Parvin; Brazil: A Avezum*, GB Oliveira, CS Marcilio, AC Mattos; Canada: K Teo*, S Yusuf*, J Dejesus, D Agapay, T Tongana, R Solano, I Kay, S Trottier, J Rimac, W Elsheikh, L Heldman, E Ramezani, G Dagenais, P Poirier, G Turbide, D Auger, A LeBlanc De Bluts, MC Proulx, M Cayer, N Bonneville, S Lear, D Gasevic, E Corber, V de Jong, I Vukmirovich, A Wielgosz, G Fodor, A Pipe, A Shane; CHILE: F Lanas*, P Seron, S Martinez, A Valdebenito, M Oliveros; CHINA: Li Wei*, Liu Lisheng*, Chen Chunming, Wang Xingyu, Zhao Wenhua, Zhang Hongye, JiaXuan, Hu Bo, Sun Yi, Bo Jian, Zhao Xiuwen, Chang Xiaohong, Chen Tao, Chen Hui, Chang Xiaohong, Deng Qing, Cheng Xiaoru, Deng Qing, He Xinye, Hu Bo, JiaXuan, Li Jian, Li Juan,Liu Xu, Ren Bing, Sun Yi, Wang Wei, Wang Yang, Yang Jun, Zhai Yi, Zhang Hongye, Zhao Xiuwen,Zhu Manlu, Lu Fanghong, Wu Jianfang, Li Yindong, Hou Yan, Zhang Liangqing, Guo Baoxia, Liao Xiaoyang, Zhang Shiying, BianRongwen, TianXiuzhen, Li Dong, Chen Di, Wu Jianguo, Xiao Yize, Liu Tianlu, Zhang Peng, Dong Changlin, Li Ning, Ma Xiaolan, Yang Yuqing, Lei Rensheng, Fu Minfan, He Jing, Liu Yu, Xing Xiaojie, Zhou Qiang; Colombia: P Lopez-Jaramillo*, PA Camacho Lopez, R Garcia, LJA Jurado, D Gómez-Arbeláez, JF Arguello, R Dueñas, S Silva, LP Pradilla, F Ramirez, DI Molina, C Cure-Cure, M Perez, E Hernandez, E Arcos, S Fernandez, C Narvaez, J Paez, A Sotomayor, H Garcia, G Sanchez, T David, A Rico; India: P Mony *, M Vaz*, A V Bharathi, S Swaminathan, K Shankar AV Kurpad, KG Jayachitra, N Kumar, HAL Hospital, V Mohan, M Deepa, K Parthiban, M Anitha, S Hemavathy, T Rahulashankiruthiyayan, D Anitha, K Sridevi, R Gupta, RB Panwar, I Mohan, P Rastogi, S Rastogi, R Bhargava, R Kumar, J S Thakur, B Patro, PVM Lakshmi, R Mahajan, P Chaudary, V Raman Kutty, K Vijayakumar, K Ajayan, G Rajasree, AR Renjini, A Deepu, B Sandhya, S Asha, HS Soumya; Iran: R Kelishadi*, A Bahonar, N Mohammadifard, H Heidari; Malaysia: K Yusoff*, TST Ismail, KK Ng, A Devi, NM Nasir, MM Yasin, M Miskan, EA Rahman, MKM Arsad, F Ariffin, SA Razak, FA Majid, NA Bakar, MY Yacob, N Zainon, R Salleh, MKA Ramli, NA Halim, SR Norlizan, NM Ghazali, MN Arshad, R Razali, S Ali, HR Othman, CWJCW Hafar, A Pit, N Danuri, F Basir, SNA Zahari, H Abdullah, MA Arippin, NA Zakaria, I Noorhassim, MJ Hasni, MT Azmi, MI Zaleha, KY Hazdi, AR Rizam, W Sazman, A Azman; OCCUPIED PALESTINIAN TERRITORY: R Khatib*, U Khammash, A Khatib, R Giacaman; PAKISTAN: R Iqbal*, A Afridi, R Khawaja, A Raza, K Kazmi; PHILIPPINES: A Dans*, HU Co, JT Sanchez, L Pudol, C Zamora-Pudol, LAM Palileo-Villanueva, MR Aquino, C Abaquin, SL Pudol, ML Cabral; Poland: W Zatonski*, A Szuba, K Zatonska, R Ilow#, M Ferus, B Regulska-Ilow, D Różańska, M Wolyniec; SAUDI ARABIA: KF AlHabib*, A Hersi, T Kashour, H Alfaleh, M Alshamiri, HB Altaradi, O Alnobani, A Bafart, N Alkamel, M Ali, M Abdulrahman, R Nouri; South Africa: A Kruger*, H H Voster, A E Schutte, E Wentzel-Viljoen, FC Eloff, H de Ridder, H Moss, J Potgieter, AA Roux, M Watson, G de Wet, A Olckers, JC Jerling, M Pieters, T Hoekstra, T Puoane, E Igumbor, L Tsolekile, D Sanders, P Naidoo, N Steyn, N Peer, B Mayosi, B Rayner, V Lambert, N Levitt, T Kolbe-Alexander, L Ntyintyane, G Hughes, R Swart, J Fourie, M Muzigaba, S Xapa, N Gobile, K Ndayi, B Jwili, K Ndibaza, B Egbujie; Sweden: A Rosengren*, K Bengtsson Boström, U Lindblad, P Langkilde, A Gustavsson, M Andreasson, M Snällman, L Wirdemann, K Pettersson, E Moberg; TANZANIA: K Yeates*, J Sleeth, K Kilonzo; TURKEY: A Oguz*, AAK Akalin, KBT Calik, N Imeryuz, A Temizhan, E Alphan, E Gunes, H Sur, K Karsidag, S Gulec, Y Altuntas; United Arab Emirates: AM Yusufali*, W Almahmeed, H Swidan, EA Darwish, ARA Hashemi, N Al-Khaja, JM Muscat-Baron, SH Ahmed, TM Mamdouh, WM Darwish, MHS Abdelmotagali, SA Omer Awed, GA Movahedi, F Hussain, H Al Shaibani, RIM Gharabou, DF Youssef, AZS Nawati, ZAR Abu Salah, RFE Abdalla, SM Al Shuwaihi, MA Al Omairi, OD Cadigal; R.S. Alejandrino; Zimbabwe: J Chifamba*, L Gwaunza, G Terera, C Mahachi, P Murambiwa, T Machiweni, R Mapanga.
*National Coordinator.
References
Footnotes
Twitter Follow Ehimario Igumbor @Ehimario and Rajeev Gupta @rajeevgg
Contributors CC, DC, ABG, MK and SY contributed to the design and development of the study. CC drafted the paper, DC conducted all analyses, AG and MK contributed to the interpretation of the analyses. All other authors contributed to the data collection and implementation of the protocol. All authors reviewed and contributed to the manuscript draft and its revisions.
Funding The tobacco environment data collection and analyses was supported by a CIHR (Canadian Institute of Health Research) grant application number 184349. CC is supported by a NHMRC Career Development Award APP1033478 cofunded by the Heart Foundation and a Sydney Medical Foundation Chapmen Fellowship and a member of the cardiovascular group at the George Institute supported by a NHMRC programme grant. AG is a member of the UK Centre for Tobacco and Alcohol Studies (UKCTAS), a UK Centre for Public Health Excellence which is supported by the British Heart Foundation, Cancer Research UK, the Economic and Social Research Council, the Medical Research Council and the National Institute of Health Research, under the auspices of the UK Clinical Research Collaboration. EI is supported in part by the National Research Foundation of South Africa (UID: 86003). SY is supported by the Heart and Stroke Foundation Mary Burke Chair for CV research. The funders played no role in the study design, analysis and interpretation of data, nor writing of the report or the decision to submit the article for publication. The content is solely the responsibility of the authors and does not necessarily represent the views of the funders.
We have listed in a separate appendix the details of funding for the parent study PURE.
Competing interests None declared.
Ethics approval The EPOCH study and data collection instruments were approved by the Hamilton Health Sciences/McMaster Health Sciences Research Ethics board and by corresponding ethics boards in each country
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data for this study and related studies from the PURE and EPOCH studies are stored at the Population Health Research Institute (PHRI), McMaster University. Requests for PURE and EPOCH data is assessed by the study steering committee and applications can be made to the study project manager, Sumathy Rangarajan sumathy.rangarajan@phri.ca.