Article Text

Abstract
Objectives Single-visit root canal treatment has some advantages over conventional multivisit treatment, but might increase the risk of complications. We systematically evaluated the risk of complications after single-visit or multiple-visit root canal treatment using meta-analysis and trial-sequential analysis.
Data Controlled trials comparing single-visit versus multiple-visit root canal treatment of permanent teeth were included. Trials needed to assess the risk of long-term complications (pain, infection, new/persisting/increasing periapical lesions ≥1 year after treatment), short-term pain or flare-up (acute exacerbation of initiation or continuation of root canal treatment).
Sources Electronic databases (PubMed, EMBASE, Cochrane Central) were screened, random-effects meta-analyses performed and trial-sequential analysis used to control for risk of random errors. Evidence was graded according to GRADE.
Study selection 29 trials (4341 patients) were included, all but 6 showing high risk of bias. Based on 10 trials (1257 teeth), risk of complications was not significantly different in single-visit versus multiple-visit treatment (risk ratio (RR) 1.00 (95% CI 0.75 to 1.35); weak evidence). Based on 20 studies (3008 teeth), risk of pain did not significantly differ between treatments (RR 0.99 (95% CI 0.76 to 1.30); moderate evidence). Risk of flare-up was recorded by 8 studies (1110 teeth) and was significantly higher after single-visit versus multiple-visit treatment (RR 2.13 (95% CI 1.16 to 3.89); very weak evidence). Trial-sequential analysis revealed that firm evidence for benefit, harm or futility was not reached for any of the outcomes.
Conclusions There is insufficient evidence to rule out whether important differences between both strategies exist.
Clinical significance Dentists can provide root canal treatment in 1 or multiple visits. Given the possibly increased risk of flare-ups, multiple-visit treatment might be preferred for certain teeth (eg, those with periapical lesions).
- Clinical outcomes
- Clinical studies/trials
- Comparative effectiveness research (CER)
- Endodontics
- Evidence-based dentistry/health care
- Systematic reviews and evidence-based medicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Clinical outcomes
- Clinical studies/trials
- Comparative effectiveness research (CER)
- Endodontics
- Evidence-based dentistry/health care
- Systematic reviews and evidence-based medicine
Strength and limitations of this study
This registered systematic review applies meta-analysis and trial-sequential analysis to assess the strength and quantity of the accrued evidence towards different root canal treatment strategies.
The synthesised estimates are supported only by moderate or weak evidence according to GRADE.
Firm evidence for benefit or harm of single-visit or multiple-visit root canal therapy as well as futility of further trials was not reached.
Introduction
After root canal treatment, teeth can experience short-term and/or long-term complications. Short-term complications include postoperative inflammation of periapical tissues leading to mild pain or flare-up (ie, an acute exacerbation of pulpal or periapical pathosis after root canal treatment, like severe unbearable pain and swelling). Pain and swelling have been associated with instrumentation or irrigation transporting medications, infected debris and bacteria into the periapical tissues. Inadequate instrumentation and disinfection lead to bacterial persistence within the root canals and consequent (re)contamination of periapical tissue.1 ,2 Long-term outcomes include persisting inflammation and infection, resulting in abscess, sinus track formation, radiographical signs of periapical bone resorption or severe pain, with subsequent need to endodontically re-treat or remove teeth.3 ,4 Both short-term and long-term outcomes seem to be affected by the preoperative condition of the tooth (tooth type, vitality, symptoms, periapical conditions).4 Moreover, they might be affected by how root canal treatments are provided.
Single-visit root canal treatment attempts instrumentation, disinfection and obturation of the root canal system in one visit. In contrast, multiple-visit root canal treatment performs the instrumentation (or large parts of it) in the first and the obturation in the second visit, while the disinfection is provided in both visits via irrigation. Moreover, a disinfecting medication is placed in the canals between visits to allow further reduction of bacterial numbers. While single-visit treatment has obvious advantages over conventional multiple-visit treatment (like reduced number of visits, no need for repeated application of anaesthetics or rubberdam, no intermediary restoration); it might be disadvantageous both with regard to short-term and long-term outcomes.
A number of reviews have compared single-visit versus multiple-visit root canal treatment.3 ,5–8 Some of these are outdated,3 ,6 others investigate only short-term pain as outcome,5 again others build on evidence beyond controlled trials like cohort studies or expert opinions,7 or pooled short-term and long-term outcomes, which does not allow to weigh them against each other.8 The present review aimed to comprehensively compare the currently available controlled trial data on short-term and long-term complications of single-visit versus multiple-visit root canal treatment. Our primary objective was to answer the question: In patients needing root canal treatment, is single-visit treatment significantly more effective than multiple-visit treatment with regard to risk of long-term failure? The secondary objective was to compare both treatments with regard to risk of short-term postoperative pain as well as the risk of flare-up. We further investigated moderators of risks using subgroup or meta-regression analysis, and assessed how statistically robust current evidence is with regard to type I or II errors using trial sequential analysis (TSA). The review should guide the conduct of further studies and help to deduct clinical recommendations.
Methods
Eligibility criteria
This systematic review (registered at PROSPERO CRD42016036386) included trials that:
Were randomised controlled trials or controlled trials without signs of selection bias (ie, treatments were not allocated according to preoperative tooth status, etc). Sensitivity analyses were performed to account for the introduced risk of bias in case of treatment allocation not being at random.
Compared single-visit with multiple-visit root canal treatment in permanent teeth with closed apices and without internal resorption, regardless of the preoperative condition (meta-regression and subgroup analyses were performed to account for different conditions).
Reported on risk of long-term complications (≥1 year after treatment), and/or risk of experiencing any short-term pain, and/or risk of short-term flare-up.
Outcomes
The primary outcome was the risk of long-term complications, defined as pain, infection/swelling/sinus track formation, or development, persistence or aggravation of periapical lesions or widening of the periodontal ligament, etc, ≥1 year after treatment. No standard as to how periapical lesions needed to be assessed or categorised was set, as a range of classification systems are currently used.3 Note that against our protocol, we did not assess the need of retreatment due to long-term complications, as in most included trials it was not clearly stated, if retreatments have been performed.
The secondary outcomes were:
Risks of experiencing any short-term pain (<1 year after treatment) after obturation or after instrumentation or after both. For comparison of treatments, we considered only pain after obturation, not after instrumentation without obturation during multiple-visit treatment. To detect the largest difference between treatments, incidence of pain was extracted at the shortest recording time point after treatment. As we did not separate mild, moderate or severe pain, and even included outcome measures like having taken any pain medication in this outcome, risk of any pain does not necessarily indicate a further treatment being required. Moreover, it should be noted that different degrees of pain were pooled. This was not avoidable given the different scales used, which cannot be synthesised otherwise, but introduces additional heterogeneity.
Risks of experiencing short-term flare-up, usually defined as an acute exacerbation of an asymptomatic pulpal and/or periradicular pathosis after the initiation or continuation of root canal treatment.9 Note that flare-up was not defined consistently across studies; some studies reported flare-up while having treated both symptomatic and asymptomatic teeth. We therefore defined flare-up as a short-term symptom (<1 year, usually directly after initiation or conclusion of root canal treatment) which led or can be assumed to lead to a further intervention (like reaccessing/reinstrumenting an incomplete treatment; completing an incision and drainage procedure, or reperforming root canal treatment).
Searches
We searched MEDLINE via PubMed, EMBASE via Ovid and Cochrane Central on 10 March 2016. Moreover, opengrey.eu was searched to identify accepted, but not published studies. There was no date restriction in our search. In addition, reference lists of identified full-texts were screened and cross-referenced. We contacted study authors if required to obtain full texts. Neither the authors nor journals were blinded to reviewers. No language restriction was set.
The applied search strategy can be found in figure 1.

Study flow. Database screening was performed using a four-pronged search strategy, combining four domains of the search using Boolean operators. Number of studies yielded in MEDLINE by each search domain are shown in the upper boxes; combining these boxes led to the number of results as shown for each database.
Study records
Data management
A piloted spreadsheet was used for data extraction and management.
Selection process
Two reviewers (FS and GG) independently screened titles and then compared their findings. In case of disagreement, titles were included to obtain full texts. Full texts were assessed independently after de-duplication. Studies were included after agreement with consensus in cases of disagreement being reached through discussion.
Data collection process
Data extraction was performed independently by two reviewers (FS and GG). Disagreements were resolved through discussion.
Data items
The following items were collected: author names, year, sample, setting, tooth type, pulp vitality, preoperative pain, presence of radiographically detectable periapical lesions, instrumentation type, obturation type, irrigation, medication, intermediate restoration, number of visits, evaluation method, findings.
Outcomes
Outcomes and outcome measures were extracted. For studies reporting non-significant findings without any further information, this was extracted to allow including these into a sensitivity meta-analysis (see below).
Data synthesis
Meta-analysis
The statistical unit was the tooth. Clustering was near absent in most studies. Therefore, the risk of this approach leading to artificially narrow CIs is low.10 A continuity correction of +1 was performed in case of zero events. Random-effects meta-analysis using the DerSimonian-Laird estimator of variance was performed using Comprehensive Meta-Analysis V.2.2.64 (Biostat, Englewood, New Jersey, USA), with risk ratios (RRs) and 95% CIs as effect estimates. Fixed-effect models were used as well, but did not yield significantly different findings given the low level of heterogeneity. Unit of analysis issues were handled as described in the online supplementary appendix. Heterogeneity was assessed using Cochran's Q and I2 statistics.11 Funnel plot analysis and Egger test were performed to assess small study effects or publication bias.12 ,13 RR were adjusted to check the impact of possible publication bias.14
Supplemental material
Subgroup and meta-regression analyses
Subgroup and meta-regression analyses were carried out to assess (1) the impact of a root canal medication being used (or not) in multiple-visit treatment, (2) pulp vitality prior treatment, (3) preoperative pain and (4) the presence of radiographically detectable periapical lesions on effect estimates. Details can be found in the online supplementary appendix.
Confidence in data
Risk of bias was assessed and classified according to Cochrane guidelines.13 Note that against our protocol, we did not assess performance bias (blinding of operators), as this is not feasible in trials comparing single-visit versus multiple-visit treatment.
In addition, TSA was performed to assess if quantitative findings are robust, and to calculate the required information size (RIS), that is, the cumulative sample size needed to yield significant differences between treatments.15 ,16 RIS is then adjusted for heterogeneity/diversity (DARIS). TSA additionally estimates trial sequential monitoring boundaries (TSMBs), that is, statistical thresholds for significance which are adapted depending on the so far reached sample size. Firm evidence is assumed to be reached when the Z-curve crosses the TSMB for either benefit or harm before the DARIS was reached. Effect estimates supported by only few small trials are handled stricter than those supported by large samples. In addition to such superiority/inferiority TSMBs, monitoring boundaries for futility were calculated. These indicate if further trial conduct is likely to be futile, that is, if sufficient evidence has been accrued to claim non-inferiority of treatments (which would be most relevant for this review). Further details have been reported elsewhere,17 and can also be found in the online supplementary appendix.
Evidence for each outcome effect estimate was graded according to the GRADE working group of evidence,18 using Grade Profiler V.3.6, and strength of recommendations deduced accordingly.19
Results
Results of the searches
From 817 records, 64 were screened full text. After cross-referencing 67 articles were screened and 29 included (figure 1).8 ,20–48 Excluded studies and reasons for exclusion can be found in the online supplementary appendix table S1.
Overall, 4341 (mainly adult) patients had been treated (table 1).
Included studies
Six trials treated only teeth with vital pulps, six treated vital and non-vital teeth or did not specify vitality; the remaining trials treated non-vital teeth. Three trials clearly stated to treat only teeth with preoperative pain, 20 treated both painful and painless teeth or did not state any details on preoperative symptoms, and the remaining trials treated only teeth without preoperative symptoms. Ten trials included only teeth with periapical lesions, 13 trials did not report on radiographical status of the periapex or treated both teeth with and without lesions; the remaining trials treated only teeth without any detectable lesions.
Six trials were found to have low risk of bias (see online supplementary table S2), the remaining trials showed high or unclear overall risk of bias. This was mainly due to a lack of examiner blinding or allocation concealment. Two trials did not at all report on randomisation, and were treated accordingly in the performed meta-analysis. The majority of trials mentioned randomisation, but did not state how sequences were generated. Attrition was generally limited (as most trials did only assess short-term pain, see below), as was risk of selective reporting.
Risk of long-term complications
Long-term complications were investigated by 10 trials, with a total of 1257 teeth being treated. Mean follow-up was 2.3 years (range 1–5 years). All trials had used calcium hydroxide as medication in the multiple-visit group. All but two trials had high risk of bias. Risk of complications was not significantly different in single-visit versus multiple-visit treatment (RR 1.00 (95% CI 0.75 to 1.35)). Heterogeneity was low. Publication bias was not detected via Egger's test (p=0.36) or funnel plot analysis (figure 2A, online supplementary appendix figure S1A).

Risk of long-term complications after single-visit versus multiple-visit root canal treatment. (A) Forest plot, with RR and 95% CIs per study and overall (black diamond) being given. Heterogeneity across studies is indicated by I² and Q. Low risk of bias and lack of random allocation of treatment is indicated by asterisks and hashtag. (B) Trial sequential analysis. The cumulative Z-score (black), that is, the accumulated level of significance, was plotted against the number of participants (N) accrued, which was compared with the DARIS. The Z-curve does not cross the conventional thresholds for superiority or inferiority (hatched grey lines). Neither the DARIS nor TSMB (grey solid lines) were reached. The information fraction was too small to draw trial sequential futility boundaries. DARIS, diversity-adjusted required information size; RR, risk ratio; TSMB, trial sequential monitoring boundary.
Preoperative conditions were not found to significantly impact on effect estimates (table 2).
Meta-regression analysis
Studies which did not state to have randomly allocated treatments did not find significantly different RRs (p=0.35). By using TSA, we found neither the conventional thresholds for benefit or harm nor the TSMB for benefit, harm or futility to be reached. The sample size was far below DARIS (figure 2B). Given that risk of bias was serious and the number of events low (leading to imprecision), our confidence in this finding was weak.
Risk of experiencing any postoperative pain
Twenty studies used binary estimates to express risk of short-term pain. Of these, three had used a factorial design, with resulting subgroups being handled as independent studies. Three further studies used visual analogue scales and reported pain to not be significantly different; these were included in a sensitivity analyses. For the base-case analysis, a total of 3008 teeth were available and assessed. Pain had been recorded after a mean of 2 days (range 1–7 days) postoperatively. Three trials had compared pain only after instrumentation; the other studies compared pain after obturation. All but three trials showed high risk of bias.
Risk of pain was not significantly different in single-visit versus multiple-visit treatment (RR 0.99 (95% CI 0.76 to 1.30)). Heterogeneity was moderate. There was no indication for publication bias via Egger's test (p=0.46) or funnel plot analysis (figure 3A, online supplementary appendix figure S1B). Preoperative conditions or the use of a calcium hydroxide instead of no root canal medication between visits had no significant impact on effect estimates (table 2). Studies which did not state to have randomly allocated treatments did not find significantly different RRs compared with studies which had clearly stated randomisation (p=0.46). Including imputed studies which had only reported that differences between groups were non-significant (but had not given an effect estimate) increased the total number of assessed teeth to 3417, but did not significantly change our estimates (RR=1.00 (0.86 to 1.21)). Excluding those trials which only reported on pain after instrumentation, not obturation, also had no significant impact (RR=0.99 (0.84 to 1.17)). Using TSA, we found the conventional thresholds for benefit to be spuriously crossed, while the TSMB for benefit was not reached. Futility boundaries were not constructible due to too few data being available. The sample size was far below DARIS (figure 3B). Given the serious risk of bias, but only limited evidence for imprecision, this finding is supported by moderate evidence according to GRADE.

Risk of experiencing any postoperative pain after single-visit versus multiple-visit root canal treatment. (A) Forest plot. Low risk of bias and lack of random allocation of treatment is indicated by asterisks and hashtag. Studies which compared treatments in different subgroup of teeth were handled as independent studies and are indicated accordingly. (B) Trial sequential analysis. The information fraction was too small to draw trial sequential futility boundaries. DARIS, diversity-adjusted required information size; TSMB, trial sequential monitoring boundary.
Risk of flare-up
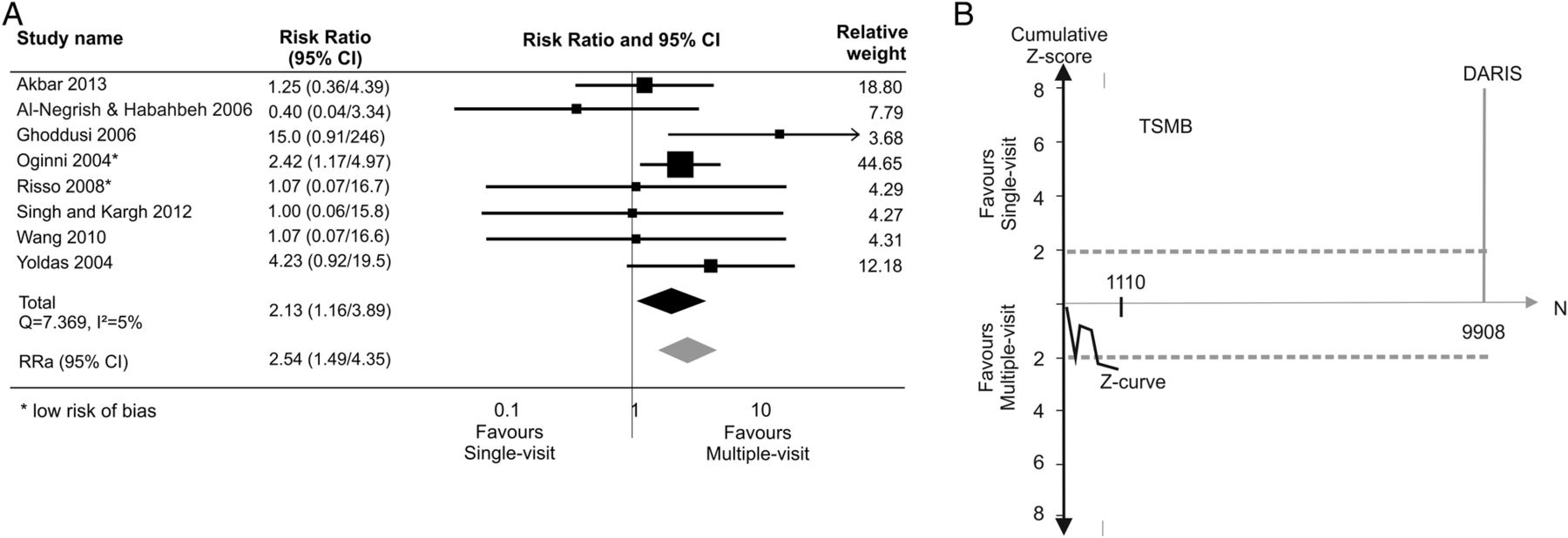
Risk of flare-up was recorded by eight studies. A total of 1110 teeth had been followed over a period of 7–10 days. All studies stated to be randomised trials, two studies showed low, the rest high risk of bias.
Risk of flare-up was significantly higher after single-visit versus multiple-visit treatment (RR 2.13 (95% CI 1.16 to 3.89)). Heterogeneity was low. There was some indication for publication bias based on funnel plot analysis, but not Egger's test (p=0.26). Adjusting the estimate accordingly increased the RR (figure 4A, online supplementary appendix figure S1C). Preoperative conditions and the root canal medication had no significant impact on effect estimates (table 2). Using TSA, we found the conventional thresholds for harm to be spuriously crossed, while the TSMB for harm was not reached. Futility boundaries were not constructible due to too few data being available. The sample size was far below DARIS (figure 4B). Given the serious risk of bias, imprecision and publication bias being present, our confidence in this finding is supported by only very weak evidence according to GRADE.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk of experiencing flare-up after single-visit versus multiple-visit root canal treatment. (A) Forest plot. RR and 95% CI were adjusted for publication bias using trim-and-fill (RRa). Low risk of bias and lack of random allocation of treatment is indicated by asterisks and hashtag. Studies which compared treatments in different subgroup of teeth were handled as independent studies and are indicated accordingly. (B) Trial sequential analysis. The information fraction was too small to draw trial sequential futility boundaries. DARIS, diversity-adjusted required information size; RR, risk ratio; RRa, adjusted risk ratio; TSMB, trial sequential monitoring boundary.
Discussion
Even after optimal root canal disinfection via instrumentation and irrigation, bacteria usually remain within the root canal system.49 ,50 During multiple-visit root canal treatment, an antibacterial medication like calcium hydroxide is placed in the root canals, thereby aiming to further disinfect the canals between treatment appointments, the efficacy of which remains unclear at present.49 ,51–53 In contrast, in single-visit root canal treatment any further appointments and intracanal medications are omitted, and the root canal system obturated directly after instrumentation and irrigation, aiming to seal remaining bacteria and deprive them from both space and nutrition.3 ,46 ,54 ,55
For risk of long-term complications, we did not find a difference between single-visit and multiple-visit endodontic treatment. This was our primary outcome as such complications oftentimes decide the fate of the tooth.56–58 It is noteworthy that this was supported by a range of studies (ie, studies with high or low risk, small or large samples, in adults or adolescents, vital or non-vital teeth, teeth with or without periapical lesions) with relatively homogeneous findings. Only one trial found significant differences between groups (favouring single-visit treatment),35 all others did not find one treatment significantly superior over the other.
Based on our analyses, the discussed confounders do not seem to significantly affect the relative risk of complications. Even in teeth with periapical lesions, single-visit treatment showed no significantly different risk of complications. This finding is in line with that from a previous review.6 We want to highlight that our performed meta-regression and subgroup analyses are potentially underpowered, with high risk of type II errors. In general, our findings on the risk of complications outcome are supported by limited data, as indicated by TSA. Based on this analysis, no firm evidence on benefit, harm or futility is available (while the cumulative Z-curve never crossed any threshold for significance, once more confirming a trend towards non-difference of treatments).
The resulting evidence was graded as weak, mainly due to risk of bias of trials. Thus, a number of recommendations towards future studies need to be made: First, future trials should have higher internal validity, for example, by performing and reporting on sequence generation, by sufficiently concealing the allocation, and by blinding assessors, all to reduce the risk of selection and detection bias. We are well aware that blinding operators or patients is impossible in such trials; future reviews should reflect on this when assessing risk of bias (as we did accordingly). Second, trials should be performed in realistic (primary care) settings with sufficiently long follow-up periods, as complications are expected to occur long term. Third, trials should aim to investigate the relevance of preoperative conditions as possible confounders, as current data are insufficient to conclude on the suitability of single-visit versus multiple-visit treatment in different teeth or patients.
We also found single-visit treatment to not significantly increase the risk of short-term postoperative pain, which is in line with findings from previous reviews.3 ,6 ,59 Pain is a relevant outcome, despite being reported only for brief periods after treatment and not being a strong predictor for success,50 as it is directly burdening patients and could influence their attitude and behaviour towards future endodontic treatment. Our findings were again relatively consistent between trials regardless of their risk of bias, setting, patients or treated teeth. Only three studies found significant differences between groups; two in favour of single-visit treatment,21 ,27 and one in favour of multiple-visit treatment.30 All three were performed in non-vital teeth. It is again important to note that while we did not identify significant confounders (which is in line with previous findings),60 our meta-regression analyses are (as discussed) of limited power. However, the overall number of treated teeth was relatively high, and while current data were4 insufficient to establish firm evidence, we expect futility boundaries of TSA to be reached if future trials confirm these findings. Given the discussed uncertainties associated with the preoperative condition (vitality, symptoms), researchers should account for these confounders when designing and evaluating future trials in the field.
We found single-visit treatment to significantly increase the risk of flare-up, which is in agreement with a previously identified increased risk of swelling after single-visit treatment.3 It should be highlighted that our analysis for this outcome was built on only few, mainly high-risk trials, and that one particular study contributed a lot to the effect estimate given its weighting.34 This weighting was the result of the high incidence of flare-up in this study (20% in the single-visit group), which is much higher than that in all other trials. Excluding this study from the analysis decreased the effect estimates, with no significant difference between groups remaining (RR 1.85 (0.89 to 3.86)). Given that TSA indicated that no firm evidence has been reached so far, caution is thus required when interpreting our finding regarding flare-up. Such caution is further justified as flare-ups, occurring directly after treatment as well as up to 7 days after instrumentation (or obturation), were pooled. Moreover, risk of flare-ups might be affected by further factors like patients' age, gender or systemic conditions. While patients with systemic conditions were excluded in all studies, insufficient information was available regarding gender and age distribution. Future studies should report in more detail on these aspects.
This review has a number of limitations. First, it builds only on randomised or at least controlled trials. While we see the value of practice-based long-term cohort studies (which have higher external validity and yield findings in a more relevant timeframe), we actively restricted our review on controlled studies to minimise the risk of selection bias, the impact of which can be expected to be potentially severe given that treatment decisions might be made based on the preoperative condition of the tooth. For example, dentists might be more willing to perform single-visit treatment in vital teeth, or molars might be treated in multiple visits more often due to practical reasons. This would greatly distort the true relative efficacy of both therapies.
Second, our primary outcome, complications, is a composite of different components like long-term pain, clinical signs of inflammation and infection (swelling, sinus track formation), and radiographic success (which does not need the patient to experience symptoms). For each component, a decision to re-treat or not might differ depending on who is deciding: dentists (and researchers specialising in endodontics) might see a persistent periapical lesion as an indication to re-treat even in the absence of symptoms (anticipating such symptoms to occur at some stage in the future, with poorer prognosis for retreatments). In contrast, patients might not be willing to re-treat such tooth (which might as well be justified when considering the success rates of the available retreatments and the resulting treatment costs).58
Third, one of our secondary outcomes, the risk of experiencing any postoperative pain, does not account for the degree of pain, losing a significant amount of information. That was done as most trials reported pain using either binary scales (pain yes/no) or ordinal scales, which did not always use identical categories and pose great difficulties when pooling them (or require the definition of a certain pain threshold, which is usually arbitrary). Future studies should use continuous outcome measures like visual analogue scales, allowing to fully display the recorded information on pain. It is noteworthy that those studies which used such scales also found no significant difference of pain levels between treatments.
Last, most included trials reported only on very limited periods after treatment. While this might be acceptable for short-term pain, a follow-up of mean 2.3 years is insufficient to truly reflect ‘long-term’ complications (as is applied definition of minimum 1 year follow-up to consider a complication as long-term). This is closely related with the discussed limitations of randomised trials, which are seldom able to follow-up teeth for much longer given the high associated efforts and costs.
Future trials are thus needed to gain firm evidence whether differences in outcomes between single-visit or multiple-visit root canal treatment exist. To improve validity and comparability, these trials should aim for standardised outcome measures (eg, visual analogue scale for pain assessment; agreed definition for success/failure), long-term follow-up periods and limited risk of bias (while certain bias cannot be fully excluded). They should best be performed in representative settings and populations and report in detail on confounders of treatment success.
In conclusion and within the limitations of this review, there is insufficient evidence to rule out whether important differences in outcomes between single-visit or multiple-visit root canal treatment exist. Given the possibly increased risk of flare-up, a careful recommendation could be to prefer multiple-visit treatment in teeth where the risk if complication is increased (eg, teeth with existing periapical lesions).
References
Footnotes
Contributors FS contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; GG contributed to conception, design, data acquisition, interpretation and critically revised the manuscript.
Funding This study was funded by the authors and their institution.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.