Article Text

Abstract
Objectives Recent evidence from the 7-year follow-up of the Pediatric Osteoporosis Prevention (POP) study indicates an inverse correlation between years of participation in a physical activity (PA) intervention and fracture risk in children. However, we could not see a statistically significant reduction in fracture risk, which urged for an extension of the intervention.
Setting The study was conducted in 4 neighbouring elementary schools, where 1 school functioned as intervention school.
Participants We included all children who began first grade in these 4 schools between 1998 and 2012. This resulted in 1339 children in the intervention group and 2195 children in the control group, all aged 6–8 years at the state of the study.
Intervention We launched an 8-year intervention programme with 40 min of moderate PA per school day, while the controls continued with the Swedish national standard of 60 min of PA per week.
Primary outcome measure We used the regional radiographic archive to register objectively verified fractures and we estimated annual fracture incidences and incidence rate ratios (IRRs).
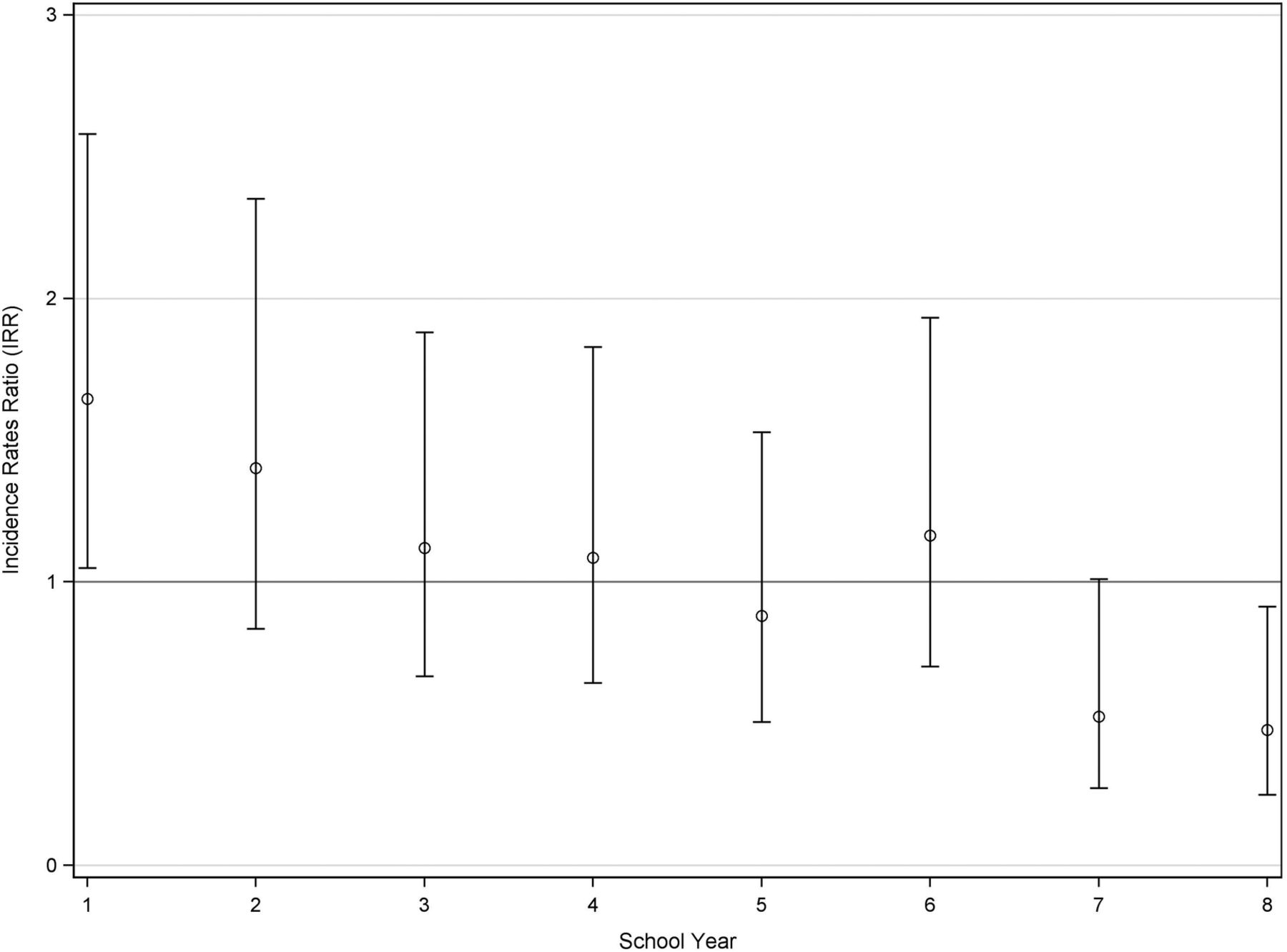
Results During the first year after initiation of the intervention, the fracture IRR was 1.65 (1.05 to 2.08) (mean 95% CI). For each year of the study, the fracture incidence rate in the control group compared with the intervention group increased by 15.7% (5.6% to 26.8%) (mean 95% CI). After 8 years, the IRR of fractures was 52% lower in the intervention group than in the control group (IRR 0.48 (0.25 to 0.91) (mean 95% CI))].
Conclusions Introduction of the school-based intervention programme is associated with a higher fracture risk in the intervention group during the first year followed by a gradual reduction, so that during the eighth year, the fracture risk was lower in the intervention group.
Trial registration number NCT00633828.
- SPORTS MEDICINE
- PUBLIC HEALTH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The study was conducted as a longitudinal population-based case–control study.
The long follow-up period and large sample size facilitated estimation of annual fracture risk.
There was a lack of registration of where and when fractures were sustained and how many fractures were sustained during the school physical activity.
There were no background data available among participants.
There was a notable discrepancy between the numbers of participants in the intervention group compared with the control group.
Introduction
Prospective controlled studies have shown that physical activity (PA) intervention programmes in children improve bone mass and muscle strength,1–4 traits known to affect fracture risk.5–7 Other studies have found that induced skeletal benefits in adolescence and young adulthood are positively correlated with low fracture risk later in adulthood.8–11 There are no studies however that has shown that PA-induced gains in musculoskeletal function in childhood result in lower fracture risk. Instead, increased PA in childhood has actually been found to initially increase the fracture risk,3 ,12 possibly because any beneficial gains in bone mass and muscle function are only reached after some time of participation in PA. This initial risk increment may obscure a progressive fracture-risk reduction if the fracture risk only is reported aggregated for the entire period.13 ,14 There is thus a need for a long-term intervention study with year-by-year evaluation of fracture risk.
In the Pediatric Osteoporosis Prevention (POP) study, a prospective controlled PA intervention study, we have previously reported that the annual incidence rate ratio (IRR) of fractures declined with each year of additional PA, but we could not show that the intervention resulted in a lower fracture risk.3 To be able to conclude whether or not this happens, there is a need for an extension of the study. We conducted such an extension with the hypothesis that our long-term PA intervention programme would initially lead to a higher fracture risk before musculoskeletal benefits evolve, but after 8 years, the intervention would result in a lower fracture risk.
Methods
The Malmo POP study is a prospective controlled intervention study that evaluates the effects of school-based PA on different medical aspects in growing children.15 ,16 The study was approved by the Ethics Committee of Lund University, Sweden (LU 453-98; 1998-09-15) and was conducted according to the Declaration of Helsinki. This clinical trial is registered with registration identification ClinicalTrials.gov NCT00633828.
We have previously described the study protocol in detail,13 ,15 but to summarise we asked four elementary schools to participate in the study. The schools were community-based, government-funded, used the compulsory standard national curriculum and were located within the same city region. The children were assigned to their school according to their residential address. One school served as intervention school, while the three others were control schools. The intervention school increased the amount of physical education (PE) from 60 min/week to 40 min/school day (200 min/week).15 The control schools continued with 60 min/week, given in one to two lessons, the standard duration of PE in our national school curriculum. There were no extra PE classes during weekends or holidays (15 weeks/year). The PE was supervised by the regular schoolteachers and consisted of ordinary PE activities within the national educational plan such as running, jumping, climbing, swimming and various ball games. Thus, the PE was not specifically designed to reduce fractures. The intervention was conducted within the resources of the schools. The intervention proceeded for 8 years, and since PE is a compulsory subject in Sweden, all children had to participate.
We included all children (3534) who began first grade (6–8 years old) between 1998 and 2012, 1339 children (46.2% girls and 53.8% boys) in the intervention and 2195 children (48.7% girls and 51.3% boys) in the control group. We followed the children that started school between 1998 and 2005 for 8 years and those who started school in 2006 and later until 2013. Consequently, the children were followed from 1 to 8 years depending on which year they began first grade. The number of participants having completed a year of intervention is thus lower by each successive school year (table 1). Children who moved out of the region or changed school between intervention and control schools (n=183) were followed until the date either of these things occurred.
Number of fractures, fracture incidences, and incidence rate ratios (IRR) per school year during the 8-year study period
We registered objectively verified incident fractures through repeated evaluations of the regional computerised radiographic database that has records of all radiographs within the region. Fractures occurring outside the region were registered at follow-up exams at our hospital. This method has previously been used and evaluated extensively at our research centre.17 Since we used the radiographic archive to register fractures, we could evaluate 100% of the participating children, that is, there were no dropouts. Trauma mechanism, determined by reading the referrals, was regarded as high-energy, moderate-energy or low-energy using the Landin classification.18
We used IBM SPSS Statistics V.20 for statistical analyses. Data are presented as absolute numbers and means with 95% CIs. We estimated annual fracture incidences and calculated IRRs by dividing the incidence in the intervention group with the incidence in the control group. We used Spearman's test for correlation between number of years of intervention and the IRR for each year. We also used a generalised estimating equations (GEE) model based on negative binomial distribution with exchangeable working correlations to estimate the difference in fracture incidence rates during the overall study period. Finally, as there was an outlier in fracture incidence in the intervention group during the sixth school year, we conducted the same analysis using a dummy variable for this outlier for comparison.
Results
During the study period, we found 506 fractures among the 3534 children. The annual fracture incidences per group are shown in table 1. Gender and school-specific analyses are shown as online supplementary appendices 1–4. Types of fractures and trauma mechanisms are shown in table 2. We found an inverse correlation between the annual IRR for sustaining a fracture and the number of years of intervention (r=−0.86; p=0.007) (figure 1). The IRR for sustaining a fracture during the first year was 1.65 (95% CI 1.05 to 2.58), during the seventh year 0.52 (95% CI 0.27 to 1.01) and during the eighth year 0.48 (95% CI 0.25 to 0.91) (table 1). The overall IRR during the 8-year study period was 1.00 (95% CI 0.88 to 1.13). Using the GEE model, we estimated that after initiation of the study, the fracture incidence rate in the control group was 54.0% (95% CI (35.7% to 81.5%)) of the fracture incidence rate in the intervention group. Furthermore, during the study period, the fracture incidence rate for the control group compared with the intervention group increased each year of the study by 15.2% (95% CI (5.0% to 26.4%)). Using a dummy variable in the analysis resulted in a 0.2 percentage point difference in the estimation (15.4% (95% CI (5.2% to 26.6%))).
Supplemental material
Fracture types and trauma mechanisms by group for the 506 registered fractures. Data presented as absolute values with percentages within parentheses.

{kind=link}
Annual fracture incidence rate ratios (IRRs) throughout the study for the intervention group compared with the control group. Data presented with 95% CIs.
The number of fractures, fracture incidences and IRRs per school year during the 8-year study period was calculated. Data are presented as numbers, person-years, mean fracture rates and risk ratios with 95% CIs. Statistically significant group differences are in bold.
Discussion
We have previously reported an inverse correlation between number of years of PA intervention and fracture risk after a temporary increase in fracture risk when introducing the PA intervention,3 but we can now also state that the annual fracture risk is 52% lower during the eighth year of intervention. Since about 30% of all children sustain at least one fracture during childhood,19 our findings have clinical importance for individual suffering, and for costs and the burden of healthcare on society.
There was no difference in overall fracture risk during the study period between the intervention group and control group. However, as previously reported,3 year-by-year fracture risk evaluation revealed an initial transient increase in fracture risk in the intervention group followed by a gradual fracture risk reduction leading to a significantly lower fracture risk at the end of the intervention period. The lower IRR in the current study seems mainly explained by the fact that the intervention group did not experience the normal increasing fracture incidence during puberty,19 an increase found in the control cohort. A potential explanation for this finding is that before any positive effects of the PA has had time to develop, the increased PA possibly results in more trauma exposure and thereby fractures. As the intervention then continuous, it could result in positive fracture preventive effects such as increased bone mass, muscle strength and neuromuscular function that lead to a progressive reduction in fracture risk. During the sixth year of the study, the fracture incidence in the intervention group seemed to increase compared with previous and following years. We have found no explanation for this finding and it may most likely be a result of chance, but we cannot exclude factors such as maturation, growth and lifestyle changes have influenced the results.
There are several possible mechanisms for PA to modulate fracture risk. In a 7-year POP study report,3 we found that in a subcohort of children that received the intervention, the PA was accompanied by greater gains in muscle strength and areal bone mineral density (aBMD). In adults, improved muscle strength has been found to reduce fall frequency20 and higher aBMD to reduce fracture risk,21 which might indicate that this is true also for children. Furthermore, fall frequency may in children also be reduced due to better neuromuscular function and coordination. This may then lead to fewer falls, and also to less injurious falls due to improved body control and faster protective movements.22 Consequently, it seems that PA may induce beneficial effects in several traits that all could decrease the fracture risk.
Our findings imply that increased PA in the school curriculum could be used as a population-based fracture-protective tool in adolescence, but that the duration of the increased PA must be long term to achieve benefits. Exactly how long time of PA that is needed to receive lower fracture risk is not determined, but we could in our study only find effects after 8 years of intervention. Other studies have shown that fracture incidence is low in former athletes8–11 and that PA-induced skeletal benefits are partly retained long term after reduced activity level.9 ,23 ,24 We therefore speculate that our school-based intervention programme could result in lower fracture risk in adulthood and old age, but future prospective studies are needed to verify or reject this hypothesis.
Furthermore, as described in the Methods section, the PA intervention consisted of regular physical activities not specifically designed to reduce fractures. An intervention with more high-impact activities, which strengthen bone and muscle, may result in an even lower fracture risk, but could also result in higher exposure to trauma and thereby a higher fracture risk. Also, there is a risk that repeated activities make the children bored and thereby reduce their intensity levels during the PE. Greater effects may also have been possible if the PA was changed during the course of the programme. Overall, the optimal programme would include all children, prevent fractures throughout the study and not result in a higher fracture risk after initiation. To find out which activities at what extent have the best fracture protective effects, further studies are needed.
Study strengths include the longitudinal population-based case–control design, a large sample size, no dropouts, inclusion of only objectively verified fractures, the long follow-up period facilitating estimation of annual fracture risk and the use of the clinically relevant end point fractures. Study limitations include the lack of registration of where and when the fractures were sustained and how many fractures were sustained during the school PA. Also, it would have been preferable to have background data on the participants such as height, weight, maturation status, previous fracture history, PA levels outside school and dietary intake to evaluate potential confounding factors. A major limitation is also that this is not strictly a randomised controlled trial, a study design the schools refused to participate in due to practical reasons. Furthermore, we must emphasise that our conclusions are based on comparisons with a group of children receiving 60 min of PE per school day and with a fairly generous amount of spare time PA. Thus, we cannot state whether or not the same effects will be seen in comparison to other groups with either lower or higher amounts of baseline PA. Finally, the lower number of participants in the intervention group compared with the control group could possibly affect the outcome of the study.
In conclusion, this is the first time it has been shown that a childhood intervention with extra PA during a longer period is associated with a lower fracture risk. We must however emphasise that this is preceded by a transient higher fracture risk after introduction of the PA. Whether or not the fracture risk reduction remains after cessation of the intervention has to be evaluated.
References
Footnotes
MEC and JF contributed equally.
Contributors MEC and JF did all calculations, interpreted the data and wrote the manuscript. J-ÅN supervised the statistical analyses and the interpretation of the data. BER and MD collected data, planned the analyses and drafted the manuscript. CK drafted the manuscript. MKK designed the study, collected data and supervised all the work.
Funding This work was supported by the Centre for Athletic Research, the Herman Järnhardt Foundation, Skåne Regional Foundations and ALF Foundations.
Competing interests None declared.
Ethics approval Ethics Committee of Lund University, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.