Article Text

Abstract
Background Numerous studies have explored the association between educational inequalities and stillbirth but most have failed to elaborate how low educational attainment leads to an increased risk of stillbirth. We hypothesised that use of biomass fuels and consumption of unsafe water related to low educational attainment could explain the stillbirth burden in Ghana attributable to socioeconomic disadvantage.
Methods Data from the 2007 Ghana Maternal Health Survey, a nationally representative population-based survey were analysed for this study. Of the10 370 women aged 15–49 years interviewed via structured questionnaires for the survey, 7183 primiparous and multiparous women qualified for inclusion in the present study.
Results In a logistic regression analysis that adjusted for age, area of residence, marital status and ethnicity of women, lower maternal primary education was associated with a 62% (OR=1.62; 95% CI 1.04 to 2.52) increased lifetime risk of stillbirth. Biomass fuel use and consumption of unsafe water mediated 18% and 8% of the observed effects, respectively. Jointly these two exposures explained 24% of the observed effects. The generalised additive modelling revealed a very flat inverted spoon-shaped smoothed curve which peaked at low levels of schooling (2–3 years) and confirms the findings from the logistic regression analysis.
Conclusions Our results show that biomass fuel use and unsafe water consumption could be important pathways through which low maternal educational attainment leads to stillbirths in Ghana and similar developing countries. Addressing educational inequalities in developing countries is thus essential for ensuring household choices that curtail environmental exposures and help improve pregnancy outcomes.
- EPIDEMIOLOGY
- PUBLIC HEALTH
- SOCIAL MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The study was based on a large and representative sample.
The education–stillbirth relationship was illustrated in terms of smoothed curves of school years.
The exposure assessment method applied has limitations but has been widely used in environmental epidemiological studies and shown to be very good proxy measures of exposure.
Exposure misclassification was possible in the study owing to the inability to ascertain whether cooking fuel choices and drinking water sources of the households remained relatively stable throughout the pregnancies of the study participants.
Introduction
Stillbirth, the intrauterine death of any conceptus at any time during pregnancy,1 is a major public health concern in developing countries. An estimated 3.2 million stillbirths occur worldwide annually with 98% of these stillbirths found in developing countries.2 Important causes of stillbirths globally are asphyxia and infection associated with obstructed or prolonged labour, pre-eclampsia and eclampsia, chorioamnionitis, syphilis, malaria and poor nutritional status.3 Stillbirth occurrence has been noted to be much higher among ethnic minority, disadvantaged, marginalised and rural populations.4–6 This observation demonstrates the important role of socioeconomic factors in the aetiology of stillbirth.
The risk factors of stillbirth in low-income countries are associated with poverty7 including solid fuel use and consumption of unsafe water. Many households in developing countries rely on ground and surface water resources due to limited access to pipe-borne water, erratic supply, and high connection and utility charges. These water resources are often polluted by mining and agricultural activities, as well as nearby pit latrines which are also in widespread use in developing countries. Mining activities, especially in unregulated mines, lead to deposition/leaching of substantial amounts of chemicals such as cyanide and sulfuric acid, and heavy metals into nearby water bodies. Agricultural runoffs also introduce sediments, pesticides, fertilizers and pathogens into water bodies. Pit latrines have also been widely documented to leach microbial and chemical contaminants including coliforms, Escherichia coli, faecal streptococci, ammonia, nitrates and nitrites into groundwater resources.8 Poverty further hampers many households from treating these unwholesome water resources before usage. Solid fuels are also the predominant cooking fuel in developing countries owing to poverty and limited access to clean fuels.9 Bonjour et al10 estimated the proportion of households in Africa and Southeast Asia relying on solid fuels for cooking to be more than 60%. Studies have associated use of solid fuels11 and consumption of contaminated drinking water12–14 with stillbirth and other adverse pregnancy outcomes.
Socioeconomic characteristics including educational attainment are well documented to have strong effects on health outcomes including pregnancy outcomes. Several studies mostly emanating from high-income countries have explored the relationship between educational attainment and stillbirth but most have failed to elaborate how low educational attainment leads to an increased risk of stillbirth. We hypothesised that household use of biomass fuels and consumption of unsafe water related to low educational attainment could explain the stillbirth burden in Ghana attributable to socioeconomic disadvantage. As noted by Kramer,15 research that identifies and quantifies the causal pathways and mechanisms through which social disadvantage leads to higher risks of adverse pregnancy outcomes may help to reduce disparities and improve pregnancy outcomes across the entire socioeconomic spectrum.
We relied on data from the 2007 Ghana Maternal Health Survey (GMHS),16 a nationally representative population-based survey, that collected comprehensive information at the household and individual woman's level on maternal health issues including pregnancies, stillbirths, abortions and miscarriages and maternal deaths in the country.
Methods
Data from the 2007 GMHS16 were analysed for this study. GMHS was a nationally representative population-based survey that collected comprehensive information on maternal health and mortality in the country to provide baseline information for the Reducing Maternal Morbidity and Mortality (R3M) programme initiated in three regions (Greater Accra, Eastern, Ashanti) of Ghana in 2006. The survey design of GMHS involved the selection of 1600 primary sampling units (clusters) from the 10 administrative regions of the country, across urban and rural areas. The primary sampling units consisted of wards or subwards drawn from the 2001 population census.
Data collection was carried out in two phases with data for the present study deriving from the second phase. In the second phase, 400 clusters were randomly selected from the 1600 clusters with a long household questionnaire administered in 10 858 households (response rate, 98.8%) randomly selected from these clusters. These households were selected independently from the 227 715 households identified in the first phase (from the 1600 clusters) for profiling maternal deaths. Also in the second phase, a women's questionnaire was administered to 10 370 women aged 15–49 years (response rate, 97.6%) identified from the 10 858 households. The long household questionnaires collected information on the demographic and socioeconomic characteristics of members of the households sampled, whereas the women's questionnaire gathered information on a wide range of maternal health-related issues including live births, stillbirths, abortions and miscarriages and usage of health services in relation to these events.
To be eligible for inclusion in the present study, a woman must have given birth at least once (ie, primiparous and multiparous women). Of the 10 370 women aged 15–49 years, 7183 (69.3%) primiparous and multiparous women were eligible for the present study.
A flow chart of the survey sampling procedure and mothers included in the present study is depicted in figure 1.
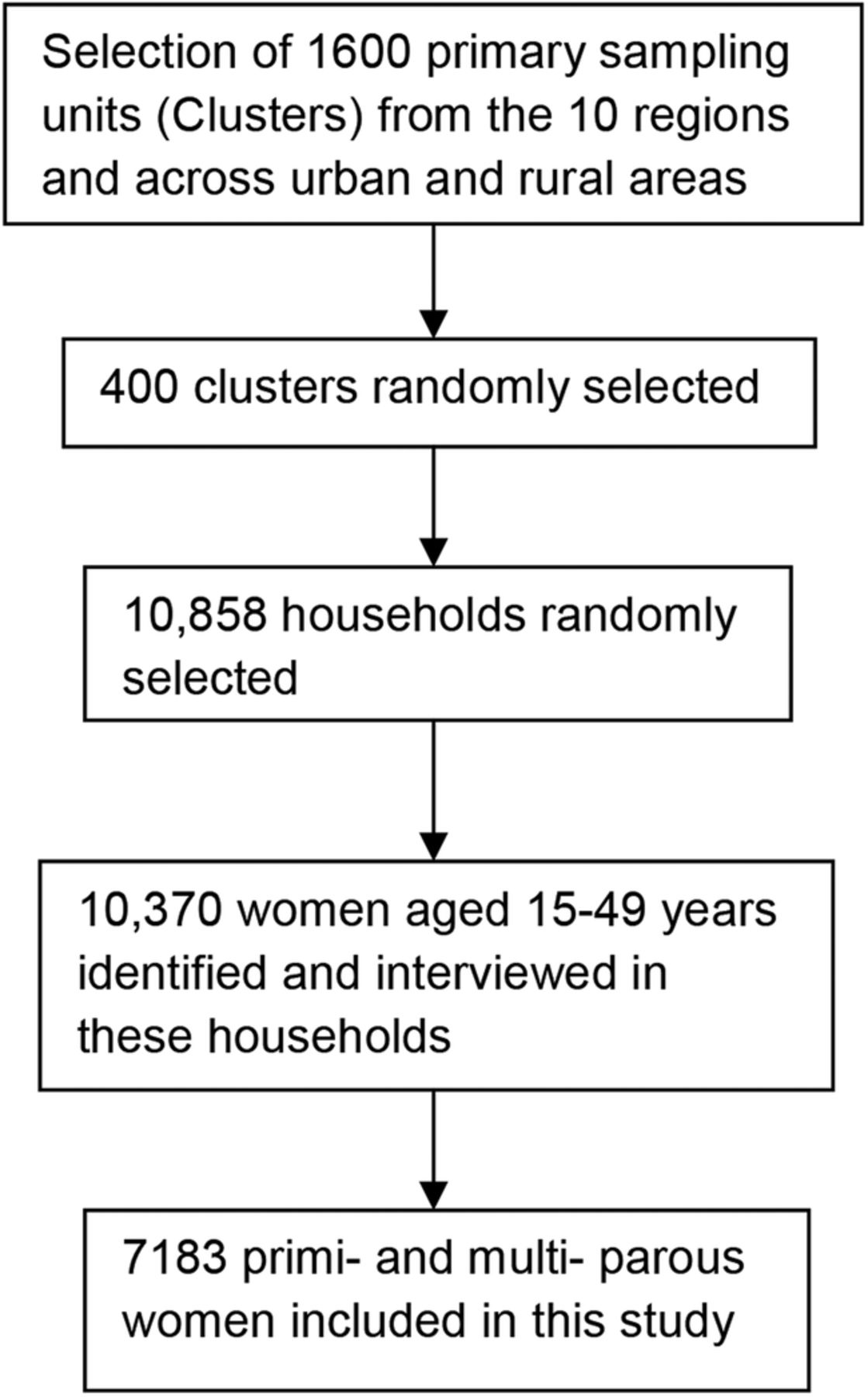
{kind=link}
Flow chart of the survey sampling procedure and mothers included in present study.
Ascertainment of educational attainment
In the women's questionnaire, respondents were asked whether they have ever attended school and if they answered ‘yes’ they were further asked about the highest level of school they attended and the highest grade they completed at that level. Maternal education was treated as a continuous and categorical variable in the analysis.
In treating maternal educational attainment as a continuous variable, we combined the information obtained from mothers who reported ever attending school into years of schooling (1–15 years). Mothers who never attended school were ranked zero on this scale.
The following levels of maternal education were applied in the analysis: none, lower primary (1–4 years of schooling), upper primary (5–6 years of schooling), some middle/junior secondary school (JSS) (7–8 years of schooling), completed middle school/JSS (9 years of schooling), secondary/senior secondary school (SSS) (10–12 years of schooling) and higher (≥13 years of schooling).
Assessment of exposure
Maternal exposure to household air pollution (HAP) was assessed by the type of fuel used by households for cooking. This information was obtained from the long household questionnaire. In this questionnaire, household heads were asked, ‘What type of fuel does your household mainly use for cooking?’ Mothers living in households using electricity, liquefied petroleum gas (LPG) and natural gas served as the reference category with those residing in households using charcoal, firewood and straw/shrubs/grass representing the exposed category. Kerosene, a non-solid fuel but with uncertainties about its cleanliness was excluded from the reference category. Very few households used coal/lignite, a non-biomass fuel for cooking and were thus excluded from the analysis.
Maternal exposure to contaminated drinking water was ascertained by the type of drinking water sources of the household. This information was also obtained from the long household questionnaire in which household heads were asked, ‘What is the main source of drinking water for members of your household?’ Mothers residing in households using piped and bottled/sachet water served as the reference category with those living in households sourcing water from surface (rivers, streams, lakes, dams, ponds, etc) and ground (wells, boreholes) waters representing the exposed categories. Mothers in households using spring water, rainwater and tanker water were excluded from the analysis because of the small number of households using these water resources.
Outcome of interest
The outcome of interest was lifetime experience of stillbirth (yes vs no) among primiparous and multiparous women. This information was extracted from the women's questionnaire where mothers were asked whether they have ever given birth in late pregnancy (7 months or more) to a dead child and if they answered ‘yes’, they were further asked about the number of stillbirths they have had in their lifetime.
Covariates
The following core potential confounders were adjusted for in the analysis: area of residence (urban, rural), age of woman, marital status and ethnicity.
Ethical consideration
Informed consent was obtained from all the participants before the interview.
Statistical analysis
We first described the education–stillbirth relationship in terms of relative risk by educational categories using logistic regression (PROC LOGISTIC). PROC LOGISTIC was used to estimate the effects of maternal education on the risk of stillbirth (yes, coded 1 vs no, coded 0) in a woman's lifetime, and to also establish whether a gradient in the risk exists. The analysis was adjusted for the core potential confounders.
We performed a causal pathway analysis using the difference method17 to establish the independent and joint mediating effect of biomass fuel use and consumption of unsafe drinking water in the observed educational differences in stillbirth risk. In brief, after controlling for the core confounders, biomass fuel use and unsafe water consumption were further independently and jointly added to the adjusted model with the mediation fractions computed using the formula below: where ORadjusted is the OR in the adjusted model and ORmediation is the OR in the independent and joint mediation models.
where ORadjusted is the OR in the adjusted model and ORmediation is the OR in the independent and joint mediation models.
We next illustrated the education–stillbirth relationship in terms of cubic smoothing splines using generalised additive modelling (GAM) with three degrees of freedom (df). Three df were chosen after fitting six separate models (df=3, 4, 5, 6, 7 and 8) and identifying the model with 3 df to have the best fit. The Akaike Information Criterion (AIC) was used to evaluate goodness of fit of the models fitted. AIC was estimated using the formula below: where D(θ) is the deviance and p is the number of parameters (df) in the model. The model with the smaller AIC value was deemed a better fit. The AIC values are presented in online supplementary table S1.
where D(θ) is the deviance and p is the number of parameters (df) in the model. The model with the smaller AIC value was deemed a better fit. The AIC values are presented in online supplementary table S1.
supplementary tables
GAM allowed maternal education to be applied as a continuous variable (school years), thereby increasing statistical power and enabling a better illustration of the predictor–risk relationship. Possible non-linearities in the maternal education data were explored by performing χ2 test of non-linearity. We stratified the curve fitting by urban and rural residence to ascertain whether there exist any marked differences.
SAS V.9.3 was used to perform all the analysis with the exception of the GAM which was performed with Stata 12.0.
Results
The characteristics of the study population are presented in tables 1 and 2. Close to one-third (31.9%) of the respondents were within the age group 20–39 years. More than half (68.6%) of the women reported being married with very few (6.4%) reporting that they have never been married. Close to half (46.3%) of the study population were resident in the R3M regions (Greater Accra, Eastern and Ashanti) with 19% of the women living in the three northern regions (Northern, Upper East, Upper West). More than half (58%) of the respondents were rural dwellers with about 17% of the respondents identified as city dwellers. Majority of the women (75%) were Christians with Muslims making up about 16% of the study respondents. Close to half (46%) of the women were Akans. Close to one-third (32.3%) of the respondents had no formal education with only 2.1% of the women educated up to the tertiary level or higher.
Demographic and background characteristics of the study respondents (n=7183)
Cooking fuel choices and drinking water sources of study respondents households (n=7182)
Biomass fuel, notably charcoal and firewood were the dominant cooking fuels of respondent's households with 91% of households using these fuels. LPG was used by 8% of the respondent's households. Whereas among highly educated mothers, LPG was the dominant fuel used (69%), among uneducated (77%) and primary educated (64%) mothers firewood was the fuel mostly used. Piped water (40%) and well/borehole (41%) were the dominant drinking water sources of the respondents. About 5% and 11% of the respondents used bottled/sachet and surface water, respectively. Secondary (59%) and highly (64%) educated mothers patronised piped water mostly. A quarter of highly educated mothers used bottled/sachet water. Among uneducated mothers, 53% accessed well/borehole water resources with 26% using piped water. Among primary and some middle school/JSS-educated women, the proportion using piped and well/borehole water resources were about the same.
The gravidity status and lifetime stillbirth experience of the women interviewed are presented in table 3. About 14% of the respondents were primigravida. About 6% of the respondents reported experiencing stillbirth in their lifetime with a small proportion (13%) of them experiencing this occurrence more than once. Uneducated mothers and mothers who completed middle/JSS recorded the highest proportion of lifetime stillbirths; 32% and 26%, respectively.
Gravidity status and lifetime stillbirth experience of study respondents classified by maternal education
Table 4 and online supplementary S2 present the ORs for the association between maternal education and lifetime stillbirth experience calculated from logistic regression. Lower primary education was associated with a statistically significant 62% (OR=1.62, 95% CI 1.04 to 2.52) increased risk of stillbirth in a lifetime after adjustment for the core covariates. Biomass fuel use and unsafe water consumption mediated 17.7% and 8.1% of the observed association of lower primary education on lifetime stillbirth risk. In the joint model, the mediation fraction was 24.2%. No consistent educational gradient was observed.
Binary logistic regression of lifetime stillbirth experience on maternal education (n=7183)
Online supplementary figure S1 depicts the smoothed curves for OR of stillbirth in a lifetime in relation to maternal years of schooling. Among all mothers, a very flat inverted spoon-shaped smoothed curve was observed. The OR of lifetime stillbirth increased slightly away from the reference level up to about 2.5 years of schooling, and declined slowly afterwards with further schooling. The 95% confidence band was generally wide especially towards the tail end of the smoothed curve. Among rural dwellers, a more pronounced inverted spoon-shaped smoothed curve was observed. Among urban dwellers, an s-shape smoothed curve with a generally wide 95% confidence band over the whole range of the maternal schooling years was observed.
supplementary figure
For all study participants (p=0.4166) and urban dwellers (p=0.6003), the non-linearity χ2 was not statistically significant. Among rural dwellers, the non-linearity χ2 was borderline significant (p=0.0558) thereby indicating possible departure from linearity. In the model adjusting for the mediating effect of biomass fuel use, the decrease in the OR of lifetime stillbirth after 6.5 years of schooling was very gentle. In the model adjusting for the mediating effect of unsafe water consumption, no appreciable change in the smoothed curve was observed and possibly confirms the small mediation fraction estimated in the logistic regression.
Discussion
We found lower maternal primary education to be associated with a 62% (OR=1.62; 95% CI 1.04 to 2.52) increased lifetime risk of stillbirth. Biomass fuel use and consumption of unsafe water mediated 18% and 8% of the observed effects, respectively. Jointly these two exposures explained 24% of the observed effects. The GAM revealed a very flat inverted spoon-shaped smoothed curve which peaked at low levels of schooling (2–3 years) and confirms the findings from the logistic regression modelling.
Validity issues
Selection bias was minimised in the study owing to the population-based nature of the GMHS survey and the high response rate (97.6%) achieved. Also the standardised data collection instruments and procedures of DHS surveys including the present, and the extensive training of interviewers guarantees the collection of reliable information from survey participants. On the issue of missing data, of the variables of interest concerned (education, marital status, ethnic group, cooking fuel type and drinking water source), the proportion of respondents with missing data was very low (<0.04%).
Educational attainment is a strong determinant of future employment and income,18 ,19 and certainly has implications for maternal health and pregnancy outcomes. The potential for outcome measurement bias is reduced in our study even though the outcome of interest was subjectively reported by the respondents. This is because stillbirth is a very traumatic experience that every mother with such an experience can vividly recollect.
Exposure to HAP and drinking water contaminants was assessed based on the primary cooking fuels and main drinking water sources of maternal households. There are limitations with the exposure assessment method applied but they have been widely used in environmental epidemiological studies and shown to be very good proxy measures of exposure. There is nonetheless the potential for exposure misclassification in the study with the direction of bias unclear. It was impossible to ascertain whether cooking fuel choices and drinking water sources of the households remained relatively stable throughout the pregnancies of the mothers interviewed. Regarding cooking fuel choices, it is often the case of households transitioning to fuels higher up the energy ladder with improved socioeconomic conditions and back to their traditional fuels as conditions deteriorate. With regards to drinking water sources, except in situations where communities have been connected to pipe-borne water, household water sources traditionally remain the same irrespective of improvement in socioeconomic conditions. It is possible that households connected to pipe-borne water after years of relying on ground and surface water resources will report use of pipe-borne water as their main drinking water source. This information bias, however, would rather underestimate the true effect.
The study adjusted for the effect of age of respondent, marital status, area of residence (urban vs rural) and ethnicity. We had no information on the smoking status of the mothers, but in Ghana only few women smoke. The 2008 Ghana Demographic and Health Survey20 estimated the proportion of women smoking cigarettes and other tobacco products to be 0.4%. Maternal smoking can therefore not be considered as a serious threat to validity in this study. We were unable to examine the confounding effect of prenatal and intrapartum care, maternal nutrition and anthropometry as well as malaria and sexually transmitted infections. However, with regards to infections, it has been suggested by Silver et al21 that they are more clearly associated with early stillbirth (20 weeks) than with late stillbirth (after 28 weeks). With the GMHS survey ascertaining stillbirths with a cut-off point of 7 or more months, we can assume that the associations reported are not likely to be confounded by maternal infections.
Synthesis with previous evidence
Our study adds to the weight of evidence emanating mostly from high-income countries22–26 on the adverse perinatal effects of low maternal educational attainment. We found lower primary education to be associated with a 62% increased risk of lifetime stillbirth. The smoothing curves also peaked at low levels of schooling (2–3 years) and declined with further schooling. A multicountry study27 conducted in six low-income countries and one middle-income country reported a 40% (RR=1.4; 95% CI 1.2 to 1.5) increased risk of stillbirth with no formal maternal schooling. Two recent population-based studies conducted in rural Ghana,28 ,29 however, found no association between maternal education and stillbirth. Ha et al28 reported small and statistically insignificant increased odds of antepartum and intrapartum stillbirth with no formal and primary maternal education. Engmann et al29 reported a much higher increased odds of stillbirth with no formal (OR=1.47; 95% CI 0.94 to 2.29) and primary/JSS (OR=1.48, 95% CI 0.95 to 2.30) maternal education. These associations were also not statistically significant. A systematic review and meta-analysis of the available evidence on the major risk factors for stillbirth in high-income countries26 found low educational attainment (<10 years of schooling) to be associated with 70% (OR=1.7; 95% CI 1.4 to 2.0; n=5) increased odds of stillbirth. The findings of our study are consistent with the findings of McClure et al27 and Flenady et al.26
Causal pathways
Medical care has been mentioned as the route through which education leads to inequality in stillbirth from placental abruption and cord compression.30 Suboptimal care including delayed recognition of medical problems or poor management has been noted to contribute to a significant proportion of stillbirths.31 Delayed access of prenatal care services owing to ignorance is very common in developing countries. Also common in developing countries is the inability of mothers to apply the nutritional and health messages received during prenatal visits for improved maternal and fetal health. This situation arises as a result of lack of education or low educational attainment of mothers. According to Galobardes et al,32 education may affect an individual's cognitive functioning and enable him/her to access appropriate health services, to better communicate with healthcare workers and to be more receptive to health education messages. Stephansson et al33 have also suggested that the socioeconomic differences in the risk of stillbirth can be attributed to social differences in seeking care for signs of pathological pregnancy such as reduced fetal movements.
In developing countries, besides access and usage of health services, there are other important pathways through which low educational attainment impacts on perinatal outcomes. Our study is the first to explore the mediating role of environmental factors in the maternal education–stillbirth relationship. Biomass fuel use and unsafe water consumption explained about 18% and 8% of the observed effects of low maternal educational attainment on lifetime stillbirth risk. Jointly, they mediated almost a quarter (24%) of the observed effect. A study in Ghana found the effects of low educational attainment on average birth weight to be substantially (62%) mediated by biomass fuel use.34 Studies in Ghana,35 ,36 Ethiopia,37 ,38 Cameroun39 and Kenya40 have reported educational attainment to be an important determinant of cooking fuel choices of households.
We must mention that the mediation fraction reported is likely to be overestimated and should be interpreted with caution. This is because prenatal and intrapartum care, maternal nutrition and other social factors which we were unable to control in the analysis are associated with educational attainment just as much as fuel and drinking water choices. It is thus possible that biomass fuel use and unsafe water consumption are essentially a proxy for these confounding variables and biasing the causal effect away from null as a result.
Conclusions
In conclusion, we provide evidence that in Ghana and similar developing countries, biomass fuel use and unsafe water consumption could be important pathways through which low maternal educational attainment leads to stillbirths. Women with no formal or low education should therefore receive extra care and support, and be alerted to household environmental risks to their pregnancies during prenatal visits. This recommendation could help curb the high stillbirth occurrence in developing countries. According to Goldenberg et al,41 each geographical area must understand the local causes of stillbirth, and the contexts in which they occur to enable prevention strategies to be developed and implemented.
Acknowledgments
We would like to thank Measure DHS for granting us permission to use the 2007 Ghana Maternal Health Survey data set for this research.
References
Footnotes
Contributors AKA conceived and designed the study, and performed the data analysis with guidance from SN and JJKJ. AKA wrote the manuscript with SN and JJKJ reviewing drafts for intellectual content. All authors read and approved the final version.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval The Ghana Maternal Health Survey was approved by the Ghana Statistical Service, Ghana Health Service and MEASURE DHS.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.