Article Text

Abstract
Introduction Atrial fibrillation (AF), the world’s most common arrhythmia, often goes undetected and untreated in low-resource communities, including India, where AF epidemiology is undefined. AF is an important risk factor for stroke, which plagues an estimated 1.6 million Indians annually. As such, early detection of AF and management of high-risk patients is critically important to decrease stroke burden in individuals with AF. This study aims to describe the epidemiology of AF in Anand District, Gujarat, India, characterise the clinical profile of individuals who are diagnosed with AF and determine the performance of two mobile technologies for community-based AF screening.
Methods This observational study builds on findings from a previous feasibility study and leverages two novel technologies as well as an existing community health programme to perform door-to-door AF screening for 2000 people from 60 villages of Anand District, Gujarat, India using local health workers. A single-lead ECG and a pulse-based application is used to screen each individual for AF three times over a period of 5 days. Participants with suspected arrhythmias are followed up by study cardiologist who makes final diagnoses. Participants diagnosed with AF are initiated on treatment based on current anticoagulation guidelines and clinical reasoning.
Analytical plan Age-stratified and sex-stratified prevalence of AF in the Anand District will be calculated for sample and estimated for Anand distribution using survey design weights. Sociodemographic and clinical factors associated with AF will be evaluated using multivariable regression methods. Performance of each mobile technology in detecting AF will be evaluated using a 12-lead ECG interpretation as the gold standard.
Ethics and dissemination This protocol was approved separately by the Institutional Review Board of University of Massachusetts Medical School and the Human Research Ethics Committee at Charutar Arogya Mandal. The findings of this study will be disseminated through peer-reviewed journals and scientific conferences.
- cardiac epidemiology
- valvular heart disease
- public health
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The Smartphone Monitoring for Atrial fibrillation in Real-Time in India study represents an innovative screening and referral paradigm for persons living in low-resource settings who may have an undetected chronic disease.
This study highlights the importance of conducting a feasibility study and engaging local community partners prior to undertaking more broad-based population screening efforts.
Serial screening and rigorous clinical follow-ups, which include continuous monitoring using a Holter device, increase the chances of identifying paroxysmal atrial fibrillation (AF) events. By contrast, most AF screening programmes described in the literature rely on a single-point screening.
Our efforts to characterise the clinical profile of participants diagnosed with AF are limited by the cross-sectional design of our study which prohibit us from drawing casual inferences.
Background
Clinical and public health significance
Although atrial fibrillation (AF) is the world’s most common serious heart rhythm problem, it often goes undetected and untreated, particularly in low-resource settings like India.1–5 As such, little is known about the epidemiology of AF in India.1–3 5 However, it is estimated that five million Indians have AF, based on ageing of the Indian population and limited data showing that the Indian population is increasingly affected by AF risk factors, including hypertension, diabetes mellitus and coronary heart disease.6 The importance of AF to Indian public health is underscored by an ongoing stroke epidemic with an estimated 1.6 million Indians experiencing a stroke in 2015.7 8 AF is a major risk factor for stroke conferring a fivefold higher risk among affected individuals compared with those free from the arrhythmia, suggesting that AF has become a major public health concern in India.8–10
Public health programmes for the routine surveillance of AF or other risk factors for stroke are sparse in India. A small proportion of Indian residents have access to routine cardiovascular care or prompt stroke treatment, and this subgroup is disproportionately clustered in urban and metropolitan cities. In light of the limited access to, and out-of-pocket costs associated with, stroke treatment, AF screening and treatment represent an appealing method for primary stroke prevention in rural India.7 Targeted AF screening has been employed successfully in high-income countries, such as the UK and Australia,11–14 but there are no major systematic efforts to screen for AF in low-income and middle-income countries. Furthermore, oral anticoagulation to prevent stroke is an effective therapy for patients with AF, but solutions are needed to assist those with limited means to pay for this treatment.5 15–17 Another major barrier to AF screening has been the resource intensiveness of performing conventional 12-lead ECG to diagnose AF.18 For these and other reasons, the importance of developing new, affordable, medical devices for AF screening that could be deployed in India was emphasised by an National Heart, Lung, and Blood Institution Expert panel and at the 2008 Hyderabad workshop.5
In this manuscript, we present an innovative community-based study called Smartphone Monitoring for Atrial fibrillation in Real-Time—India (SMART-India). Our approach deploys two novel smart device-based arrhythmia analysis technologies for AF screening using an existing network of community-health workers in rural Western India, medical professionals and provincial health leaders, and builds on a foundational feasibility assessment conducted in Gujarat, India. The SMART-India study is supported by our interdisciplinary Indo-US research team that has an ongoing collaboration between investigators with a proven track record of conducting community-based technology research in India.19
AF screening technology
Single-lead ECG device
Kardia’s Food and Drug Administration (FDA) approved AliveCor device records a single-lead ECG signal from the user. Participants place two or three fingers of their right hand and left hand on the two electrodes on the AliveCor device. Finger contact activates the recording of bipolar lead 1 and the signal is transmitted from the device to the iPhone by frequency modulation of an ultrasound signal.20 An automated algorithm, developed to interpret one’s cardiac rhythm, produces noise-filtered traces and a computer-averaged complex for arrhythmia diagnosis based on two criteria: p-wave absence and R–R interval irregularity. The developers of AliveCor device reported a sensitivity of 0.98 and specificity of 0.97 for the detection of AF against the gold-standard 12-lead ECG in the controlled developmental environment.20
Pulse-based ANAND application
Our team has developed a novel pulse-based approach for detecting arrhythmias that does not require additional hardware. This experimental Automated Novel Atrial fibrillation Noninvasive Detection (ANAND) application, named after our study site in India, builds on our previous USA-based algorithm to identify pulse complexity and irregularity.21 22 Participants are asked to hold the mobile phone in their hand, with their right first finger or second finger over the standard camera and lamp. The flashlight illuminates the finger and the pulse waveform is recorded for up to 2 min, with 30 s being needed in most cases to complete a rhythm analysis. The ANAND algorithm performs two calculations to approximate a person’s cardiac rhythm: (1) root mean square of successive difference of RR intervals to quantify variability between RR peaks and (2) Shannon entropy (or turning point ratio) to characterise the complexity of variability between two consecutive segments of 14 RR peaks.22 The results from this automated algorithm’s calculation on the waveform are classified as normal sinus rhythm, possible AF or indeterminate.21 The preceding prototype for ANAND application (app) was tested in a clinical environment and compared its performance against a manually adjudicated ECG reading demonstrating a sensitivity of 0.97 and a specificity of 0.94 for the detection of AF. This ANAND app is not commercially available and differs from the early prototype in two main aspects: a shorter duration of pulse recording and optimised threshold for RR variability and Shannon entropy based on data collected from our feasibility study.23
Feasibility study
In mid-2015, a feasibility study was undertaken in rural Western India to screen for AF using the two smartphone-based technologies: (1) the AliveCor device and (2) the ANAND app. Our primary objective for this study was to help identify the potential barriers and facilitators for conducting AF screening on a larger, more diverse and representative sample.
Our field staff for each village consisted of two undergraduate medical students who were trained in collecting field observation notes (online supplementary appendix A), a research coordinator, two social workers who were trained in administering questionnaires and using mobile technology to screen for AF and a local village health worker to help identify residents of the given village who meet the eligibility criteria. We screened a total of 354 participants aged 50 years and above, across six villages in Anand District in Gujarat. Each participant in this pilot study was screened for 2 min using both technologies for five consecutive days. Data was collected over a 6-week period. Key findings from field observation notes and in-depth interviews of the field staff are described in table 1. The sample prevalence of AF using the clinician’s adjudication of single-lead ECG recordings from the AliveCor device was found to be 5.1% (95% CI 2.7% to 8.7%).24
Supplementary file 1
Findings from the feasibility study and corresponding modifications in the SMART-India study
Community-based approach
Our approach builds on a long-standing collaboration between the University of Massachusetts Medical School and Charutar Arogya Mandal (CAM), a tertiary care hospital and medical college in rural Western India.19 This collaboration, which we have called Research and Advocacy for Health in India (RAHI: Hindi word for pathfinder), is grounded in extensive interactions with the local Indian communities. As we have described elsewhere,19 the research priorities of our collaboration and our studies are informed by community health needs assessments. The subsequent collaborative research plans are designed based on a dynamic process that incorporates feedback collected through iterations of community engagement activities. We discussed our findings from the feasibility study with the Community Extension Department at CAM, local community health workers and CAM clinical staff. Based on their feedback, we decided to leverage an existing CAM programme called SPARSH (Shree Krishna Hospital Programme for Advancement of Rural and Social Health; Hindi word for touch) to facilitate the community-based screening for AF.
SPARSH is a 5-year joint project by CAM’s Community Extension Department and Shree Krishna Hospital that is focused on non-communicable diseases. The ultimate goal of the SPARSH programme is to develop a three-tier healthcare system that reaches local villages at the grass-roots level. A total of 60 villages from the administrative district of CAM are enrolled in the SPARSH programme. In this programme, local village health workers, representing the first tier of three, are used to identify and register patients through an annual household survey, monthly camps and standardised screening programmes. These patients are then referred to the remote extension centres, representing the second tier of the SPARSH programme, where a medical officer assesses, educates and prescribes necessary treatment. Additionally, if a medical officer determines that further work-up is required, the patient is referred to the Shree Krishna Hospital, third tier, located at the main CAM campus. At the time of implementation of the SMART-India study, this three-tier referral system was not in place and, therefore, SMART-India relied exclusively on the census collected by village health workers as part of their annual household survey.
Methods/design
Objectives
Box lists the primary objectives of the SMART-India study. These objectives are informed by the feasibility study, AF-screening technology and community-based approach.
Study aims for Smartphone Monitoring for Atrial fibrillation in Real-Time—India
Aim 1: Describe the epidemiology of atrial fibrillation (AF) in Anand District, Gujarat, India. Screen 2000 residents of Gujarat to describe the age-stratified and sex-stratified prevalence of AF.
Aim 2: Characterise the profile of individuals who are diagnosed with AF. Compare clinical findings, quality of life and risk factors of participants who are diagnosed with AF with those who do not have AF.
Aim 3: Determine the performance of two mobile technologies for community-based AF screening. Determine the sensitivity, specificity and discriminative ability of the AliveCor and Automated Novel Atrial fibrillation Non-invasive Detection’s automated AF detection algorithm to the gold-standard 12-lead ECG as well as interpretation by a trained clinician.
Study design
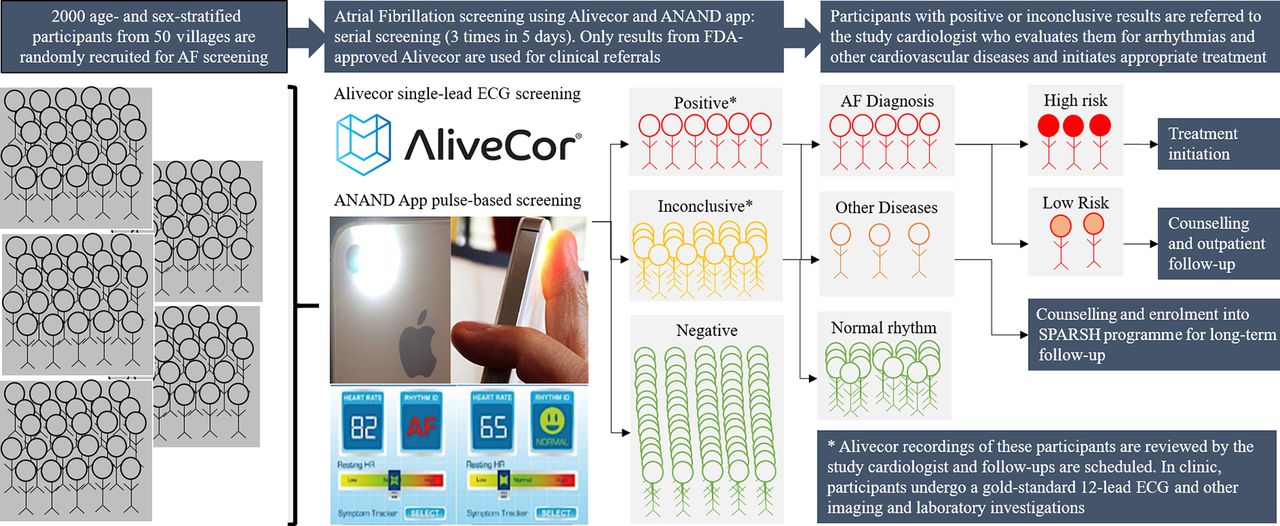
Figure 1 provides an overview of the SMART-India study protocol from the perspective of prospective participants. The SMART-India study is a cross-sectional screening of 2000 adult men and women aged 45 years and older from 60 villages participating in the SPARSH programme paired with a clinical follow-up of all participants with abnormal screenings. Each participant is screened three times over the course of 5 days to account for potential paroxysmal AF presentation.

An overview of SMART-India study protocol for community-based screening of AF and referral for clinical follow-up in rural Western India. AF, atrial fibrillation; ANAND, Automated Novel Atrial fibrillation Noninvasive Detection; app, application; FDA, Food and Drug Administration; SMART-India, Smartphone Monitoring for Atrial fibrillation in Real-Time—India; SPARSH, Shree Krishna Hospital Programme for Advancement of Rural and Social Health.
Staff training
The SMART-India study is supported by 4 field workers, 1 clinical coordinator, 1 project supervisor and 50 village health workers. The field workers and clinical coordinator received 2 weeks of training in the use of smartphones and devices to administer questionnaires to surveyed individuals and perform screening for AF. Additionally, the five staff members worked with the investigators to develop standardised operating procedures for their tasks. Following training, the five team members collaborated with the study investigators to organise a 1-hour orientation for the 60 village health workers. Participants from 50 villages took part in this study, while volunteers from the other 10 villages had participated in the feasibility study described earlier. Training provided the village health workers with information about the study, their roles and introduction to the rest of the study team. During the orientation, village health workers indicated that navigating the village to identify participants listed in the roster would be the primary time constraint. Thus, we divided the four field workers into two teams and proceeded with simultaneous screenings in two separate villages to enhance efficiency. One of the Indian co-investigators on the team fulfilled the role of project supervisor.
Questionnaire translation and testing
We use standardised questionnaires to collect information about participants’ demographic characteristics, lifestyle risk factors, past medical history, family history, physical activity, medication, AF-related symptoms and healthcare usage at the time of the first screening (table 2). Additionally, we administer an exit survey to ascertain participants’ feedback about the screening technology and a clinical follow-up survey to assess participants’ quality of life and cardiovascular-related factors. All questionnaires were translated to Gujarati and interpreted by several volunteers representing a wide range of literacy (ie, attending physician, healthcare worker, research coordinator, village health worker and community representative). The interpretations of questions and responses were back-translated and compared with the original questionnaire in English. Common themes for discordance between the original and back-translated forms were identified and used to modify the original questionnaire to accommodate the cultural context. This process was repeated until there was convergence between the two versions. All translations were done by certified professional translator services in Gujarat, India.
Data collected using standardised questionnaires during enrolment, final screening and follow-up time points for Smartphone Monitoring for Atrial fibrillation in Real-Time—India study
Data management
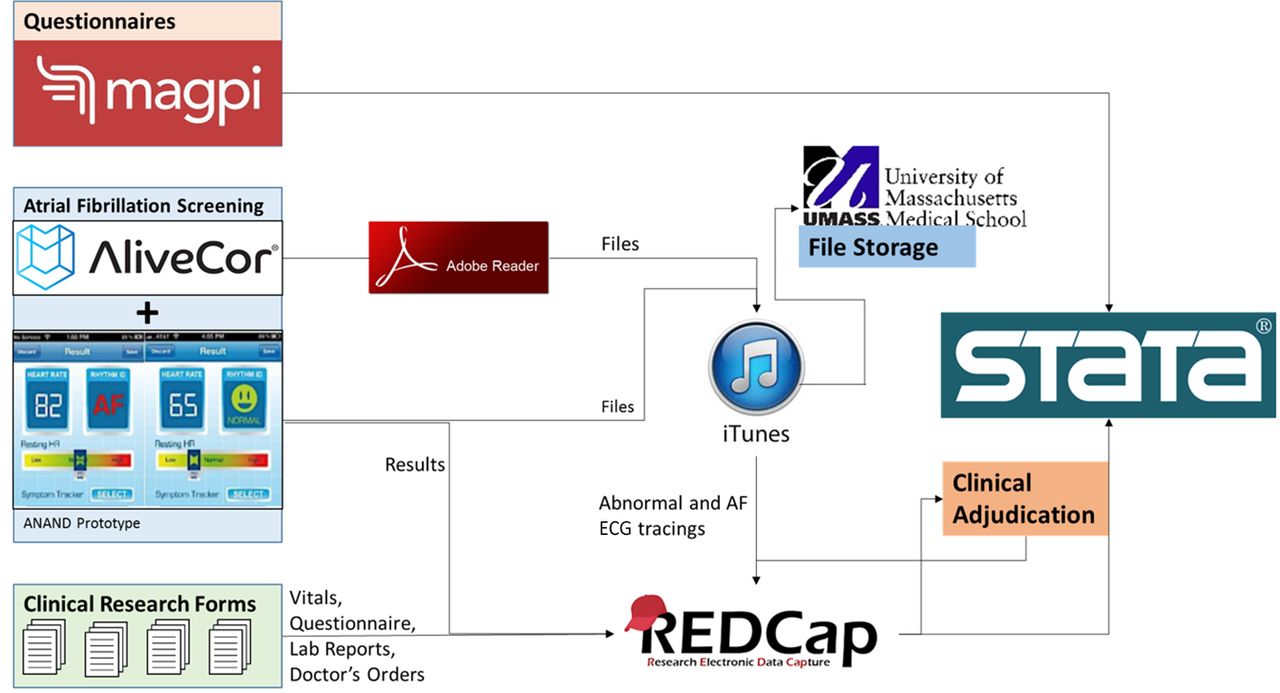
Figure 2 describes the data management strategy for SMART-India study. Based on our prior experience, we use the Magpi platform to administer questionnaire-based surveys to the participants. Magpi allows for off-line data collection in smartphones and tablets through a user-friendly app and uploads collected data to a secure server once the device connects to the Internet. The files from the AF screening apps (AliveCor and ANAND) are downloaded to a personal computer from the phones using iTunes. Results from the automated algorithm of AF screening apps and all abnormal AliveCor ECG tracings are uploaded to REDCap. Additionally, all data emerging from the clinical follow-up, except for questionnaire-based surveys, are uploaded to REDCap. REDCap is used because it allows for file uploads and can create reports that are helpful during the adjudication process.

An overview of data management for SMART-India study. Questionnaire data is collected using Magpi platform, screening files are imported through iTunes, and clinical forms as well as abnormal recordings are stored in REDCap. Logo credit: Magpi Inc (www.home.magpi.com); AliveCor (www.AliveCor.com); Adobe Reader (www.acrobat.adobe.com); iTunes (www.apple.com/itunes); REDCap (www.project-redcap.org); Stata (www.stata.com)
Sample size calculations
Based on our calculations, a sample size of 1823 persons is required to estimate the prevalence of AF with 1% error assuming the a priori prevalence of AF to be 5% based on our feasibility study. The resultant stratum size of 300 people can estimate the subpopulation prevalence of 5% with a 95% CI of 2.8% to 8.1%. An effective screening tool maximises sensitivity to avoid false-negative findings. Assuming a 5% prevalence of AF, a sample size of 2000 participants (5% AF rate, n=100) or more is necessary to obtain a satisfactory confidence band for 90% sensitivity for study aim 3 (table 3). Considering the extent of resources available, the study team decided to screen 2000 adult men and women 45 years and older to accomplish the aims outlined in box.
95% CI for sensitivity and specificity by number of participants to justify the sample size of 2000 participants for the Smartphone Monitoring for Atrial Fibrillation in Real-Time in India (Smart-India)study (assumes 5% prevalent atrial fibrillation)
Community-based screening
Prescreening preparation
One week prior to screening, field workers for study team A and team B contact the respective village health workers to inform them of the screening plan. Both teams develop an age-stratified and sex-stratified recruitment roster for their respective villages based on the census provided by the SPARSH programme. In total, six strata are defined for the combination of age (40–55, 56–65 and 65+ years) and sex (male and female) categories. Teams print out recruitment and screening tracking forms (online supplementary appendix B) and charge the smartphones and portable powerbanks for use during the week.
Supplementary file 2
Screening protocol
Recruitment and enrolment occurs on day 1 and day 2 of the screening process. The two study teams accompany their respective village health workers to enrol 21 willing participants in their respective villages on a daily basis. Each participant is screened using the AliveCor device for 1 min, with the AliveCor device placed on the clipboard (figure 3), followed by the ANAND app for 1 min 30 s. Results are recorded in the tracking form. If the participant is screened for either unclassified or unreadable heart rhythm on AliveCor, two more attempts are made to obtain either a normal or possible AF automated reading. Following this screening process, each participant completes the enrolment questionnaire that is entered directly into the Magpi database by the field assistants. Village health workers perform random blood glucose testing and measured the blood pressure of all participants. On day 3, both field teams attempt to screen all 42 participants using the AliveCor device and ANAND app. A successful follow-up, number of attempts required and whether or not the screening occurred at home is recorded in the tracking form. On day 4 and day 5, the third screening for AF is again split into 2 days. If a participant is not available on day 3, field workers approach them on both days to perform a total of three screenings over 5 days. Thus all participants are screened 1 and 2 days apart, unless they are unavailable during their follow-up screening. After the final screening was completed, the field workers administer an exit survey, and data is entered directly into Magpi forms. The results of all screenings are recorded on paper and entered into REDCap along with the AliveCor ECG recordings for those who have an abnormal finding.

A field worker is collecting single-lead ECG recording from a SMART-India participant. The participant is asked to place her fingers on the AliveCor device that is supported by a clipboard to minimise motion-noise artefact. The participant approved the use of this picture and provided consent for its use. SMART-India, Smartphone Monitoring for Atrial fibrillation in Real-Time—India.
Postscreening activities
On each of the final 2 days (day 4 and day 5) of screening, field workers travel back to CAM to complete data entry and upload all abnormal (possible AF/unclassified) ECG files to REDCap. All AliveCor and ANAND files are downloaded from the phones using iTunes. All AliveCor portable document formats are renamed with patient IDs and separated into normal results versus AF/unclassified results. All AF/unclassified files are uploaded to REDCap and flagged for adjudication. The field workers create a weekly report to summarise recruitment and results of screening and distribute it with the team (online supplementary appendix C). All of the ANAND and AliveCor files are uploaded to a secure server to support ad hoc analyses for measuring the performance of the two screening methods. Ultimately all data are exported to STATA for statistical analyses (figure 2).
Supplementary file 3
Clinical follow-ups
Our protocol for clinical follow-ups evolved over time based on feedback from the research team. The primary impetus behind the change in approach was higher than expected number of screenings that are classified as inconclusive and the resultant backlog of follow-up visits needed to understand these inconclusive readings. In order to facilitate prompt clinical visits for high-risk participants, we introduced a triaging step (Modifications for follow-up scheduling) after reviewing the clinical charts and final diagnosis for the first 50 participants that were followed up in clinic.
Scheduling follow-ups
The clinical coordinator schedules all follow-up visits with village health workers. One day prior to the visit, the clinical coordinator informs the cardiac and extension departments about the number of participants and which village health workers are coming. The clinical coordinator prints out the abnormal ECGs and paper clinical forms to prepare for the follow-up visit.
Follow-up protocol
The clinical coordinator meets the village health workers and participants at the hospital and escorts them to the cardiac centre. Once at the cardiac centre, the clinical coordinator conducts further AF screening using the AliveCor device and ANAND app using the same methodology as in the field. Subsequently, all participants receive a 12-lead ECG. The study cardiologist reviews all of the ECG recordings (field and clinical visit) and determines whether or not to pursue additional clinical work-up. While waiting for the cardiologist’s interpretation, the clinical coordinator administers the follow-up survey in Magpi, recorded vital information as measured by the nurse (height, weight, blood pressure, heart rate, O2 saturation, temperature) and verified the participants’ medical history. The cardiologists’ clinical decision-making is described in figure 4. If the cardiologist interprets all ECG recordings of the participant as showing normal sinus rhythm, no additional studies are ordered. If the cardiologist diagnosed the participant as having definite AF in any of the ECG, either in any of the screening ECG or in-office ECG, additional laboratory investigations are performed to inform clinical decision-making about initiation of anticoagulation and management plan (figure 4). If AF was suspected on any of the screening ECG but a diagnosis of definite AF could not be made due to poor quality of ECG tracings from screening app, multiple atrial or ventricular premature complexes, or a normal sinus rhythm on the 12-lead ECG, the cardiologist orders 24-hour Holter monitoring to look for paroxysmal AF events or other abnormalities. Two-dimensional echocardiography is performed in all participants diagnosed with AF and in those having symptoms and/or ECG abnormalities that warrants for an echocardiographic examination. Decision to initiate anticoagulation is taken based on Congestive heart failure, Hypertension, Age 75+ years, Diabetes mellitus, Stroke, Vascular disease, Age 65-74 years, Female sex (CHA2DS2-VASc) score.25 All of the clinical data including medications is abstracted by the clinical coordinator using clinical research forms.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A flow chart describing the clinical decision-making of the study cardiologist for participants following up in clinic for abnormal screening results during SMART-India study. CHA2DS2-VASc, Congestive heart failure, Hypertension, Age 75+ years, Diabetes mellitus, Stroke, Vascular disease, Age 65-74 years, Female sex; HbA1c, glycated haemoglobin; SMART-India, Smartphone Monitoring for Atrial fibrillation in Real-Time—India.
Modifications for follow-up scheduling
A preliminary inspection of clinical follow-ups found that the majority are due to an ‘inconclusive’ finding of AliveCor ECG recording based on Kardia’s automated algorithm. Specifically, 44 out of the first 50 follow-ups are of participants whose screening was inconclusive. Out of these 44 participants, 41 were found to have normal sinus rhythm after the study cardiologist interpreted field and 12-lead clinical ECGs. Additionally, two of the remaining three participants were found to have benign, non-AF arrhythmias. Based on these findings, we modified our follow-up protocol by having the study cardiologist triage the single-lead ECG recordings from the field prior to the participants’ clinical follow-ups to prioritise high-risk patients and rule out false-positive recordings.
Data adjudication
All interpretations of ECG recordings determined as AF or abnormal by the AliveCor automated algorithm are reviewed by a separate team of trained clinicians through a standardised adjudication process. Two resident-level physicians independently review each abnormal AliveCor generated ECG recording using REDCap and enter their interpretation as either: (1) normal sinus rhythm, (2) AF or (3) as an other arrhythmia (free text). In the event of disagreement between the two reviewers, a fellow-level physician reviews the ECG recording.
Analytical plan
Aim 1: AF epidemiology
The gold standard of cardiologist-verified diagnoses of AF will be used to calculate the age-stratified and sex-stratified prevalence of AF in the study sample. Population estimates will be derived from the sample prevalence using survey weights constructed using the census collected by the SPARSH programme and the Government of India sponsored census in 2011. Three separate calculations will be performed to describe the overall prevalence of AF and separately for those with valvular AF and non-valvular AF.
Aim 2: Profile of patients likely to have AF
Distribution of covariates (table 1) across group of participants diagnosed with AF will be compared with those who were not diagnosed with AF to determine associated risk factors. Sensitivity analyses will be performed to rule out differences between the group of participants who were not diagnosed with AF but were followed up clinically in comparison with those who were never followed up. If meaningful differences are identified in our sensitivity analyses, distribution of covariates will be assessed across the three different groups of participants. Additionally, among those participants who are followed up clinically, differences in the distribution of clinical factors between the group of AF-positive and AF-negative participants will be assessed. For sociodemographic and clinical risk factors, multivariable regression techniques will be used to identify their conditional effects after accounting for other covariates. Lastly, among the participants who were followed up clinically, the effects of AF will be estimated by comparing differences in the quality of life score ((Short Form-12 Survey) SF-12, table 1) between groups of participants who are diagnosed for AF versus those who do not have AF. Potential confounders will be identified based on a priori knowledge (age, sex, socioeconomic status) and an examination of bivariate association of sociodemographic factors with AF and quality of life.
Aim 3: Performance of AF-screening technology
Sensitivity, specificity and discriminative ability (receiver operating characteristic curve analyses) with 95% CI bands will be used to measure the performance of our AF-screening technology in field and in clinic (table 4). In-field performance of AF-screening technology will be used by comparing results from the ANAND and AliveCor automated algorithms with the gold standard of adjudicated interpretations of the AliveCor ECG recordings. The clinical performance of AF-screening technology will be assessed by comparing results from the automated algorithms from both technologies with results from the gold-standard 12-lead ECG.
Validation strategy to assess performance of atrial fibrillation screening technology
Limitations and strengths
It is important to consider that this study screens people of villages from rural Indian region who live in villages enrolled in SPARSH programme that is focused on addressing non-communicable diseases and its risk factors. Therefore, the participants recruited in this study may under-represent the true burden of AF risk factors present in rural Indian population. Additionally, ascertainment of certain lifestyle-related AF risk factors is based on self-report, which is prone to under-reporting. Mobile technologies are used to perform multiple AF screening to account for potentially paroxysmal nature of AF. This approach, although superior to single time point screening, is vulnerable to missing AF. However, we attempt to partially address this limitation by obtaining a 24-hour Holter recording for participants who experience rhythm abnormalities on AliveCor or 12-lead ECG but may not be classified as AF.
Discussion
The SMART-India study represents an innovative screening and referral paradigm for persons living in low-resource settings who may have an undetected chronic disease. Our study also highlights the importance of conducting a feasibility study and engaging local community partners prior to undertaking more broad-based population screening efforts. Findings from this study will provide greater insights into the silent burden of AF in rural Indian communities and help identify potential targets for intervention to modify the ongoing epidemic of stroke in India. The potential public health impact of the SMART-India study is particularly noteworthy in light of a recent white paper on AF screening which reported that AF detected during a screening procedure is not a benign condition and carries a sufficient risk of stroke.14 Further work is needed to build on the SMART-India study and build a nexus of providers that can help triage high-risk patients and further enhance the efficiency of a referral system for persons with suspected chronic disease, including cardiovascular disease. Leveraging existing community-based programmes, such as SPARSH, can help achieve this ambitious, but feasible, goal.
Ethics and dissemination
The SMART-India study was reviewed and approved by ethical boards from the University of Massachusetts Medical School (IRB number H00008089) and CAM (HREC number IEC/HMPCMCE/70/Faculty/15/160/16). The primary outcomes of this study will be disseminated through annual scientific conferences and three separate peer-reviewed publications, one corresponding to each objective. Additionally, the authors will share data with ongoing coalition efforts to better understand global epidemiology of AF and to guide the development of more robust AF screening programmes in resource-limited settings.
References
Footnotes
Contributors AS, NF, SR, ST conceptualised, designed and implemented the study in India. AS drafted the initial manuscript and approved the final manuscript as submitted. SK, HP, JB, KT, RS contributed to the design and implementation of the study in India. SK, SR, JB, RS, RG, AGP, JJA, SMN, DDMM contributed to the drafting of the manuscript and approved the final manuscript as submitted. HP, NF, KT contributed to the drafting of the initial manuscript and approved the final manuscript as submitted. AH contributed to the design of the study, drafting and formatting of the manuscript, and approved the final manuscript as submitted. SB contributed to the implementation of the study in India, editing of the manuscript and approved the final manuscript as submitted. RG, AGP conceptualised and designed the study in India. ST provided input to the analyses, contributed to the drafting of the manuscript and approved the final manuscript as submitted. JJA, SMN, DDMM conceptualised and designed the study in India and supported its implementation. KC supported the implementation of the study in India. JJA contributed to the drafting of the manuscript and approved the final manuscript as submitted.
Funding This study is supported by 2016 University of Massachusetts Medical School Office of Global Health Pilot Project Grant. AS received support from the National Center for Advancing Translational Sciences (TL1-TR001454) and JJA received support from the National Institute on Minority Health and Health Disparities (P60-MD006912-05). DDMM’s time was supported by KL2RR031981, 1R15HL121761-01A1, 1UH2TR000921-02 and 1R01HL126911-01A1 from the National Heart, Lung and Blood Institute.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Competing interests DDMM discloses equity stakes or consulting relationships with Flexcon, Inc., Bristol-Myers Squibb, Inc., Mobile Sense, Inc., ATRIA, Inc. and Boston Biomedical Associates, Inc. He has also received research funding from Sanofi Aventis, Inc., Otsuka Pharmaceuticals, Inc., Philips Healthcare, Inc., Biotronik, Inc. and Pfizer, Inc.
Patient consent Obtained.
Ethics approval UMMS IRB & CAM HREC.
Provenance and peer review Not commissioned; externally peer reviewed.