Article Text

Abstract
Objectives Prehospital intravenous access is a common intervention for patients with out-of-hospital cardiac arrest (OHCA). We aimed to assess the effectiveness of prehospital intravenous access and subsequent epinephrine administration on outcomes among OHCA patients.
Methods We conducted a prospective cohort study of patients with OHCA from non-traumatic causes aged ≥18 years in Osaka, Japan from January 2005 through December 2012. The primary outcome was 1-month survival with favourable neurological outcome defined as a cerebral performance category of 1 or 2. The association between intravenous line placement and survival with favourable neurological outcome was evaluated by logistic regression, after propensity score matching for the intravenous access attempt stratified by initial documented rhythm of ventricular fibrillation (VF) or non-VF. The contribution of epinephrine administration to the outcome was also explored.
Results Among OHCA patients during the study period, 3208 VF patients and 38 175 non-VF patients were included in our analysis. Intravenous access attempt was negatively associated with 1-month survival with a favourable neurological outcome in VF group (OR 0.76, 95% CI 0.59 to 0.98), while no association was observed in the non-VF group (OR 1.06, 95% CI 0.84 to 1.34). Epinephrine administration had no positive association in the VF patients (OR 0.75, 95% CI 0.51 to 1.07) and positively associated in the non-VF patients (OR 1.52, 95% CI 1.08 to 2.08) with the favourable neurological outcome.
Conclusions Intravenous access attempt could be negatively associated with survival with a favourable neurological outcome after OHCA. Subsequent epinephrine administration might be effective for non-VF OHCAs.
- Cardiac arrest
- cardiopulmonary resuscitation
- intravenous access
- epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Prospectively collected population-based data on intravenous access attempts.
A propensity score matching of intravenous access attempts at the decision point of emergency life-saving technicians (ELSTs) in the real world.
Being lack of data on the skill level of ELSTs, the quality of cardiopulmonary resuscitation, information on in-hospital advanced measures after hospital arrival.
The presence of unmeasured or unknown confounding factors that may have influenced the results.
Introduction
Out-of-hospital cardiac arrest (OHCA) is one of the leading causes of death in the world.1 In Japan, approximately 120 000 cardiac arrest events occur every year,2 and survival from OHCA remains low in spite of improvements in the ‘chain of survival’ and the revision of cardiopulmonary resuscitation (CPR) guidelines.3–6
There is little evidence to evaluate intravenous access and subsequent epinephrine administration for OHCAs with adjustment of inherent indications for intravenous line placement in actual prehospital settings. Current guidelines suggest that epinephrine be given during resuscitation of patients with OHCA with weak recommendation of very low-quality evidence.1 Although epinephrine is expected to have pharmacological effects as a potent vasoconstrictor and coronary artery vasodilator during CPR,7 8 several studies have suggested poor neurological outcomes of epinephrine administration for OHCA patients in prehospital settings.9–11
In Japan, the emergency medical service (EMS) system is well-managed nationwide by the Fire and Disaster Management Agency and is operated by local fire departments. Usually, each ambulance has a crew of three emergency providers including the emergency life-saving technicians (ELSTs), the most highly trained prehospital emergency care providers. EMS personnel provided advanced life support measures only for OHCA patients who did not get a return of spontaneous circulation (ROSC) after a series of basic life support measures such as chest compressions and defibrillations. ELSTs have been allowed to place a peripheral intravenous line since 1991, and specially trained and certified ELSTs were permitted to administer epinephrine following intravenous line placement in 2006.12 ELSTs administered epinephrine neither through the intraosseous (IO) route nor intratracheal route but only through the intravenous access.
The aim of this study was to evaluate the effect of intravenous route access on favourable neurological outcomes after OHCA. The contribution of subsequent epinephrine administration to the outcomes was also explored.
Methods
Settings
This was a prospective population-based cohort study conducted in Osaka Prefecture, Japan from January 2005 through December 2012. Osaka Prefecture had an area of approximately 1905 km2 and a population of approximately 8.8 million in 2014.13 14 There were 34 fire departments with dispatch centres in Osaka Prefecture, and municipal governments provided EMS. Do-not-resuscitate orders or living wills are not widely accepted in Japan, and EMS personnel are prohibited from terminating resuscitation in the field. Therefore, all patients with OHCA who were treated by EMS personnel were transported to hospitals.
Participants
The Utstein Osaka project was a prospective, population-based registry system of OHCA based on the standardised Utstein-style reporting guidelines for cardiac arrests.15 16 Details of the project were published elsewhere.3 We included all persons aged 18 years or over with OHCA of non-trauma origin. Among patients with initial rhythm of VF, we included only those who did not respond to the first defibrillation as those patients rarely have intravenous access attempt. Cardiac arrest was defined as the cessation of cardiac mechanical activities, as confirmed by the absence of signs of circulation.15
We collected data on ELSTs’ attempts of intravenous route access and their results. Throughout the study period, ELSTs were authorised to insert an intravenous route and to place advanced airway management devices on OHCA patients under online medical control direction when patients did not get ROSC after a series of basic life support procedures. They recorded the intravenous route to have been successfully placed when they could administer intravenous fluids by the access. If a patient had already had an intravenous route access made in a healthcare facility, they recorded the access as not to be attempted.
We also obtained variables including age, gender, location of arrests, activity of daily living (ADL) before arrests, year, presence of bystander’s witness, details of bystander-initiated CPR, medical control council (MC) in charge, epinephrine administration (yes, no), advanced airway management, origin of arrests (trauma, non-trauma) and initially documented rhythms.
Initial documented rhythm was recorded and diagnosed by the EMS personnel with semiautomated defibrillators on the scene and confirmed by the physician who was responsible for online medical direction. When laypersons delivered shocks using a public-access automated external defibrillator, the first documented rhythm was regarded as ventricular fibrillation (VF). The data form was filled out by the EMS personnel in cooperation with physicians in charge of the patients and transferred to the Information Center for Emergency Medical Services of Osaka. When a data sheet was incomplete, it was completed by getting in contact with the relevant EMS personnel. Data on bystander CPR were obtained by the EMS observation and an interview with the witness before leaving the scene, by asking specific questions regarding the presence or absence of chest compressions and rescue breathing.
Endpoints
All survivors were followed for up to 1 month after the event by the EMS personnel in charge. Neurological outcome was determined by a follow-up interview to the EMS personnel in cooperation with the physicians in charge of the patient 1 month after successful resuscitation, using the Cerebral Performance Category (CPC) scale17: category 1, good cerebral performance; category 2, moderate cerebral disability; category 3, severe cerebral disability; category 4, coma or vegetative state; and category 5, death.
The primary outcome measure of this study was 1-month survival with a favourable neurological outcome, which was defined as CPC category 1 or 2. Secondary outcome measures included a ROSC before hospital arrival and 1-month survival.
Statistical methods
Baseline characteristics were summarised in numbers and percentages for categorical variables, and means and SD for continuous variables. All participants were divided into two groups according to their initially documented rhythms, VF or non-VF. Propensity scores (PS) modelling likelihood of intravenous access attempts compared with no attempt were calculated by fitting a logistic model with the following variables: year, age, gender, ADL, place, presence of bystander witness, bystander CPR details, MC, presence of a certificated ELST for epinephrine administration and type of airway devices used. The variables included in the model were chosen as factors that may influence intravenous access attempt. As each MC cover different area and is trained differently for intravenous access attempt for OHCA, we included MC in the model to calculate PS. We performed PS matching in a one-to-one fashion between the intravenous access attempted group and the non-attempted group using callipers with a width equal to 0.2 of the SD of the logit of the PS.18 Covariate balances before and after matching were checked by comparing standardised mean differences. A standardised difference <10% was considered to indicate successful balancing.19 Logistic regression analyses were performed to assess the association of intravenous access attempt with the endpoints. We also exploratory analysed the association of successful intravenous access placement, epinephrine administration and the endpoints. Moreover, ORs and their 95% CIs were calculated. All statistical analyses were performed using V.3.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
Ethics
The project protocol was approved by the institutional review board of Osaka University, with the approval of the EMS authorities and local governments in Osaka Prefecture. The requirement of written informed consent was waived.
Results
Participants
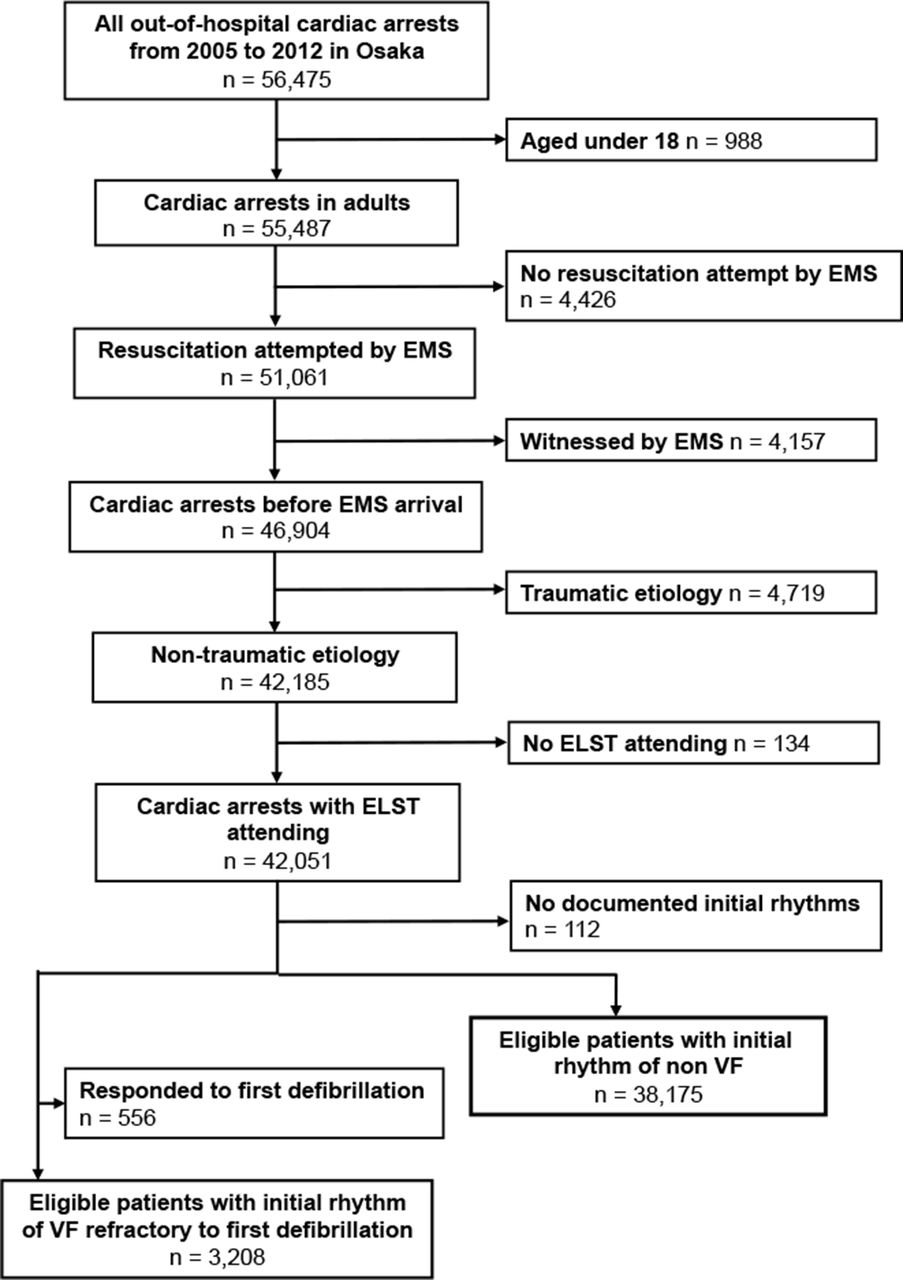
A total of 56 475 OHCAs were registered during the study period. Among them, 55 487 were adults aged 18 years or older, and 51 061 had resuscitation attempted by EMS. Among those 51 061, 46 904 OHCA patients had cardiac arrests before EMS arrival, 42 185 of which were non-traumatic cardiac arrests, and 42 051 ELSTs treated cardiac arrests. Among 3764 patients with initial rhythm of VF, 556 patients responded to the first defibrillation, and the remaining 3208 patients were eligible to this study. Non-VF rhythm was documented in 38 175 (figure 1).

{kind=link}
Flowchart of the study. EMS, emergency medical service; ELST, emergency life-saving technician; VF, ventricular fibrillation.
Patient characteristics and intravenous access attempt, success and epinephrine administration
Table 1A shows characteristics of eligible patients with VF rhythm, and table1B shows those of patients with non-VF rhythm. In the VF group, intravenous access was attempted in 1642/3208 (51.2%) and the success rate was 878/1642 (53.5%). In the non-VF group, intravenous access was attempted in 16 047/38 175 (42.0%) and the success rate was 7334/16 047 (45.7%). After PS matching, 1802 patients of the VF group and 20 010 patients of the non-VF group were matched. Characteristics of the matched patients were presented in table 1A and 1B with successful matching. The area under the receiver operating characteristic curves of the logistic regression models (for the propensity of intravenous access attempt) was 0.81 for VF group and 0.82 for non-VF group.
Patient characteristics with initial rhythm of VF according to intravenous access attempt before and after PS matching
Patient characteristics with initial rhythm of non-VF according to intravenous access attempt after propensity score matching
Outcomes
Associations between intravenous route access, successful inttravenous route access placement, epinephrine administration and the favourable neurological outcome according to initially documented rhythms are shown in tables 2 and 3.
ORs for CPC 1 or 2 at 1 month before and after PS matching, and prehospital ROSC and 1-month survival for matched patients with initial rhythm of VF
OR for CPC 1 or 2 at 1 month before and after PS matching and prehospital ROSC and 1-month survival for matched patients with initial rhythm of non-VF
In the VF group (table 2), the intravenous route access attempt was negatively associated with 1-month survival with a favourable neurological outcome (OR 0.76, 95% CI 0.59 to 0.98). Even when the intravenous route access was successfully established and epinephrine was administered, the outcome was not improved (OR 0.87, 95% CI 0.65 to 1.15). Failure of intravenous route access was associated with worsening of the outcome (OR 0.61, 95% CI 0.42 to 0.87). In regards to the secondary outcomes, successful intravenous route access was associated with higher rate of prehospital ROSC (OR 1.29, 95% CI 1.01 to 1.65), and the failure of intravenous access had negative relation with achieving prehospital ROSC or survival at 1 month after cardiac arrest (OR 0.60, 95% CI 0.42 to 0.83; OR 0.64, 95% CI 0.48 to 0.86). In turn, epinephrine administration has not been proved to increase prehospital ROSC or 1-month survival (OR 1.32, 95% CI 0.98 to 1.76; OR 1.00, 95% CI 0.75 to 1.33) among the matched patients with an initial rhythm of VF.
In the non-VF group (table 3), intravenous access attempt, its success or failure were not found to have a favourable relationship with the outcome (OR 1.06, 95% CI 0.84 to 1.34, OR 1.17, 95% CI 0.89 to 1.54 and OR 0.91, 95% CI 0.66 to 1.25). However, when the intravenous route access was successfully established and epinephrine was administered, the outcome was improved (OR 1.52, 95% CI 1.08 to 2.08). The intravenous access attempt (OR 2.41, 95% CI 2.16 to 2.69; OR 1.19 95% CI 1.04 to 1.36), successful intravenous access (OR 3.91, 95% CI 3.49 to 4.38; OR 1.39, 95% CI 1.20 to 1.62) and epinephrine administration (OR 10.30, 95% CI 9.22 to 11.51; OR 2.81, 95% CI 1.84 to 2.58) were all positively related to achieve prehospital ROSC and 1-month survival.
Discussion
This study aimed to evaluate the effectiveness of prehospital intravenous access for survival with neurologically favourable outcomes among VF and non-VF OHCAs, considering the attempt and success of intravenous access by EMS personnel based on a large-scale prospective population-based OHCA registry. The success rate of intravenous access was low and intravenous access attempted among VF OHCA patients was negatively related to 1-month survival with favourable neurological outcome, even after a propensity score matching.
When EMS personnel administer epinephrine to the patients, the procedure includes three steps; intravenous access attempt, successfully securing intravenous route and epinephrine administration. The effectiveness of epinephrine administration during resuscitation should depend on the success rate of the intravenous route attempt and interruption of CPR, in addition to the epinephrine’s pharmacological effect. We performed an analysis of the association between an intravenous route access ‘attempt’ and patients' outcomes, reflecting a decision-making process in the real world and demonstrated low survival in the intravenous access attempted among VF patients, but high survival in those among the non-VF group receiving epinephrine administration. The low success rate of the intravenous route attempt in this study (46%) was almost the same as with a previous study.20 As it is difficult to provide advanced treatments with high-quality CPR especially in prehospital settings,1 we should discuss that advanced life support measures might not always help survival.
Intravenous access and epinephrine administration in OHCA (success rate, association with outcomes)
The effects of epinephrine administration on OHCA patients have been vigorously discussed for decades. A recent large randomised controlled trial (RCT) showed that patients with intravenous drug administration had no statistically significant improvement in survival to hospital discharge or 1-year survival.21 A large observational study from Japan that showed prehospital epinephrine had a negative association with favourable neurological outcomes at 1 month.10 On the other hand, Jacob’s RCT showed statistically significant improvement in the proportion of patients achieving prehospital ROSC, though failed to show statistically significant improvement in a survival to hospital discharge due to inadequate number of patient recruitment.22 Some observational studies from Japan have reported that early administration of epinephrine might be effective for both initially unshockable23 and shockable rhythms.24 In our matched population, none of the patients with initial unshockable rhythms received epinephrine early in the time course, so we could not evaluate the effectiveness of early epinephrine administration. IO access would realise a higher success rate and make more rapid drug infusion possible than intravenous access during cardiac arrest, as previously reported,25 and might yield some additional benefits from epinephrine administration.
When we investigate the role of epinephrine in real prehospital OHCA settings, we should consider the intravenous access attempt, success and use rate before epinephrine administration. A report from national data of all OHCAs in Japan showed an association between intravenous route access and the decreased likelihood of a favourable neurological outcome.26 It matched patients who received prehospital intravenous fluids with those who did not receive intravenous fluids. Considering that the success rate of intravenous access attempt is not so high in general, there might have been two different types of patients among those who did not receive intravenous fluids; those for whom an intravenous access had been attempted but failed and an intravenous access had never been attempted. We prospectively collected data on intravenous access attempts to address this issue and calculated the propensity of intravenous access attempts at the decision point of ELSTs in the real world.
There are two reasons for placing an intravenous access in resuscitation: the delivery of pharmacological therapy and volume loading. For the latter, a previous study of paediatric OHCA reported that intravenous or IO access attempts and fluid administration were associated with improved survival.27 However, few studies have demonstrated the advantage of prehospital intravenous access in adult patients. There might be several reasons why we could not find the beneficial effects of intravenous route attempts on neurological outcome. First, procedures related to intravenous access and epinephrine administration might have led to a decline in the quality of chest compressions such as compression fraction and depth, which are keys to survival after OHCA.1 Second, delayed scene time might impact patient outcomes. A few studies have reported that the scene time had an association with patients’ outcomes.27 28 In our study, we found a 4 min delay from emergency call to hospital arrival. While the clinical effectiveness of many prehospital advanced life support procedures has been controversial,21 29 30 the effectiveness of each procedure should be discussed in light of the sequence and time course of procedures.
Limitations
Several inherent limitations to our study must be noted. First, we did not obtain data on the skill level of ELSTs and the quality of CPR such as compression rate and depth, which could have influenced on the outcomes. Second, we did not collect data on the timing of the prehospital ROSC and intravenous attempt. We have excluded patients who responded to the first defibrillation, as these patients rarely receive intravenous attempt. However, this exclusion criterion partly adjusted comparability only among VF patients. In non-VF patients, we could not discriminate the patients who achieved ROSC in the very early timing of the CPR and did not have intravenous access attempted from those who did not achieve ROSC and did not have intravenous attempted for any reason. Third, our data did not include information on in-hospital advanced measures after hospital arrival. We could not address whether prehospital intravenous access contributed to treatment after hospital arrival such as early administration of medications or therapeutic hypothermia. Fourth, this study did not assign intravenous access attempts randomly. We performed propensity score matching to improve comparability, but could not control unmeasured or unknown confounding factors that may have influenced the results. Of note, EMS personnel in Japan are prohibited from terminating CPR at their own discretion, which could impose substantial bias on the interpretation of the result. Intravenous access could have been attempted only for those patients that EMS personnel and online MC personnel in charge judged as to be worth going forward with advanced procedures. Although we adjusted with available data, including bystander witness and MC, the results could be biased by unmeasured confounders, including the competency of providers, the quality of resuscitation attempts and prolonged downtime. Given that the effect sizes observed in the present study are relatively small, the results must be cautiously interpreted for their fragility. Fifth, our analyses were primarily intended to evaluate the effectiveness of intravenous access. As patients’ outcome could be strongly influenced by the epinephrine administration, we additionally analysed the effect of epinephrine administration. However, the results should be taken as exploratory considering that the PS model was constructed for intravenous access attempt, not for epinephrine administration. We have noticed that there is a high profile ongoing double-blind, randomised controlled study, Prehospital Assessment of the Role of Adrenaline: Measuring the Effectiveness of Drug administration In Cardiac arrest that investigates the clinical efficacy and cost-effectiveness of epinephrine administration for patients with OHCA.31 Gathering all the results from the RCT and observational studies would contribute in renewing the clinical practice guideline. Finally, this study was performed only in Osaka Prefecture in Japan. These results might not be applicable directly to other regions.
Conclusions
Intravenous access attempts could be negatively associated with 1-month survival with a favourable neurological outcome after OHCA. Subsequent epinephrine administration might be effective for initial non-VF OHCAs.
Acknowledgments
We are greatly indebted to all of the EMS personnel and concerned physicians in Osaka.
References
Footnotes
Contributors TI is the guarantor of the research. TF and TKi conceived the project. TF worked on the initial architecture for the study with methodological input from TKi. TI and TKa helped draft the article and revise it critically for important intellectual content. KKa, TN and YH worked on the data acquisition. KKi and CN worked on the data management. All authors gave final approval of the version to be published.
Funding This research received no specific grant from any funding agency in the public, commercial or not’for’profit sectors
Competing interests None declared.
Ethics approval Osaka University.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.