Article Text

Abstract
Introduction During brain tumour surgery, vasopressor drugs are commonly administered to increase mean arterial blood pressure with the aim of maintaining sufficient cerebral perfusion pressure. Studies of the commonly used vasopressors show that brain oxygen saturation is reduced after phenylephrine administration, but unaltered by ephedrine administration. These findings may be explained by different effects of phenylephrine and ephedrine on the cerebral microcirculation, in particular the capillary transit-time heterogeneity, which determines oxygen extraction efficacy. We hypothesised that phenylephrine is associated with an increase in capillary transit-time heterogeneity and a reduction in cerebral metabolic rate of oxygen compared with ephedrine. Using MRI and positron emission tomography (PET) as measurements in anaesthetised patients with brain tumours, this study will examine whether phenylephrine administration elevates capillary transit-time heterogeneity more than ephedrine, thereby reducing brain oxygenation.
Methods and analysis This is a double-blind, randomised clinical trial including 48 patients scheduled for surgical brain tumour removal. Prior to imaging and surgery, anaesthetised patients will be randomised to receive either phenylephrine or ephedrine infusion until mean arterial blood pressure increases to above 60 mm Hg or 20% above baseline. Twenty-four patients were allocated to MRI and another 24 patients to PET examination. MRI measurements include cerebral blood flow, capillary transit-time heterogeneity, cerebral blood volume, blood mean transit time, and calculated oxygen extraction fraction and cerebral metabolic rate of oxygen for negligible tissue oxygen extraction. PET measurements include cerebral metabolic rate of oxygen, cerebral blood flow and oxygen extraction fraction. Surgery is initiated after MRI/PET measurements and subdural intracranial pressure is measured.
Ethics and dissemination This study was approved by the Central Denmark Region Committee on Health Research Ethics (12 June 2015; 1-10-72-116-15). Results will be disseminated via peer-reviewed publication and presentation at international conferences.
Trial registration number NCT02713087; Pre-results. 2015-001359-60; Pre-results.
- phenylephrine
- ephedrine
- cerebral microcirculation
- brain oxygenation
- magnetic resonance imaging
- positron emission tomography
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- phenylephrine
- ephedrine
- cerebral microcirculation
- brain oxygenation
- magnetic resonance imaging
- positron emission tomography
Strengths and limitations of this study
Unique clinical trial design incorporating neuroimaging in the search for optimal vasopressors in anaesthetised patients undergoing craniotomy for cerebral tumours.
Comparing effects of vasopressors on cerebral blood flow parameters between the peritumourous area and the contralateral hemisphere.
Neuroimaging with MRI and positron emission tomography (PET) in a homogeneous group of patients to obtain the best measurements of cerebral blood flow, capillary transit-time heterogeneity, cerebral metabolic rate of oxygen and oxygen extraction fraction.
Small sample size due to difficult inclusion in a vulnerable group of patients and extensive study set-up.
Not possible to obtain simultaneous MRI and PET values; thus, the study is divided into two parts.
Introduction
Patients with brain tumours often have increased intracranial pressure (ICP)1 and impaired autoregulation,2 with potential to cause cerebral ischaemia during surgery.3 4 To ensure sufficient cerebral perfusion pressure (CPP), higher mean arterial blood pressure (MABP) values5 6 are often maintained with vasopressor therapy in patients undergoing craniotomy for brain tumours and other cerebral pathology.7
Phenylephrine and ephedrine are commonly used vasopressors during neurosurgical procedures.8 9 However, studies show that MABP correlates poorly with microcirculatory flow.10–12 Accordingly, elevation of blood pressure may, paradoxically, lead to reduced capillary perfusion and decreased oxygen delivery despite reaching endpoints with CPP within 50–70 mm Hg.10–12 This is supported by an experimental study demonstrating a vasopressor-inotrope-induced mismatch between cerebral perfusion and oxygenation, possibly due to microvascular heterogeneity.13 In addition, a number of studies demonstrate that cerebral tissue oxygen saturation (SctO2), as measured by near-infrared spectroscopy (NIRS), decreases after phenylephrine administration but remains unchanged after administration of ephedrine, although both agents cause MABP to increase in healthy anaesthetised subjects.9 14–18 In one study, the decrease in SctO2 was associated with an increase in cerebral artery blood flow velocity and possibly vasoconstriction.19 Thus, augmenting MABP and CPP with vasopressors may lead to a paradoxical microcirculatory response, including vasopressor-induced tissue hypoperfusion and poor tissue oxygenation. Except for one study reporting transcranial Doppler, cerebral blood flow (CBF) was not measured in the studies above, and it is therefore unclear whether the SctO2 changes were associated with changes in CBF.15
Brain microcirculation is the primary site of oxygen exchange. We have recently proposed that red blood cell capillary transit-time heterogeneity (CTH) may affect tissue oxygen tension in patients with ischaemic stroke, subarachnoid haemorrhage and traumatic brain injury.20–23
According to this theory, capillary constriction, or capillary compression due to oedema and elevated ICP, may cause redistribution of capillary flows into heterogeneous patterns with functional shunting of oxygenated blood through the capillary bed.20 This capillary dysfunction may further hinder oxygen diffusion into cerebral tissue and ultimately cause cerebral ischaemic damage. We therefore hypothesise that the diverging effects of phenylephrine and ephedrine on cerebral oxygenation may be the result of differential effects on either blood supply, as measured by CBF, or oxygen extraction efficacy (OEF), as derived from CTH.
Currently, there are no comparative studies available on the effects of commonly used vasopressors on brain microcirculation and oxygenation in patients with brain pathology. Using MRI and positron emission tomography (PET), this study aims to investigate whether phenylephrine, when compared with ephedrine, is associated with capillary flow disturbances, elevated CTH and reduced oxygen availability in anaesthetised patients with brain tumours.
Methods and analysis
Study design
The study is an investigator-initiated, interventional, prospective and randomised clinical trial. The setting for the trial is the Department of Neurosurgery and Neuroanesthesia, Aarhus University Hospital, Aarhus, Denmark. The trial is divided into two parts according to imaging method (see below). Trial reporting will be guided by the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines (see online supplementary file 1 and file 2 for the populated SPIRIT checklist and figure).
Supplementary file 1
Supplementary file 2
Patients
Forty-eight patients scheduled for intracranial tumour resection by craniotomy will be included in the study following written informed consent obtained by the primary investigator or coinvestigator.
Inclusion criteria
Patients who meet the following criteria will be included in the study: (1) patients who are scheduled for elective craniotomy for supratentorial malignant and non-malignant brain tumours 3 cm or larger (measured as the largest diameter in any plane on MRI), (2) patients with an American Society of Anesthesiologists status 1–3,24 and (3) patients aged between 18 and 75 years.
Exclusion criteria
Patients who meet any of the following criteria will be excluded from the study: (1) patients who are pregnant (positive pregnancy urine test) or nursing, (2) patients with a history of allergic reactions to phenylephrine or ephedrine, (3) patients with an extra glomerular filtration ratio (eGFR) <60 mL/min per 1.73 m2 and (4) and patients who are unable to give written informed consent.
Randomisation and blinding
Patients will be allocated to treatment groups based on a computer-generated random allocation sequence (http://www.randomization.com), using a 1:1 randomisation ratio. In parts 1 and 2 of the study, randomisation is performed in blocks of 10+10+4 patients to receive either phenylephrine or ephedrine. The allocation sequence refers an independent assistant to one of the consecutively numbered, opaque, sealed envelopes, which contains information about the vasopressor to be given (phenylephrine or ephedrine). On study inclusion, each patient receives the treatment assigned in a numbered envelope, which will be opened by dedicated study nurses just before anaesthesia. Syringes containing either ephedrine or phenylephrine are marked with a randomisation code known only to the study nurses.
Patients and investigators are blinded to the randomisation. Interpretation of MR/PET imaging and calculation of flow parameters are performed by a blinded investigator. After final inclusion, an independent assistant will unblind the two groups and subsequently label the groups 0 and 1. Statistical analysis will be performed and eventually final unblinding will take place.
Anaesthesia and monitoring
Anaesthesia is induced with propofol 0.7–1.5 mg/kg and remifentanil 0.3–0.6 mL/kg/h. A low dose of suxamethonium is administered in order to facilitate intubation. This is in order to reduce risk of severe hypotension after high induction doses of propofol and remifentanil. Non-depolarising relaxation is not used. It is important to emphasise that bispectral index (BIS) monitoring is used during induction to ensure adequate depth of anaesthesia.9 Propofol and remifentanil are administered to ensure immobility. The patients are ventilated with 50% oxygen in air by controlled ventilation with the goal of achieving partial pressure of carbon dioxide in arterial blood (PaCO2) and partial pressure of oxygen in arterial blood (PaO2) values between 30 and 40 mm Hg and greater than 100 mm Hg, respectively. PaCO2 is adjusted according to arterial blood gas measurement. Isotonic NaCl or Ringer’s lactate is infused at a rate of 3 mL/kg/hour. Temperature is monitored as soon as the patient arrives in the operating room—equipment for temperature measurement is not MRI-compatible. The patient is kept warm in the scanner with sheets and blankets; furthermore, the MRI increases temperature in the patient body during the scan. The patient is supine and neck rotation and compression cannot occur in our MRI head cradles.
ECG, oxygen saturation, heart rate and intra-arterial blood pressure are continuously monitored. Depth of anaesthesia is monitored with BIS. Brain oxygenation is monitored by NIRS before and after MRI, and during PET, to allow comparison of brain oxygenation measurements determined by PET and MRI, respectively. Subdural ICP is measured perioperatively after removal of the bone flap.25
Intervention and study drugs
Participants will receive an intravenous infusion of either ephedrine (2 mg/mL) or phenylephrine (0.1 mg/mL) until MABP increases to above 60 mm Hg, or by 20% relative to the baseline. Baseline MABP is defined as the first MABP measured at the time of the initial MRI or PET sequence. The infusion is terminated after the subdural ICP measurement. These infusion protocols were chosen to reflect clinical recommendations and aimed to maintain a stable blood pressure throughout the whole MRI and PET sequences.26 27 In case of unacceptable hypertension during infusion of study drug, it was considered to reduce or end infusion. In addition, if reflex bradycardia occurs we consider to reduce study drug infusion rate or administration of atropine.
Experimental MRI and PET protocol
The experimental protocol is shown in figure 1. For logistical reasons, and to avoid long duration of anaesthesia, we choose not to perform consecutive MRI and PET on the same patient. Instead the protocol consists of two parts, according to imaging method.
Part 1 (MRI study): 24 patients are randomised to infusion of either ephedrine or phenylephrine and imaged by MRI after induction of anaesthesia.14
Part 2 (PET study): 24 patients are randomised to infusion of either ephedrine or phenylephrine and imaged by PET after induction of anaesthesia.14
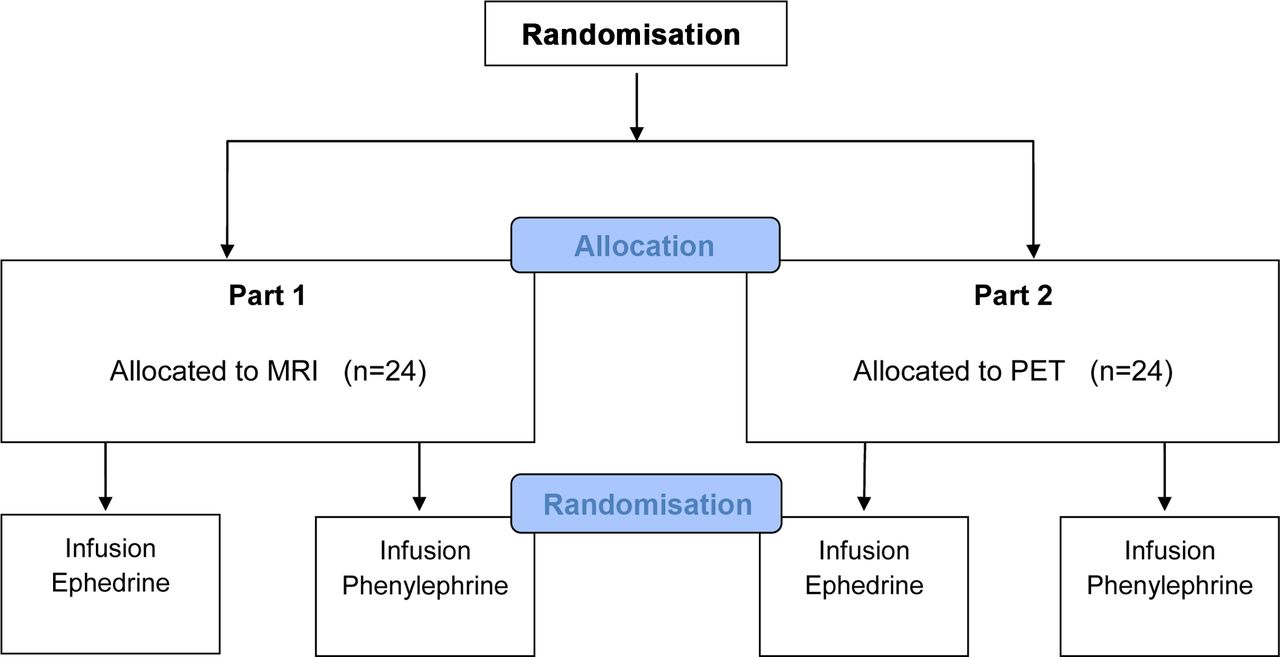
Study flow chart. PET, positron emission tomography.
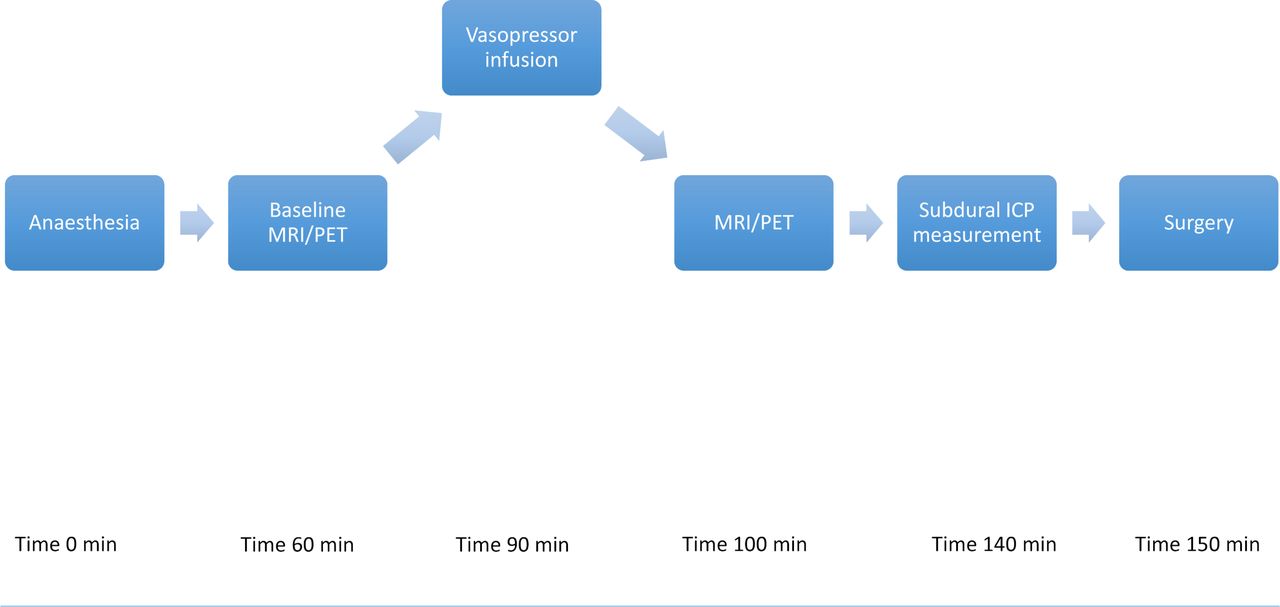
The overall experimental set-up is the same for the two parts of the study. The patient is anaesthetised in a room adjacent to the MRI or PET scanner. MRI and PET examinations are performed before and after administration of the study drug. The study period is shown in figure 2. The specific MRI and PET protocols are described below.
{kind=link}
{kind=link}
Time sequence diagram. Anaesthesia induced at time 0 min. During the first hour baseline MRI/positron emission tomography (PET) is performed (time approximately 60 min). Vasopressor infusion of either phenylephrine or ephedrine is initiated until mean arterial blood pressure (MABP) increases to above 60 mm Hg, or by 20% relative to the baseline. A 5 min steady-state period of MABP is maintained before the second MRI/PET examination is performed (time approximately 100 min). The patient is transported to the operating room. Surgery is initiated, and after removal of the bone flap subdural intracranial pressure (ICP) is measured (time approximately 140 min). Subsequently the study period is terminated and surgery continues (time approximately 150 min).
MRI protocol
The protocol consists of the following: (1) conventional MRI sequences to depict brain anatomy and structural changes, (2) diffusion-weighted MRI including diffusion kurtosis imaging to infer tissue microstructure,28 and (3) perfusion-weighted MRI to infer cerebral haemodynamics. The duration of the entire MRI scan is estimated at 60 min, and 0.25 mmol/kg macrocyclic gadolinium MRI contrast is administered, corresponding to 2.5 standard doses.
PET protocol
The protocol consists of the following: (1) CBF: 500 MBq of [15O] H2O is injected intravenously. On injection, a 5 min PET image acquisition of the brain is started together with arterial blood sampling (also 5 min) with an automated blood radioactivity sampler that draws 7 mL blood per minute. The PET acquisition is performed on a Siemens High Resolution Research Tomograph in list mode. (2) Cerebral metabolic rate of oxygen (CMRO2): 1000 MBq of [15O] O2 is inhaled and immediately exhaled. On inhalation, a 3 min PET acquisition and blood sampling are performed with protocols identical to that of the CBF measurement. (3) During each scan session, oxygen saturation and haemoglobin concentration will be measured.
Endpoints
Primary endpoint
Between-groups difference in CTH measured with MRI.
Secondary endpoints
Between-groups absolute and relative differences in cerebral blood flow (CBF), cerebral blood volume (CBV), mean transit time (MTT); calculated and measured CMRO2 and OEF, respectively.
Between-groups absolute and relative difference in MABP, arterial oxygen saturation, BIS, NIRS and subdural ICP.
Data management
All MRI and PET data are stored on a server with secured and restricted access. BIS and NIRS data are stored on an encrypted personal computer with limited access. Physiological data are recorded in a case report form (CRF). All CRFs are stored in a secure and locked area at the Department of Neuroanesthesia. Subsequently, all data are entered into a password-protected study database with secured and restricted access. Data are kept confidential.
Analysis of imaging data
MRI data
Perfusion-weighted and diffusion-weighted data are analysed as described previously.28–30
Colour-coded maps of CBF, CTH, the calculated CMRO2 and OEF for negligible tissue oxygen tension, and CBV are generated along with grey-scale apparent diffusion coefficient, and diffusion kurtosis maps are created. Regions of interests in the perilesional oedema, the contralateral normal-appearing white and grey matter, are defined on T1-weighted MRI sequences and subsequently coregistered to the perfusion and diffusion maps. Mean values in the regions of interests are calculated and correlated to the physiological parameters.
PET data
MP2RAGE will be acquired for each subject for PET coregistration. All PET images will be reconstructed with a 3D-ordered subset expectation maximization point spread function (3D-OSEM PSF) algorithm with a final isometric resolution of 2–3 mm and divided into time frames (twelve 5 s frames, six 10 s frames, and three 20 s frames for CMRO2, and 36 5 s frames, six 10 s frames, and three 20 s frames for CBF).
Parametric maps
Voxel-wise parametric estimation of CBF and CMRO2 will be performed by using arterial blood radioactivity as input function and a one-tissue-compartment model based on the works of Ohta et al and Blomqvist.31–33
Oxygen extraction fraction is calculated by the formula OEF = CMRO2/ (CBF · CaO2), where CaO2 is the arterial content of oxygen (haemoglobin concentration · oxygen saturation).
Statistics
Sample size estimation was calculated with a power analysis in Stata V.14 on a basis of earlier pilot studies with calculations of CTH, a significance level of 0.05 and a power of 0.9 (β=0.1). A 10% difference in CTH was defined as a significant clinical change. In addition, a 10% difference between phenylephrine and ephedrine in cerebral oxygenation measured with NIRS was recently found clinically significant.9 16 No data exist on vasopressor therapy with CTH as the primary endpoint. Consequently, based on our current experience with CTH, the expected 10% difference in CTH was translated into an estimated prevasopressor MRI-CTH value of 3.216 s and a 10% difference, giving a mean difference of 0.3216 s (∆phenylephrine ÷ ∆ephedrine ≥10%). In both study parts a sample size of nine patients in each randomisation arm will be required. To compensate for potential dropouts and missing data, the sample size was increased by 25% to a total of 24 patients in each study part.
All data are expressed and displayed as mean and SD unless otherwise stated. The hypothesis is two-sided. Data will be analysed using conventional appropriate test statistics depending on the distribution of the individual outcome parameters. Specific tests include paired t-test or Wilcoxon signed-rank test for paired data analysis and unpaired t-test or Mann-Whitney U test for testing of between-group differences. Standard parametric or non-parametric statistical tests will be used according to the Gaussian distribution to compare MRI, PET and physiological parameters. P values of less than 0.05 are considered statistically significant.
Study management
The study will be conducted in accordance with the guidelines and rules concerning quality control and quality management on clinical trials involving humans, and will follow the Good Clinical Practice and the Good Manufacturing Practice guidelines. All data regarding potential and enrolled participants will be treated confidentially. Only the investigators and relevant authorities will have access to the data. Amendments to the protocol will be communicated to the relevant authorities and the entries on the registry databases will be updated. Results will be disseminated via peer-reviewed publication and presentation at international conferences; additional summaries will be provided to patients.
Ethics approval and consent to participate
The study procedure, benefits, risks and data management will be introduced in detail to all eligible participants before they give written informed consent. Any incidents or adverse reaction will be treated immediately also postoperatively in the recovery room by the sponsor or coinvestigators, and the patient will be unblinded. Serious adverse events (SAE) or serious unexpected suspected adverse reaction (SUSAR) perioperatively or postoperatively will be recorded and reported to the Danish Health Protection Agency and the Regional Committee on Health Research and Ethics. Any deadly or life-threatening SAE that is both unexpected and suspected to be related to treatment (SUSARs) will be collected and reported to the competent authorities and relevant ethics committees in accordance with Directive 2001/20/EC, and as per national regulatory requirements as soon as possible and no later than 7 days after investigator of such an event has provided relevant knowledge. Subsequently, relevant follow-up information is to be communicated within 15 days.
Discussion
In this study, we hypothesise that cerebral CTH is increased and brain oxygenation therefore reduced compared with resting CMRO2 during infusion of phenylephrine in clinically relevant doses. The study-drug dosage regimen used in this study is in contrast to other studies in which phenylephrine and ephedrine were administered as bolus doses.9 14 15 In order to secure a constant exposure to the study drug and thus stable haemodynamics during the MRI and PET examinations, we found it necessary to use an infusion regimen. However, the effects on brain haemodynamics and oxygenation may be different whether the vasopressor agent is administered as a bolus dose or an infusion. For example, the gradual increase in MABP during the infusion may not elicit the same change in CTH and CBF as a bolus injection, which might elicit an autoregulatory response.9 There are methodological limitations; due to logistical and ethical considerations, we opted not to perform both MRI and PET examinations on the same subjects, although this would clearly be desirable. Accordingly, the study is divided into two different parts where patients are subjected to either MRI or PET. In addition, it is not possible to obtain simultaneous NIRS measurements during the MRI examinations due to the ferromagnetic nature of the NIRS electrode.
The study may lead to an improved understanding of the effects of commonly used vasopressors on CBF-related parameters and brain oxygenation in patients with brain pathology. The results from this study may have the potential to guide the anaesthesiologists in choosing the optimal vasopressor agent for neurosurgical procedures, which may influence surgical outcome
Trial status
The study is including patients during a period from September 2015 until December 2017.
Acknowledgments
The authors would like to thank the nurses at the Department of Neuroanesthesia, Aarhus University Hospital, and the staff at the Center of Functionally Integrative Neuroscience, Aarhus University. We would like to thank all the participating patients for their time and effort. We also thank the following people: Irene Klærke Mikkelsen (MSc, PhD), Torben Lund (Associate Professor, PhD), Dora Ziedler (neuroradiologist), Michael Geneser (neuroradiologist) and Kim Mouridsen (statistician) at Aarhus University Hospital/Aarhus University.
References
Footnotes
Contributors KUK, AT, JA and MR made substantial contribution to the conception and design of this study. KUK drafted the manuscript, with input from AT, JA, MR and LN. LN, JCHS and LØ were senior supervisors. GvO and NJ contributed to conduction of the clinical studies. KUK is the chief investigator and has the overall responsibility for the study. All authors participated in the preparation of, and approved for publication, the final manuscript.
Funding This work was supported by funding from Lundbeckfonden (ref R164-2013-15390), Toyota Fonden (ref KJ/BG 8864 F) and the AP Moeller Foundation for the Advancement of Medical Science (ref 1718/NK PhD Vasobrain), Denmark. The study received institutional support from the Center of Functionally Integrative Neuroscience at Aarhus University and the Department of Neuroanesthesia at Aarhus University Hospital.
Competing interests None declared.
Ethics approval The study has been reported to the local GCP Unit, which is monitoring the trial. The study was approved by the Central Denmark Region Committee on Health Research Ethics (12 June 2015; 1-10-72-116-15). The trial has been approved by the Danish Health and Medicines Authority (16 June 2015, 2015042707) and the data monitoring committee Danish Data Protection Agency (2 July 2015, 1-16-02-291-15) independent from sponsor and without competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.