Article Text

Abstract
Objectives To identify the approaches that are used in improving on male partner involvement in the prevention of mother-to-child transmission (PMTCT) of HIV and their impact on the uptake maternal antiretroviral therapy (ART) in sub-Saharan Africa (SSA).
Setting This was a systematic review and meta-analysis of published studies carried out in SSA at all levels of healthcare (primary, secondary, tertiary and community).
Participants The participants of the studies included were HIV-positive pregnant women and breastfeeding mothers with their male partners. Studies were included if they were conducted in SSA and mentioned an approach used in improving male partner involvement with data on the impact on the uptake of maternal ART uptake.
Outcomes In the protocol, maternal ART uptake, infant prophylaxis, safe infant feeding options, condom use and family planning were envisaged. However, only maternal ART has been reported here due to limitations on the word count.
Results From an initial 2316 non-duplicate articles, 17 articles were included in the systematic review and meta-analysis. In the combined model, the ORs for complex community interventions, enhanced psychosocial interventions, verbal encouragement and invitation letters were 4.22 (95% CI 2.27 to 7.77), 2.29 (95% CI 1.42 to 7.69), 2.39 (95% CI 1.26 to 4.53) and 1.21 (95% CI 0.89 to 1.63), respectively, whereas in the model using adjusted ORs, enhanced psychosocial interventions had a higher effect than any other intervention. The heterogeneity was moderate using adjusted ORs.
Conclusion Enhanced psychosocial interventions and complex community interventions increase male partner involvement and the uptake of PMTCT services more than any other intervention. Invitation letters had no effect. More randomised trials and observational studies (that have adjusted for potential confounders) are needed in the future.
PROSPERO registration number 42016032673.
- international health services
- public health
- health policy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The randomised controlled trials included in the study were prone to observer bias since there was no blinding done, but due to the nature of the studies, blinding was not feasible because it was essential for the investigators to have a knowledge of the couples in order to better tailor the interventions.
Even though only 7 studies out of 17 adjusted for confounders, the authors of the studies included reduced confounding by matching.
The heterogeneity was high among studies suggesting that the studies were not similar and could not be combined in a meta-analysis, but separate meta-analyses using only adjusted ORs showed moderate heterogeneity.
The independent search and screening of articles by two reviewers reduced bias.
The search was comprehensive because several databases and grey literature were searched, and authors were contacted for any unpublished studies.
Introduction
Rationale
Prevention of mother-to-child transmission (PMTCT) of HIV activities is implemented in programmatic settings through interventions which include: HIV counselling and testing, antiretroviral therapy (ART), condom use, infant prophylaxis, safe infant feeding and hospital delivery. In the absence of these interventions, the rate of transmission from mother to child is between 15% and 45% but with highly active ART during pregnancy and breast feeding, the risk can be reduced to below 1%.1 These interventions have been scaled up in the sub-Saharan Africa (SSA) region and have prevented the transmission of HIV to some 670 000 infants.2 Currently, there is an optimistic goal to eliminate of mother-to-child transmission of HIV in SSA by 2030.3 Despite these successes, a major challenge which may slow down the progress towards the elimination of mother-to-child transmission of HIV is the low level of male partner involvement.
In the literature, there is no standard definition of male partner involvement in the PMTCT of HIV.4 It is also challenging to measure male involvement in a way that can encompass the practical assistance given by men to women and the various ways in which the men may overcome the gender norms in providing support to women.5 Despite this challenge, some authors have suggested some indicators for male partner involvement such as communication between spouses (including HIV status disclosure), antenatal care attendance and childbirth, antenatal testing and couple antiretroviral treatment and antenatal support during pregnancy.4 These indicators have been put together in a composite score or index in some studies in an attempt to broadly capture the notion of male involvement.4 6 7
The findings from studies on male partner involvement suggest that the low level of male partner involvement in SSA is seen by pregnant women as a sign of disapproval and may deter them from taking up PMTCT services.8 9 Baiden et al carried out a cross-sectional study to explore the determinants of the willingness of pregnant women in a rural district in Ghana to be tested for HIV.8 This study showed that women who demonstrated a strong sense of willingness to be accompanied by their male partners were five times more likely to accept HIV testing during antenatal care (OR 5.2; 95% CI 1.4 to 19.8). Even though this study was a cross-sectional study which limits the establishment of any temporal relationship, Kiarie et al in a randomised controlled trial (RCT) showed that compliance to antiretroviral regimens in pregnancy was strongly associated with partner notification (OR 7.5; 95% CI 1.4 to 40).10 Despite the current evidence supporting the positive influence of male partners from current studies, Becker et al in an RCT had reported that the use of invitation letters to involve male partners in PMTCT paradoxically resulted in lower uptake of antenatal services by pregnant women.11
The findings from a systematic review by Brusamento et al in 2010 suggested that male partner involvement had a negative impact on the uptake of PMTCT services by women.12 Despite the robust search strategy, the authors ended up with only a single study. The single study finding was likely because most of the studies supporting the positive impact of male partner involvement were published after 2010, which was clearly after the end of the search conducted by Brusamento and colleagues. In view of this contrasting evidence, it was necessary to conduct an up-to-date systematic review with meta-analysis to determine the approaches used in improving on male partner involvement in a PMTCT of HIV activity such as maternal ART uptake by HIV-seropositive pregnant women in SSA and to determine the impact of these approaches on the uptake of maternal ART by HIV-seropositive pregnant women in SSA.
Methodology
Protocol and registration
This systematic review with meta-analysis was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement of 2015. The protocol for this systematic review was registered in the International Prospective Register of Systematic Reviews. The registration number is CRD42016032673. The protocol was published in the British Medical Journal Open.13 The method described in this study is in accordance with the published protocol, but only maternal ART was reported here due to its higher relevance compared with the other outcomes with respect to the PMTCT of HIV.2
Eligibility criteria
This review considered studies that were conducted in SSA. Studies out of the SSA were excluded. No restriction was placed on the setting of the study and the language of study. RCTs, prospective and retrospective cohort studies and serial cross-sectional studies were included. The studies were included if they provided data on the impact of male partner involvement on maternal ART. One time cross-sectional studies and case–control studies were excluded because they did not present any evidence of the impact of male partner involvement. The participants were HIV-positive pregnant women or HIV-positive breastfeeding mothers with their partners.
Information sources and search strategy
A literature search was carried out from 1 December 2015 to 31 March 2016. A search strategy was developed by the principal investigator (NFT) with inputs from ITRK and CJ using evidence from a US Centre for Disease Control and Prevention study on how to carry out a detailed systematic search in HIV prevention.14 This search was later refined with the help of the University of Glasgow librarians. Six main databases were searched: Ovid MEDLINE, Ovid Embase, Ovid Health and Psychosocial Instruments, PsycINFO, Web of Science and Cochrane library. Current Controlled Trials and ClinicalTrials.gov were searched for ongoing and newly completed trials. A detailed search strategy is shown in online supplementary table 1. The search was conducted by NFT and CJ independently, and any disagreement was settled by a round table discussion between the two authors using the inclusion and exclusion criteria, until a consensus was achieved. A final search was conducted on 31 December 2016 to ensure that any new relevant articles were not missed.
Supplementary file 1
The outputs of the search were exported to Mendeley desktop V.1.16.1, and duplicates were removed. After removal of duplicates in Mendeley, the titles and abstracts of the studies were screened independently by NFT and CJ. The full texts were obtained from the screened abstracts after inclusion and exclusion criteria were applied. If the article was unavailable through the usual online search, the article reach system of the University of Glasgow interlibrary loan system or the British library was used to obtain the articles. Authors of articles were contacted for further information on any publication.
Data collection process and data items
A data extraction spreadsheet was developed in Excel version 2013. The data extraction sheet captured characteristics of the studies such as: authors, country of study, objectives of the study, study design/method, study setting, population, sample size, approaches/intervention used for PMTCT improvement and ORs.
The outcome of interest was maternal ART uptake. Maternal ART uptake was defined as the proportion of women who started ART as measured by self-reporting or medical records. ORs were extracted from individual studies. Relative risks and proportions were converted to ORs. Two reviewers independently extracted these data from the included studies. The proportions and relative risks were converted into ORs, noting the effect size and the 95% CI. The characteristics of included studies were summarised in table 1.
Characteristics of included studies
Synthesis of results and data analysis
The studies that were relevant after inclusion and exclusion criteria were applied were used in the synthesis. Studies with data on impact of male involvement on PMTCT services were considered for a meta-analysis that was performed using statistical software STATA V.11.0. In this review, the studies included varied significantly in terms of approaches and outcomes which suggest that the true effect sizes measured could also differ. This disparities could very likely introduce high heterogeneity. Therefore, the random effect model was used to pool the evidence from the studies. An overall forest plot was produced that combined unadjusted and adjusted ORs (extracted or calculated from included studies) in a single model. Separate forest plots were later produced for adjusted ORs. In terms of the adjusted model, we did not carry out any adjustment in the model. Instead, we used adjusted ORs that were extracted from the studies. In these studies, the authors adjusted mainly for maternal age and distance from the health facilities.
Heterogeneity was assessed using the I2 statistic generated. Heterogeneity refers to the variation between the included studies, and it was assessed as follows: if the I2=25%–49%, we considered a ‘low’ heterogeneity; if the I2=50%–74%, we considered a ‘moderate’ heterogeneity and if the I2 ≥75%, we considered a ‘high’ heterogeneity.15 Metaregression was used in exploring the reasons for heterogeneity between studies. Variables included in the regression were: the subregion of the study (grouped as Southern Africa, East Africa and West Africa), the study design (randomised and non-randomised), the study setting (urban, rural or mixed), the sample size, the category of male involvement approach used and the method of measurement of outcome. Publication bias was assessed using the funnel plot and the Egger’s test.
Results
The electronic search on Ovid MEDLINE, Ovid Embase, Ovid Health and Psychosocial Instruments, Web of Science, Cochrane library, and ClinicalTrials.gov. Current controlled trials returned 3460 results and after removal of duplicates, this reduced to 2316 results. The study selection process is shown on the PRISMA flow diagram in figure 1.
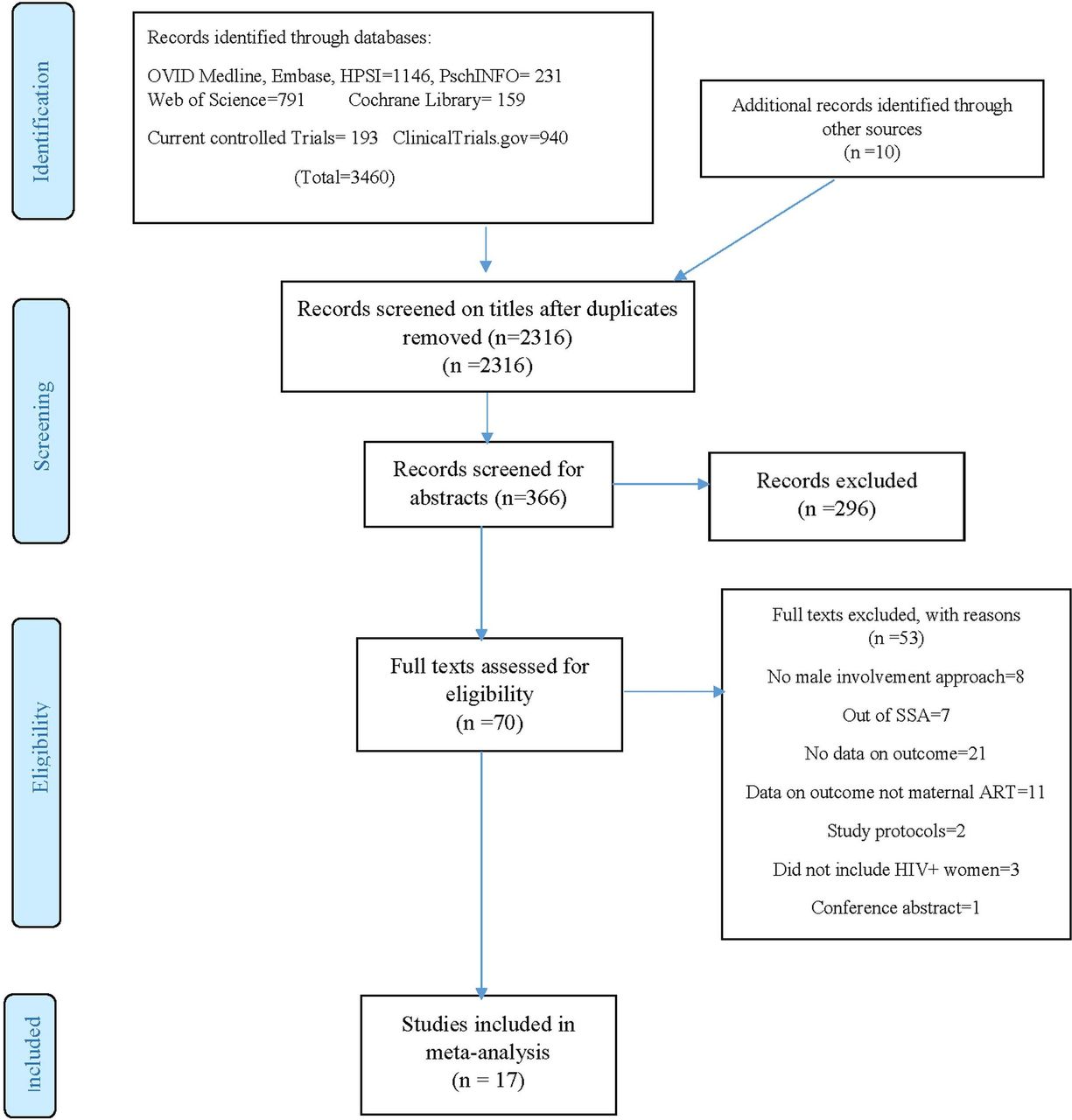
The PRISMA flow diagram showing selection of studies. ART, antiretroviral therapy; HPSI, Ovid Health and Psychosocial Instruments; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SSA, sub-Saharan Africa.
Seventeen studies were finally included in the systematic review and meta-analysis. Of this 17 studies, 4 were randomised trials, whereas 13 were observational studies.
Characteristics of included studies
The study population of participants from the RCTs included a total of 550 participants, all of which were HIV-positive pregnant women. The number of HIV-positive participants from the randomised trials ranged from 24 to 369. The observational studies included a total of 11 780 HIV-positive pregnant women and breastfeeding mothers. The number of participants ranged from 145 to 2141. In all of the studies, the outcome measured as the proportion of women who started ART. In 10 of the studies, the proportion of women who started ART was obtained from medical records, whereas in 6 studies, the proportion was obtained by self-reporting. The method of measurement of the proportion of women who started ART was not clearly stated in one study.
In three of the included studies (two RCTs and one observational), the investigators used invitation letters in order to improve the involvement of male partners in PMTCT.11 18 19 The two main types of invitation letters used were the ‘official invitation letter’ and ‘unofficial invitation letter’. The letters were considered official if they were signed by the head of the health facilities. However, even though the official letters were signed by the heads of the health facilities, no effort was made by these heads to confirm if the letters were handed to the male partners by the women.
In two of the studies (one RCT and one observational), the authors (Farquhar et al and Weiss et al) used psychological interventions that can be considered to be enhanced because they were conducted by trained personnel.20 21 Trained HIV-positive personnel were used by Farquhar and colleagues, whereas Weiss et al used the Partner Plus intervention in which trained HIV facilitators were gender-matched to conduct cognitive and behavioural skill training. Weekly sessions were conducted for 90–120 min addressing issues of HIV counselling and behaviour. In the Partner Plus intervention, participants attended four successive sessions which were gender-concordant and limited to 10 participants. In each group of 10 participants, there was the establishment of a safe environment for exchange of interpersonal experiences, role playing negotiations, problem solving and communications. Participants were given ‘homework’ to work as a couple at home and in the subsequent weeks, they were encouraged to share their experiences during the sessions and to apply behavioural skills in solving them.
In six studies (all observational), pregnant women were encouraged verbally through counselling to bring their partners for antenatal clinic. Aluisio et al, Msuya et al, Kalembo et al and Peltzer et al gave no description of the verbal message given to the pregnant women or the personnel responsible to pass across the message,22–25 whereas Spangler et al actively encouraged women through counselling to engage their male partners by disclosing their HIV status to them.26
In six of the included studies (one RCT and five observational), the investigators used complex community interventions in which several approaches to involve male partners were coupled with other changes in healthcare delivery to improve on maternal and child care within the community.27–32 Aliyu et al and Audet et al used male champions who were considered to be role models in the community.27 28 The male champions were involved in visiting the HIV-positive pregnant women and their male partners, encouraging them on PMTCT and advising the male partner on the need to support the women in taking up PMTCT services. Herce et al and Semrau et al carried out community mobilisation talks and dramas.30 31 In the Semrau et al study, there was engagement with community health workers to carry out mobilisation talks and dramas in football events, market places, clubs, churches and work places. In the study by Bannink-Mbazzi et al, health education materials were distributed in the communities, and community education was carried through radio programmes,29 whereas Byamugisha et al focused only on the family with no public event organised in the community.32 In the Byamugisha et al study, household couple support was given by community health workers in the form of education and guidance on the relevance of male involvement in PMTCT. The large sample size of the studies that used complex community interventions meant that they had high statistical power.
Quality assessment
Using the Jadad Scale, the randomised trials had a moderate risk of bias, whereas the observational studies had from moderate to low risk of bias using the Newcastle Ottawa Scale. The online supplementary figures 1 and 2 show the results of the quality assessment.
Results of meta-analysis and metaregression
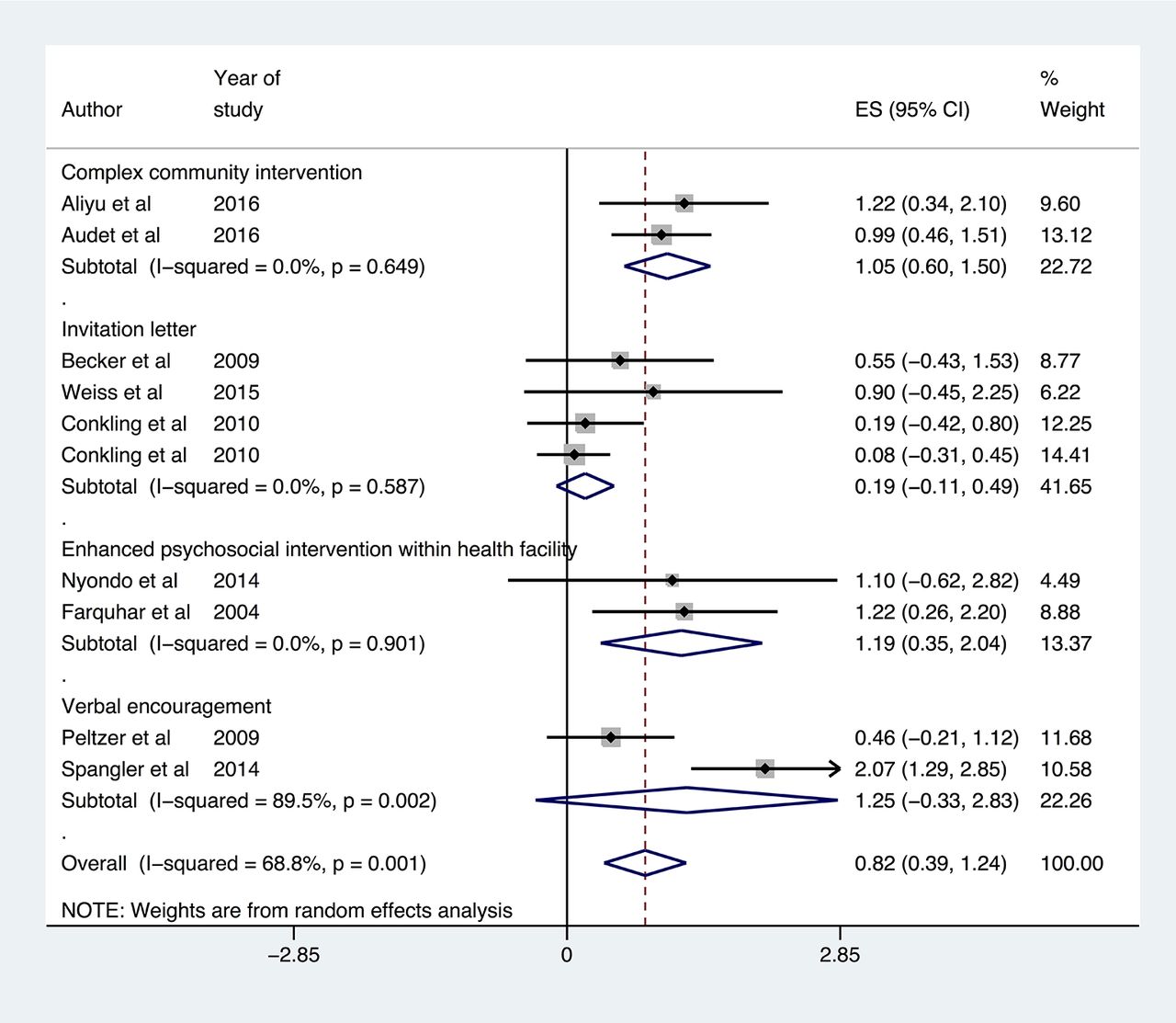
Figure 2 shows the overall forest plot of the unadjusted ORs and adjusted ORs for the studies that reported the impact of male involvement on the uptake of maternal ART. The effect sizes are reported as log ORs. The pooled estimate of the log ORs given by the blue diamond at the bottom is 1.02 with a 95% CI of 0.59 to 1.44. Exponentiating the log ORs gives the pooled unadjusted OR and 95% CI of 2.77 (1.80 to 4.22). Figure 3 shows the results of the subgroup analysis of each category of intervention. From this figure, the ORs for complex community interventions, enhanced psychosocial interventions, verbal encouragement and invitation letters were 4.22 (95% CI 2.27 to 7.77), 2.29 (95% CI 1.42 to 7.69), 2.39 (95% CI 1.26 to 4.53) and 1.21 (95% CI 0.89 to 1.63), respectively. However, in the model using adjusted ORs shown in figure 4, enhanced psychosocial interventions had a higher effect than any other intervention.

The overall forest plot showing the pooled estimate (in log ORs) of the impact of male involvement approaches on the uptake of maternal ART. ART, antiretroviral therapy; ES, effect size.

Stratified forest plot showing impact of individual male involvement approaches. ES, effect size.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Stratified forest plot of adjusted ORs showing impact of individual male involvement approaches. ES, effect size.
In the overall model in figure 2, the heterogeneity was high (I2=92.2%, P<0.001), whereas using only adjusted ORs as shown in the online supplementary figure 3, the heterogeneity was moderate (I2=68.8%, P<0.001). Online supplementary table 2 shows the results of metaregression of the studies to explore the sources of heterogeneity. The heterogeneity was completely explained by variation in the sample size of the studies (R2=100%).
The funnel plot in online supplementary figure 4 shows very little evidence of asymmetry since the points are randomly scattered throughout the plot. This suggests little or no evidence of publication bias for the studies that report the impact on maternal ART.
Discussion
A meta-analysis of 17 ORs from 17 studies showed a statistically significant increase in the uptake of maternal ART with male partner involvement. In the combined model, complex community interventions had a higher effect than any other approach, whereas in the adjusted model, enhanced psychosocial interventions have a higher effect. Invitation letters had no effect on the uptake of maternal ART in the combined model. The findings from this systematic review are similar to previous studies carried out in the area of male partner involvement in PMTCT. In a narrative review, Auvinen et al identified three main strategies to involve male partners in PMTCT which include: strategies that focus on the resources of the couples, strategies that focus on the development of healthcare and community strategies.33 Our study also similarly identified complex community strategies that encompass all the three strategies identified by Auvinen et al. However, we identified three additional approaches not mentioned in the Auvinen et al study which include: invitation letters, verbal encouragement and enhanced psychosocial interventions. It should be noted that the study by Auvinen et al was a narrative review with no systematic search strategy, no multiple database search and no independent assessment of the quality of included studies. These limitations may explain why the current systematic review identified additional studies with other relevant approaches. In addition, the narrative review could not provide data on the impact of male involvement on the uptake of PMCT services.
We found only one previous systematic review that had as objective to determine the impact of male partner involvement on the uptake of PMTCT services.12 In this systematic review, Brusamento et al thoroughly searched multiple databases with a comprehensive and systematic search strategy, independently assessed the quality of studies, but ended up with a single non-blinded RCT that met the inclusion criteria. The search strategy was biased towards identifying only randomised trials which could explain why the authors missed out relevant observational studies that could have improved on the evidence synthesis with possible meta-analysis. From this single study retrieved by the authors, the findings suggested that promoting male partner involvement in PMTCT through the use of invitation letters had no effect on the uptake of services such as maternal ART and infant prophylaxis. This finding by Brusamento et al is in agreement with our finding that invitation letters had no impact on maternal ART. However, since we pooled the evidence from as many as 17 studies in our study, other interventions were identified such as enhanced psychosocial and complex community interventions that were shown to be significantly associated with an increase in the uptake of maternal ART and infant prophylaxis.
On critical analysis of the studies that reported the use of invitation letters, it was noted that the authors did not confirm if the women actually gave the letters to their male partners. This could have partially accounted for the low response rate observed in the studies leading to selection bias. Furthermore, even though carrying out a formative research played an important role in guiding the content of the invitation letters in order to promote acceptability by the male partners, it was important to ensure that the women who participated in this formative phase were excluded in the actual study to avoid selection bias since it was likely that they could have been more prepared to participate, more educated about the study than the average woman in the settings. However, in the analysis, since it was difficult to confirm if the women actually gave the letters to their partners or not, the authors used intention to treat analysis which did not take into consideration the withdrawal or loss to follow-up.34
The findings from this study suggest that complex community interventions had a higher effect than any other intervention, whereas invitation letters had no effect. This was likely due to more engagement. By involving communities, the authors went closer to the male partner than in other approaches mentioned so far. This could reduce the chances of measurement errors observed in other approaches that relied in report from the pregnant women. Also, using several approaches within the community meant that the authors were likely to have explored diverse sociocultural context of these communities which could have accounted for more engagement with the male partners as compared with other categories of approaches used.35 However, it is very difficult to attribute the effect observed to any single type of community intervention mentioned within the complex intervention category. This is because the authors did not stratify the individual interventions and their effects.
Our analysis also shows that enhanced psychosocial interventions are associated with an improvement in the uptake of maternal ART. These either involved the use of HIV-positive peer counsellors or the use of the Partner Plus intervention in which trained facilitators were gender-matched to carry out cognitive and behavioural skill training. There are some advantages that can be associated with this interventions that may explain the observed effect. First, the use of HIV-infected peer counsellors could encourage HIV-infected couples to easily accept their status. Using well-trained peer counsellors ensured that they were well-equipped with communication skills that could improve on the level of male partner involvement.36 In addition, allowing the couples to choose the gender of the counsellor improved on the acceptance for counselling. Second, the use of the Partner Plus intervention involving well-advanced behavioural techniques may not only improve on male partner involvement in counselling and testing for HIV but also impact on their subsequent lifelong behavioural adaptations that can improve on the mental well-being of the couples.37 Despite these advantages, it should be noted that identifying HIV-infected peer counsellors could be challenging in many communities in SSA where stigma and fear of status disclosure still form a major component of the social context. Furthermore, given that the training skills of all the facilitators may not be uniform, the educational level and skill of the trainer could have confounded the observed impact on male partner involvement and uptake of PMTCT services by the couples.
This systematic review and meta-analysis had several strengths and some limitations. The search was comprehensive because several databases and grey literature were searched and authors were contacted for any unpublished studies. There was also independent search and screening of articles by two reviewers which reduced bias. Since the search ended in March 2016, new articles published between this time and the submission of the manuscript could affect the findings. However, a final search was conducted on 31 December 2016, and no new articles relevant to our outcomes of interest were retrieved. Unlike other systematic reviews on male partner involvement, the quality of studies included in our review was critically assessed. This assessment showed that the RCTs were prone to observer bias since there was no blinding. Despite this weakness, blinding was not feasible because a knowledge of the couples was essential in guiding the interventions. In the studies included for the systematic review, only seven observational studies adjusted for confounders. However, for randomised trials, the randomisation reduced the selection bias significantly, whereas the confounding was reduced by matching. In this review, a combined model was used to pool the adjusted and unadjusted ORs. The heterogeneity was therefore high among studies suggesting that the studies were not similar and could not be combined in a meta-analysis. However, separate meta-analyses using only adjusted ORs showed moderate heterogeneity. In terms of the public health and research significance, the study represents the first meta-analysis of male partner involvement in PMTCT of HIV in SSA, and it implements a prospectively published protocol for reviewing this growing body of literature. The findings from this study provide essential information on the approaches that can help in achieving the second United Nations Programme on HIV/AIDS (UNAIDS) ‘90’ target by increasing the uptake of ART by pregnant women through engagement of their male partners. Finally, the recommendations from this study will sensitise researchers in the field of male involvement in PMTCT in improving the quality of their studies by adjusting for confounders.
Implications for public health policy
The Joint UNAIDS has set the 90–90–90 target as a road map towards the end of the AIDS pandemic by 2030.38 The second ‘90’ target is for 90% of all people living with HIV to be receiving antiretroviral medication by 2020.38 HIV-positive pregnant women constitute a unique group of HIV patients that need to be targeted if the ambitious goal of ending the AIDS pandemic should come to fruition. Our study has provided the relevant guidance towards the attainment of the second UNAIDS ‘90’ target. The findings from this study can help Ministries of Health, HIV/AIDS organisations and programme implementers direct appropriate interventions on how to ensure increased and sustainable uptake of ART by HIV-positive pregnant women through adequate engagement of their male partners. The evidence from this study suggests that there should be emphasis on complex community interventions described in this paper since they have the propensity of engaging HIV-positive pregnant women and their partners from the ‘grassroots’ in SSA. These community interventions are currently piloted in many settings in SSA, but there is need for urgent scale-up given that we are less than 4 years to go before the 2020 UNAIDS deadline. Importantly, this scale-up should be implemented after cost-effectiveness analyses studies of the complex community intervention package have been conducted.
Recommendations for future research
Few randomised trials have been carried out to investigate the impact of male partner involvement on the uptake of maternal ART. More randomised trials are needed to add to the strength evidence available. Stratified analysis of the various components of the complex intervention package is needed. Future systematic reviews following additional empirical evidence are also needed. Finally, an economic evaluation is needed to adequately inform policy.
Conclusion
Enhanced psychosocial interventions and complex community interventions increase male partner involvement and the uptake of PMTCT services more than any other intervention. Invitation letters had no effect. The combined model showed high heterogeneity, whereas the heterogeneity was moderate using adjusted ORs. More randomised trials and observational studies (that have adjusted for potential confounders) are needed in the future.
Acknowledgments
The authors thank the University of Glasgow Library for access to Ovid MEDLINE, Ovid EMBASE and other search databases.
References
Footnotes
Contributors NFT and CJ conceived the paper, developed the search strategy, independently searched the literature and screened the articles and carried the meta-analysis and metaregression. NFT made the first draft of the manuscript. NFT, ITRK and CJ reviewed several versions of the manuscript. All the authors read and approved the final manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Extra data are available by emailing takahnoah@yahoo.com.