Article Text

Abstract
Objective The numbers of lower extremity revascularisations and amputations are insufficiently reported in Norway. To support future policy decisions regarding the provision of vascular treatment, knowledge of such trends is important.
Methods This retrospective cross-sectional study from 2001 to 2014 used data from the Norwegian Patient Registry. The revascularisation treatments were categorised in multilevel, aortoiliac, femoral to popliteal and popliteal to foot levels and sorted as open, endovascular and hybrid. The sessions in amputations were divided in major (thigh and below knee) and minor (ankle, foot or digit). Incidence rates were assessed per 100 000 for patients in the age group >60 years. The diabetic prevalence was calculated and the endovascular numbers at the South-Eastern, Western, Central and Northern Norway Regional Health Authority were compared.
Results The overall revascularisation rates increased from 308.7 to 366.8 (p=0.02). Open revascularisations decreased from 158.9 to 98.7 (p<0.01) while endovascular revascularisations increased from 142.2 to 243.4 (p<0.01). Hybrid revascularisations increased from 7.4 to 24.8 (p<0.01). Major amputation rates decreased from 87.8 to 48.7 (p<0.01) while minor amputations increased from 12.3 to 19.6 (p=0.01). The diabetic percentages increased from 12.2 to 22.3 (p<0.01) in revascularisations, from 26.5 to 30.8 (p=0.02) in major amputations and from 43.0 to 49.3 (p=0.13) in minor. (p values refer to average annual changes.) The regional trends in endovascular treatments varied within and between the vascular groups.
Conclusion From 2001 to 2014, the revascularisation rates increased due to the rise in endovascular procedures. Open revascularisations and major amputation rates decreased, minor increased. The regional variances in endovascular treatments indicate that the availability of this technology differed between the health regions of Norway. The increase in patients with diabetes requires continued awareness of diabetes and its complications.
- vascular surgery
- interventional radiology
- health policy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study is the first to demonstrate Norwegian trends in the numbers of open and endovascular treatments for peripheral arterial disease including lower extremity amputations, the diabetic prevalence in these treatments and the regional variances in use of endovascular technology.
The study provides valuable knowledge for future provision of vascular treatment.
Results are subject to potential errors in records, coding and analysis.
The data were anonymous and did not include outcome measures.
The study was not designed to establish causal relations.
Introduction
Endovascular procedures are now more commonly performed than open surgery in many Western countries in the invasive treatment of lower peripheral arterial disease. This has led to an increase in revascularisation rates during the past decades and more patients are treated.1 2 The only randomised controlled trial comparing the effectiveness of endovascular intervention with open surgery so far, reported similar short-term outcomes between the two treatment strategies,3 and in recent guidelines an ‘endovascular-first-strategy’ is advocated for almost all types of lesions. Although at a decreasing rate, some complex lesions are still ideally treated by surgical approach.4
On a global level, peripheral arterial disease is one of the most prevalent, morbid and mortal diseases and affected more than 202 million individuals in 2010. The disease is now reported coprevalent among men and women in high-income countries and possibly more prevalent in women than men in low- and middle-income countries. Peripheral arterial disease is relatively uncommon in people younger than 40 years but affects 1 in 10 people aged 70 years and 1 in 6 people older than 80 years. The prevalence of the disease increased by 23.5% between 2000 and 2010.5 6
Smoking and diabetes are identified as the most important risk factors associated with the development of the disease.5 7 Smoking relates to atherosclerosis of proximal segments, diabetes to that of the distal segments.8 Peripheral arterial disease is more severe and progresses more rapidly in people with diabetes than those without. These patients are also at higher risk for lower extremity amputations and reamputations.9 10 In patients with diabetes who are smokers, there is an additive risk.11 Smoking cessation is associated with a decline in the incidence of peripheral arterial disease.12
Recent studies have demonstrated a decrease in major amputations rates and a slight increase in minor amputations.2 13 14 An association between the increased application of endovascular technology and the reduced major amputation rates in patients with peripheral arterial disease has been suggested.1 15 Advances in medical therapy, decreased smoking prevalence and widespread improvements in peripheral arterial disease screening programme are other likely explanations for the reduction in major amputation rates.1 16
Norwegian numbers of lower extremity revascularisations and amputations have been insufficiently reported. To support future policy decisions regarding the provision of vascular treatment in the country, knowledge about these trends is important. The objective of this study was to investigate the Norwegian changes in numbers of open and endovascular revascularisations and lower extremity amputations and assess the diabetic prevalence in these treatments from 2001 to 2014. With regards to the political goal of equitable healthcare in the country, we also investigated and compared regional trends in endovascular treatments.
Material and methods
The material was based on retrospective analysis of anonymous treatment sessions extracted from the Norwegian Patient Registry (NPR).17 This is an independent, administrative registry of all patient treatment sessions (including also outpatients) in the public healthcare of Norway. The registry was established in 1997 and is owned by the Norwegian Ministry of Health and Care Services. The Norwegian Directorate of Health granted permission to use the anonymous data.
The unit of analysis was the treatment sessions including procedure18 and diagnosis codes19 as listed in online supplementary appendix 1A, 1B, 1C and 1D. The inclusion of all diagnosis codes from the Norwegian version of International Classification of Diseases (ICD) I70–I7919 was considered the best alternative for all groups to avoid inaccuracies and possible errors in the diagnostic coding. The listed vascular procedure codes are closely connected to peripheral arterial disease. This is not as evident for the procedure codes in the amputation groups. Consequently, amputations caused by any arterial disease from ICD I70-I7919 were included in the study. However, it is reasonable to assume that the vast majority of these lower extremity amputations were actually caused by peripheral arterial disease.20 21 Amputations caused by other conditions such as trauma, venous and lymphatic disorders and malignancies were excluded. All treatment sessions were analysed in combination with these variables: the patient’s age, sex, treatment site (hospital or health trust) and home county. As the majority of treatments (86.8%) were on patients aged >60 years this age group was used for calculation of incidence rates per 100 000. For transparency, the numbers of treatment sessions in the age groups <60 and ≥60 years were compared (see online supplementary appendix 2A, 2B, 2C, 2D and 2E). Numbers for the per capita calculations and developments in national smoking habits were obtained from Statistics Norway.22
Supplementary file 1
The treatments in the revascularisation group were categorised in four groups: multilevel (across the aortoiliac and infrainguinal levels), on the aortoiliac level, on the femoral to popliteal level and on the popliteal to foot level and sorted into open, endovascular and hybrid treatments. Hybrid treatments were defined as a combination of open and endovascular procedures. We identified a small number of endoscopic aortoiliac and infrainguinal treatment sessions. These were excluded from further analyses. The treatments in the lower extremity amputation group were divided in major amputations (thigh and below knee), major amputation revisions, minor amputations (ankle, foot or digit) and minor amputation revisions. National incidence rates are presented in table 1A and figures 1–5 and the numbers (%) of treatments in individuals with diabetes in table 1B. The hybrid treatments were added to the endovascular treatments in the analysis of regional variances shown in tables 2, 3, 4 and 5. Two of the authors cross-checked the extraction of data from the NPR and performed the analysis independently to increase the reliability of the results.
Changes over time for incidence rates per 100 000 ≥60 years for treatment sessions in multilevel, aortoiliac, femoral to popliteal and popliteal to foot revascularisations and lower extremity amputations in Norway from 2001 to 2014+
Changes over time for treatments in individuals with diabetes ≥60 years in main groups

Trends in multilevel revascularisations (treatment sessions) in age group ≥60 years.

Trends in aortoiliac revascularisations (treatment sessions) in age group ≥60 years.

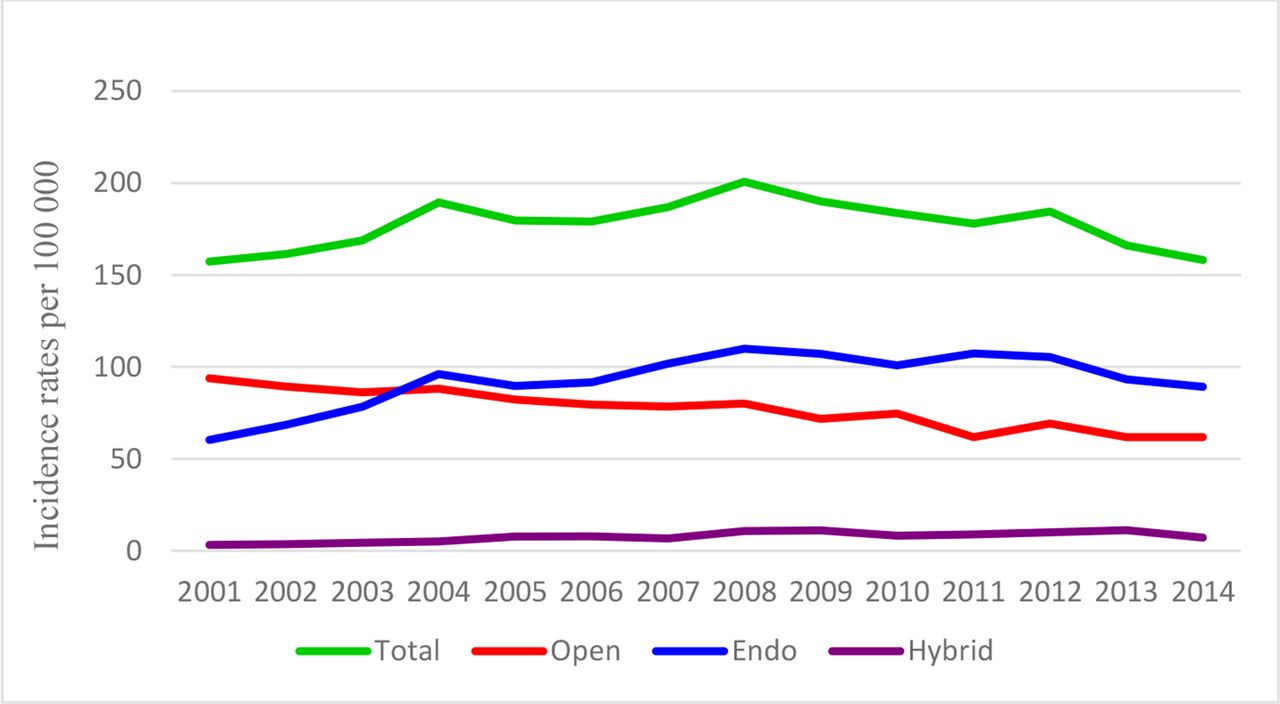
Trends in femoral to popliteal revascularisations (treatment sessions) in age group ≥60 years.

Trends in popliteal to foot revascularisations (treatment sessions) in age group ≥60 years.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trends in lower extremity amputations and revisions (treatment sessions) in age group ≥60 years.
Regional overview showing variances in percentages of endovascular treatments among the conducted multilevel revascularisations from 2001 to 2014+
Regional overview showing average annual increase (%) in endovascular treatments among the conducted multilevel revascularizations from 2001 to 2014+
Regional overview showing variances in percentages of endovascular treatments among the conducted aortoiliacal revascularisations from 2001 to 2014+
Regional overview showing average annual increase (%) in endovascular treatments among the conducted aortoiliac revascularizations from 2001 to 2014+
Regional overview showing variances in percentages of endovascular treatments among the conducted femoral to popliteal revascularisations from 2001 to 2014+
Regional overview showing average annual increase (%) in endovascular treatments among the conducted femoral to popliteal revascularizations from 2001 to 2014+
Regional overview showing variances in percentages of endovascular treatments among the conducted popliteal to foot revascularisations from 2001 to 2014+
Regional overview showing average annual increase (%) in endovascular treatments among the conducted popliteal to foot revascularizations from 2001 to 2014+
Since 2002, the Norwegian government has been responsible for the specialist healthcare service in the country. The hospitals are organised into health trusts, which again are grouped into regional health authorities. During the study period, some hospitals reported directly to the NPR while others reported to their health trust from which the number of treatments were forwarded collectively. Centralising efforts from the health authorities reduced the number of health trusts from 47 in 2001 to 26 in 2014. To avoid overly detailed information about trends in hospitals and health trusts that merged with others during the period, the lowest level of treatment site used in the analyses was the Norwegian Regional Health Authorities (NRHAs). In 2007, the number of authorities was reduced from five to four as the South and the Eastern NRHA merged. For practical reasons, the current organisational model with the South-Eastern, Western, Central and Northern NRHA was used.
Statistical analyses
The statistical analyses were performed with Stata V.14.0 (Stata Corp). We used linear regression with analytical weights to calculate average annual changes in rates and percentages, and the two-sample test of proportions. The significance level was set at ≤0.05.
Results
From 2001 to 2014, the population of Norway increased from 4.5 to 5.1 million. The proportion aged >60 years increased from 19.3% to 21.5%. The South-Eastern NRHA was the largest authority with responsibility for more than half of the population, 2.8 million in 2014. The corresponding population was 1.1 in the Western, 0.7 in the Central and 0.5 in the Northern NRHA.22
A total of 55 028 treatment sessions were categorised in the four revascularisation groups while 13 074 treatment sessions were categorised in the four lower extremity amputation groups.
6 060 of the vascular treatment sessions below the infrainguinal level included procedure codes from both the femoral to popliteal and the popliteal to foot level and were categorized in both groups. Some of the vascular sessions also included procedure codes from the amputation group. These combined treatments were identified in 1 370 (2.5%) of the vascular sessions.
Multilevel revascularisations
Total numbers
Treatment sessions of 5 738 were identified as multilevel revascularisations. In these, 4 922 (85.8%) of the patients were aged >60 years and 3 472 (60.5%) were men. Multilevel treatments of 2 082 (36.3%) contained only open procedure codes while 2 005 (34.9%) contained only endovascular procedure codes. Treatments of 1 651 (28.8%) contained both and were categorised as hybrid multilevel treatments (see online supplementary appendix 2A).
Incidence rates
The annual incidence rates of multilevel revascularisations increased from 20.4 in 2001 to 39.9 in 2014 per 100 000 for the age group >60 years. Applying linear regression with year (time) as the independent variable, the average annual increase in these incidence rates per 100 000 was 1.7 (p<0.01). The open multilevel revascularisations decreased from 14.3 to 11.7 (annual change −0.2; p=0.09), while the endovascular increased from 3.7 to 12.3 (annual change 0.7; p<0.01). The hybrid treatments increased from 2.4 to 15.9 (annual change 1.1; p<0.01). (table 1A)
Developments of treatments in individuals with diabetes
The treatments including individuals with diabetes in the multilevel group increased from 9.6% in 2001 to 17.4% in 2014 (annual increase 0.6%, p<0.01) (table 1B).
Regional variances
Table 2A,B presents the regional variances in percentages of endovascular treatments among the conducted multilevel treatments based on regression analysis. Table 2A shows that the average annual increase across the regions was 2.5% (p<0.01), whereas the Northern, South-Eastern and Central performed from 14.1% to 17.5% (p values <0.01) more multilevel endovascular treatments compared with the Western NRHA during the period. Table 2B shows the differences in annual growth between the regions. The South-Eastern had an estimated average annual growth of 1.9% during the period, while the Western had a growth of 4.2% (p values <0.01). However, the South-Eastern also started at the highest estimated share, 35.7% more than the reference group (the Western). This indicates that the growth was highest in regions that started at lower shares.
Aortoiliac revascularisations
Total numbers
Treatments sessions of 17 118 were registered with procedure codes from only the aortoiliac level. In these, 12 826 (74.9%) of the patients were aged >60 years and 10 074 (58.9%) were men. Of the aortoiliac revascularisations, 3 783 (22.1%) contained only open procedure codes while 13 201 (77.1%) contained only endovascular codes. Categorised as hybrid treatments were 134 (0.8%) (see online supplementary appendix 2B).
Incidence rates
The annual incidence rates of open aortoiliac revascularisations decreased from 27.8 to 12.4 per 100 000 for the age group >60 years (annual change −1.3; p<0.01). Endovascular revascularisations increased from 54.2 to 74.1 (annual change 1.8; p<0.01) while hybrid revascularisations remained at 0.5 (annual change 0.02; p=0.52) (table 1A).
Developments of treatments in individuals with diabetes
The treatments including individuals with diabetes in the aortoiliac group increased from 8.7% in 2001 to 15.9% in 2014 (annual increase 0.4%, p<0.01) (table 1B).
Regional variances
Table 3A,B presents the regional variances of endovascular treatments among the conducted aortoiliac treatments. Table 3A shows that the average annual increase across the regions was 1.4% (p<0.01) whereas the South-Eastern, Central and Western performed from 3.0% to 6.9% (p values ≤0.05) more aortoiliac endovascular treatments compared with the Northern NRHA during the period. Table 3B shows the differences in annual growth between the regions. The Central had an estimated average annual growth of 0.03% (p=0.91) while the Northern NRHA, that started at the lowest share, had a growth of 1.8% (p<0.01).
Femoral to popliteal revascularisations
Total numbers
Treatment sessions of 26 668 were registered in the femoral to popliteal revascularisation group. In these, 23 952 (89.8%) of the patients were aged >60 years and 15 428 (57.9%) were men. Of the sessions, 11 527 (43.2%) were registered with only open procedure codes and 13 980 (52.4%) were registered with only endovascular codes. Categorised as hybrid treatments were 1 161 (4.4%) (see online supplementary appendix 2C).
Incidence rates
The annual incidence rates of open femoral to popliteal revascularisations decreased from 93.8 to 61.8 per 100 000 for the age group >60 years (annual change −2.5; p<0.01). Endovascular revascularisations increased from 60.3 to 89.2 (annual change 2.2; p=0.01). Hybrid revascularisations increased from 3.2 to 7.2 (annual change 0.5; p<0.01) (table 1A).
Developments of treatments in individuals with diabetes
The treatments including individuals with diabetes in the femoral to popliteal group increased from 13.3% in 2001 to 22.9% in 2014 (annual increase 0.7%, p<0.01) (table 1B).
Regional variances
Table 4A,B presents the regional variances of endovascular treatments among the conducted femoral to popliteal treatments. Table 4A shows that the average annual increase across the regions was 1.6% (p<0.01), whereas the Central, Western and South-Eastern performed from 11.6% to 19.6% (p values <0.01) more endovascular treatments in this group compared with the Northern NRHA. Table 4B shows the differences in annual growth between the regions. The South-Eastern had an estimated average annual growth of 1.1% while the Western NRHA that had a lower share in 2001, had a growth of 3.2% (p values <0.01).
Popliteal to foot revascularisations
Total numbers
Treatment sessions of 11 564 were registered in the popliteal to foot revascularisation group. In these, 10 515 (90.9%) of the patients were aged >60 years and 6 880 (59.5%) were men. Of the sessions, 2 727 (23.6%) were registered with only open procedure codes, 8 623 (74.6%) were registered with only endovascular codes. Categorised as hybrid treatment were 214 (1.9%) (see online supplementary appendix 2D).
Incidence rates
The annual incidence rates of open popliteal to foot revascularisations decreased from 23.1 to 12.8 (annual change −0.9; p<0.01). Endovascular revascularisations increased from 24.2 to 67.9 (annual change 4.0; p<0.01). Hybrid revascularisations decreased from 1.3 to 1.2 (annual change 0.06; p=0.13) (table 1A)
Developments of treatments in individuals with diabetes
The treatments including individuals with diabetes in the popliteal to foot group increased from 15.7% in 2001 to 30.2% in 2014 (annual increase 0.9%, p<0.01) (table 1B).
Regional variances
Table 5A,B presents the regional variances of endovascular treatments among the conducted popliteal to foot treatments. Table 5A shows that the average annual increase across the regions was 2.4% (p<0.01), whereas the Northern performed 4.9% (p=0.23), the Central 5.1% (p=0.14) and the South-Eastern 10.7% (p<0.01) more of these endovascular treatments compared with the Western NRHA. Table 5B shows that the South-Eastern had an estimated average annual growth of 1.8% while the Western NRHA, that started at the lowest share, had a growth of 4.0% (p values<0.01).
Lower extremity amputations
Total numbers
Treatment sessions of 13 074 were registered with one or more procedure codes from the lower extremity amputation groups. In these, 12 162 (93.0%) of the patients were aged >60 years and 7 702 (58.9%) were men (see online supplementary appendix 2E).
Incidence rates
Treatments categorised as major lower amputations decreased from 87.8 to 48.7 per 100 000 for the age group >60 years (annual change −3.2; p<0.01). Major lower amputation revisions decreased from 4.8 to 3.8 (annual change −0.1; p=0.09). Minor lower amputations increased from 12.3 to 19.6 (annual change 0.6; p=0.01), while minor lower revisions increased from 1.0 to 3.6 (annual change 0.1; p=0.04) (table 1A).
Developments of treatments in individuals with diabetes
The treatments including individuals with diabetes in the major lower amputation group increased from 26.5% in 2001 to 30.8% in 2014 (annual change 0.4%, p=0.02). Major amputation revisions in individuals with diabetes decreased from 31.0 in 2001 to 23.8% in 2014 (annual change 0.4, p=0.60). Minor amputations in individuals with diabetes increased from 43.0% to 49.3% (annual change 0.4, p=0.13), while minor amputation revisions in individuals with diabetes increased from 44.4% to 56.4% (annual change −0.2, p=0.85) (table 1B).
Other inclusive results
The number of units that reported revascularisations to NPR changed during the period. In 2001, we identified 34 hospitals and 4 health trusts, in 2007, 15 hospitals and 7 health trusts and in 2014, 13 hospitals and 7 health trusts. Less than 1% of the treatment sessions in the study included patients treated at other regions than their own. All four NRHA’s took part in this exchange of patients across regional borders.
Discussion
In line with international trends, this study demonstrated an increase in the total revascularisation rates from 2001 to 2014 caused by an increase in endovascular and hybrid treatments. Rates of open surgery decreased. These trends were similar in all the vascular groups. The increase was highest in the endovascular popliteal to foot group and in the hybrid multilevel group. The decrease was most evident in the open femoral to popliteal group. Parallel to the increase in endovascular revascularisations, the major amputation and major amputation revision rates decreased. This cross-sectional study cannot establish whether this represents a direct cause and effect, neither was the study designed to evaluate other possible causes. However, from 1974 through 2001 to 2014 the percentage of daily smokers in Norway in the age group 16–74 years has gradually reduced from 52 through 30% to 14% among men and from 32 through 31% to 13% among women.22 It is likely that this decrease in smoking habits, has contributed to the reduction in major amputation rates. On the other hand, the percentage of individuals with diabetes increased significantly in all the revascularisation groups and diabetes itself profoundly increases the risk of amputation.10 11
In the present study and in alignment with diabetic complications, the percentage of individuals with diabetes was highest in the patient groups with popliteal to foot revascularisations and amputations, in particular minor amputations and minor amputation revisions. Although diabetes occurrence appears to be levelling off in Norway, the prevalence of oral antidiabetic use increased from 2.5% in 2005 to 3.2% in 2011. The use increased strongly with age with a peak in men at age 76 (12.4%) and in women at age 80 (9.9%).23 As the population in Norway is ageing, the number of patients with diabetes with peripheral arterial disease is likely to further increase.
A recent German study highlighted the high rates of limb amputation and mortality in patients with peripheral arterial disease and diabetes, and particularly in those with diabetic foot syndrome in an in-hospital setting. Patients with diabetics also had a high reamputation risk for the ipsilateral and contralateral limb during a long-term follow-up. Possible reasons for this are that patients with diabetes are inadequately and insufficiently diagnosed and treated before an amputation.10 A study from Norway and the city of Trondheim showed a 40% decline in major amputations (amputation through or above the ankle joint) in patients with diabetes from 1996 to 2006 simultaneously as a diabetic foot team started consultation services. These results could not be attributed to an increase in vascular interventions because this rate was unchanged in the same period. In addition to information and preventive care, the main treatment strategy for the diabetic foot team was off-loading of neuropathic ulcers, vascular intervention in cases of neuroischaemic ulcers and radical debridement in cases of chronic osteomyelitis.24 To further reduce the national incidence of diabetic amputations, the primary health and specialist health service in Norway must cooperate more closely.25 Our study demonstrated a higher percentage of men than women in all age groups. The underlying causes for these results need further population-based investigations.
This study documented regional variances in use of endovascular revascularisations both within and between the vascular groups. It is unlikely that these variations were caused by regional differences in the anatomy of the lesions or basic variations in the occurrence of peripheral arterial disease alone. More likely, these regional variances indicate a difference in availability of endovascular technology. Regional variations in use of endovascular technology in Norway have also been demonstrated for abdominal aortic aneurysms.26 The developments in endovascular interventions require resources and new medical equipment, education of staff and new organisation models with cooperation between vascular surgeons and radiologists. Norway’s geography, with large and sparsely populated areas, challenges the political goal of equal access to healthcare. In some regions, travel distances to even a small hospital are several hours and it is difficult to staff and equip all treatment sites in a specialised endovascular mode. Since the first report from the Norwegian association for vascular surgery in 2001 about the provision of vascular surgery, there has been an ongoing debate about where vascular treatments should be performed.27 28 Centralising versus decentralising, threats to hospital’s future existence and the relationship between volume and quality have been thoroughly debated without any conclusive results.
In this study, it was not possible to assess the developments in numbers of treatment cites because the reporting routines varied among the hospitals and health trusts during the period. Although our analysis indicated that the regions with the lowest share had the highest annual growth in endovascular treatments, it is uncertain when and if the regions will be equal in performance of these treatments. We therefore encourage an assessment of professional and technological resources at all present treatment sites for revascularisations and suggest an allocation of future revascularisations to specialised vascular centres in the regions. New technology is introduced in many medical specialities. If the healthcare system is not organised accordingly, regional variances in treatment strategies will become an increasing challenge for several specialities.
This study was based on material from the NPR. All hospitals in Norway must report to this registry directly or through their health trust when they discharge patients. The authorities use the NPR for statistics and to calculate reimbursements through the diagnoses-related group system. Fifty per cent of the hospitals’ funding was based on these data in 2014.29 Thus, there is also an economic incentive to report. To investigate the quality of data in the study, a selection of numbers registered in the NPR were compared with the corresponding numbers in NorKar, the clinical quality registry for vascular surgery in Norway. This registry was established in 1996 but national registration routines have been incomplete. Since 2013, it has been mandatory to report also to NorKar. One hospital from each of the four regions was identified in both registers for 2013. Compared with 1 189 aortoiliac and infrainguinal treatment sessions registered in the NPR, 937 (78.8%) were reported to NorKar.30
A central registry for amputations was first established in Norway in 2014.31 Thus, to validate the numbers of amputations used in this study, several of the treatment sites were contacted. The local registration routines for amputations varied both within and between these sites. This made a large-scale validation between local registries and the numbers registered in the NPR difficult. Eventually, a hospital in the Western NRHA provided a list with treatment sessions on major amputations and major amputation revisions from 2001 to 2013. Compared with 586 treatment sessions in the local registry, 545 (93.0%) were registered in the NPR.
Strength and weaknesses in the study
Our study is the first to show Norwegian trends in open and endovascular revascularisations including lower extremity amputations, the diabetic prevalence in these treatments and regional variances in use of endovascular technology. Large datasets, such as the one used in the present study, are the only valid method available for recognising national trends in patient treatments. However, there are also limitations. Results are subject to potential errors in records, coding and analyses. The treatment sessions were anonymous and some patients were included more than once in the statistics. The study was designed to investigate trends in the numbers of treatments and not indications for treatment, clinical outcomes or causal relations. Planning for future healthcare should also include cost analysis, in addition to outcome measures like short and long-term survival, thus including knowledge of quality and not only trends of practice.
Conclusion
Trends in the numbers of open and endovascular revascularisations and amputations in lower extremities in Norway from 2001 to 2014 were in line with international experience. The increases in treatment sessions involving patients with diabetes underlines the long-term complications associated with diabetes. The population in Norway is ageing and an increase in patients with diabetes and peripheral arterial disease must be expected. The study documented regional variances in the increased use of endovascular treatments, indicating that the availability of this technology differed. To provide equal healthcare to the population, we suggest an allocation of future revascularisations to specialised vascular centres.
References
Footnotes
Contributors KW, EF and KKS designed the study. RK conducted the data collection from the Norwegian Patient Register with support from KW. FG conducted the statistical analyses in cooperation with KW. KW wrote the draft of the manuscript. All authors contributed to the interpretation of data, critically reviewed the manuscript and approved the final version.
Disclaimer Data from the Norwegian Patient Registry was used in this publication. The interpretation and reporting of these data are the sole responsibility of the authors. No endorsement by the Norwegian Patient Registry is intended nor should be inferred.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.