Article Text

Abstract
Introduction First Nations people are descendants of Canada’s original inhabitants. In consequence of historical and ongoing structural injustices, many First Nations families struggle with challenging living conditions, including high rates of poverty, poor housing conditions, mental illness and social isolation. These risk factors impede caregivers’ abilities to meet their children’s basic physical and psychosocial needs. Home visiting programmes were developed to support child developmental health in families facing parenting challenges. However, whether home visiting is an effective intervention for First Nations families has not been examined. We are evaluating two home visiting programmes in Manitoba, Canada, to determine whether they promote nurturing family environments for First Nations children.
Methods and analysis This research builds on new and established relationships among academic researchers, government decision-makers and First Nations stakeholders. We will link health, education and social services data from the Manitoba Population Research Data Repository to data from two home visiting programmes in Manitoba. Logistic regression modelling will be used to assess whether programme participation is associated with improved child developmental health, better connections between families and social services, reduced instances of child maltreatment and being taken into out-of-home care by child welfare and reduced inequities for First Nations families. Non-participating individuals with similar sociodemographic characteristics will serve as comparators. We will use an interrupted time series approach to test for differences in outcomes before and after programme implementation and a propensity score analysis to compare differences between participants and non-participants.
Ethics and dissemination Approvals were granted by the Health Information Research Governance Committee of the First Nations Health and Social Secretariat of Manitoba and the University of Manitoba Health Research Ethics Board. Our integrated knowledge translation approach will involve disseminating findings through government and community briefings, developing lay summaries and infographics, presenting at academic conferences and publishing in scientific journals.
- home visiting
- first nations
- administrative data
- child maltreatment
- social services
- health equity
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The use of comprehensive administrative data from the Manitoba Population Research Data Repository is a major strength of our study, as it allows linkage of population-level health, education and social data to study short-term and long-term outcomes associated with home visiting in First Nations families.
Our collaborative research approach building on new and established relationships among academic researchers, First Nations stakeholders and government decision-makers will ensure that the findings are culturally relevant and will inform current policies and practices.
While longitudinal databases allow for real-world evaluations of programmes and policies, inverse probability of treatment weight analyses are sensitive to unmeasured confounding and interrupted time series can be sensitive to unmeasured time-varying confounders.
We are limited by the outcome measures available in our administrative data, as health and social outcomes are captured only when contact with the healthcare and social services systems is made and, therefore, outcomes not captured could reduce the statistical power of analyses.
Because we are conducting an observational study where participation in home visiting is voluntary, we will not be able to determine whether differences in outcomes are due to a true programme effect or whether they are attributable to unmeasured confounding. We will conduct a sensitivity analysis to help identify weak effects that are very likely due to unmeasured confounding.
Introduction
The environment in which children live and grow strongly influences their developmental health.1 Key aspects of healthy child development include favourable family environments,2 secure attachments to a caregiver,3 positive maternal mental health4 and socioeconomic status.5 6 However, adverse childhood conditions such as parental substance abuse, poor mental health or poor parent–child relationships are associated with negative behavioural, emotional and cognitive outcomes and put children at risk for maltreatment.7 8 Child maltreatment is defined as any act of commission or omission by a caregiver that results in harm or threat of harm to a child, including physical, sexual or emotional abuse, neglect or witnessing intimate partner violence. Child maltreatment can have long-lasting effects, as it increases the likelihood of poor mental and physical health, low educational outcomes, unemployment and homelessness later in life.9–15
Canadian Indigenous children,16 and First Nations children specifically,17 are over-represented among reported maltreatment cases and referrals to child protection services (see box 1 for more details).18 This over-representation is driven by several related risk factors including poverty, poor housing, substance misuse, domestic violence and social isolation19 as well as by prejudice and inequitable funding within the child welfare system.20 21 Many of these risk factors are associated with the intergenerational trauma resulting from the legacy of the residential school system in Canada,22 23 which continues to impede First Nations caregivers’ ability to meet their children’s basic physical and psychosocial needs. A complex set of issues, including poor understanding of the structural factors (such as poverty) that influence family functioning as well as a scarcity of culturally appropriate maltreatment prevention services, contribute to high rates of First Nations children being taken into out-of-home care by a child welfare agency.17 In 2014, the Assembly of Manitoba Chiefs produced a report highlighting the harmful and discriminatory practices of the current child welfare system with respect to First Nations families in Manitoba, calling the system ‘an extension of the cultural genocide experienced by the Residential School years and the Sixties Scoop’.24 As evidence for the negative effects of child maltreatment and family disruption on early childhood development continues to mount,25 it is clear that greater efforts are required to promote environments that are nurturing for children, particularly in First Nations families living in challenging conditions.
Canada’s First Nations
‘Indigenous peoples’ is a collective name for the original peoples of North America and their descendants. Three broad groups of Indigenous peoples are recognised by the Canadian Constitution: First Nations, Inuit and Métis. There are more than 600 distinct First Nation peoples across Canada, each with their own unique histories, languages, cultural practices and spiritual beliefs.
The majority of Canada’s First Nations reserves were established in Canada during the 1800s. A reserve is a tract of land set aside under the Indian Act and treaty agreements for the exclusive use of First Nations people; the land is not strictly owned by the First Nations but is held in trust by the Crown. In 1867, the federal government deemed First Nations wards of the state and assumed responsibility for First Nations and reserve lands by introducing the Indian Act,80 which grants the Minister of Indigenous and Northern Affairs jurisdiction over most activities taking place on reserves. Reserves are now more commonly referred to as First Nations communities .
In Manitoba, there are 63 communities and 130 000 registered First Nations people, of whom about 60% live in communities. Among the Canadian provinces, Manitoba has the second-largest First Nations population (after Ontario) and the highest proportion of First Nations people.81
The history of colonisation in Canada includes social policies that stripped First Nations people and other Indigenous peoples of their culture, language and identities and the legacy of these oppressive practices continues to impact their health status today. Colonialism is perhaps the most important predictor of the persistent gap in health, social and economic outcomes between First Nations and non-First Nations populations.43
One of the most widespread interventions aimed at promoting children’s long-term developmental health and well-being26–28 and preventing children from being taken into out-of-home care29 is home visiting. Home visiting programmes offer regular home visits by public health nurses or other trained professionals or paraprofessionals to families who face multiple parenting challenges and who may be at risk for neglecting or abusing their children. The home visitors focus on strengthening child–parent relationships, connecting families with services in their community and providing support to parents to decrease stress, improve self-efficacy and improve education and employment opportunities. There have been numerous evaluations of the impact of home visiting programmes on child maltreatment and family functioning in both USA30–36 and Canada.37 38 The Home Visiting Evidence of Effectiveness review examined 32 home visiting models, many of which had favourable impacts in domains of child development and family environment (eg, school readiness, positive parenting practices); however, larger effect sizes tended to occur only in programmes that focus on high-risk families.39 Many First Nations families in Canada live in conditions of high risk for child maltreatment40–42 and First Nations organisations and families have repeatedly reported prejudice in the child welfare system.24 However, to this date, no evaluation has focused specifically on home visiting in First Nations families. There remains a distinct lack of evidence for effective programmes to reduce the risk for child maltreatment and children being taken into care in this population. This is an important literature gap to address, because First Nations-specific findings may be different from the results of broader home visiting programme evaluations. First Nations families experience a unique set of contextual and cultural factors that may influence how programme effects manifest in this population. The dearth of information about health and social outcomes for First Nations families is itself a form of inequity, as the current political climate increasingly prioritises evidence-based evaluations to make important funding decisions.
Our study, ENVISION: Evaluating Home Visiting Interventions for First Nations Families, seeks to address this knowledge gap by evaluating home visiting interventions that aim to improve First Nations family functioning and reduce instances of child maltreatment and children being taken into care in the province of Manitoba, Canada. Two home visiting programmes have been operating in Manitoba for over a decade: the Strengthening Families Maternal Child Health (SF-MCH) programme, which operates in First Nations communities and the Families First Home Visiting (FFHV) programme, which operates in all other areas of Manitoba. ENVISION will build on existing collaborations with First Nations researchers, programme managers and communities to generate population-level evidence about the impact of these home visiting interventions on health and social outcomes for First Nations families and on health equity. Established relationships between academic researchers and decision makers from Nanaandawewigamig (the Spirit Name of the First Nations Health and Social Secretariat of Manitoba, meaning ‘Healing Place’) and in the Manitoba government’s Healthy Child Committee of Cabinet will ensure that the evidence generated is integrated into government policy and practices. The funding for ENVISION was awarded in 2016, and the study will run until February 2019.
Methods and analysis
Conceptual framework
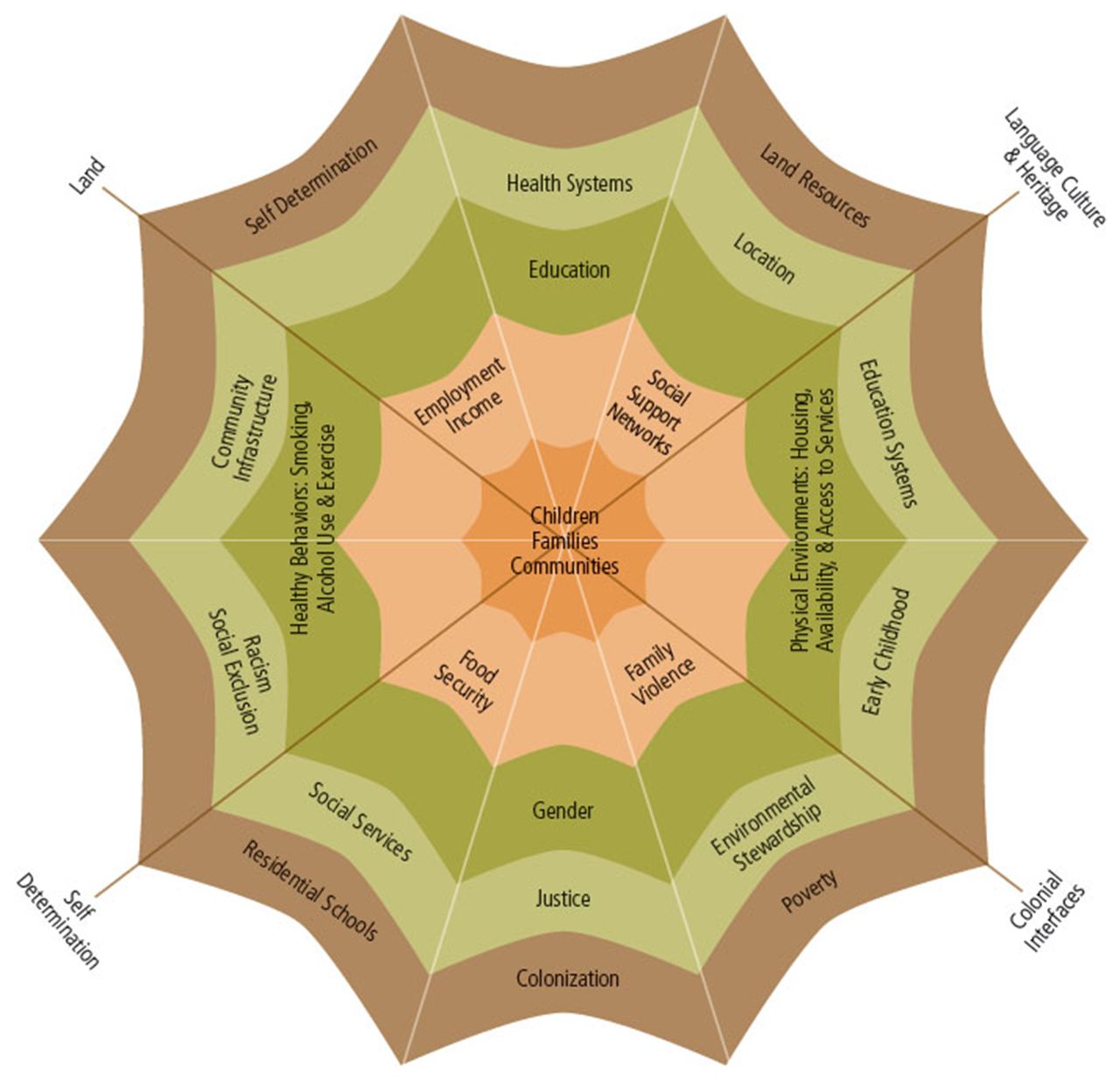
The conceptual framework guiding this population health intervention research is based on the work of de Leeuw and Greenwood (figure 1),43 which recognises the multiple social determinants affecting family functioning among First Nations and also influencing health inequities between Indigenous and non-Indigenous populations. While the interventions being evaluated will focus on the proximal determinants of child and parental health (eg, social supports, family violence), these proximal determinants are influenced by intermediate determinants (eg, poverty, community infrastructure) which are in turn influenced by distal determinants such as colonialism, racism, social exclusion and the degree of self-determination experienced by First Nations people. Although ENVISION’s outcomes are mainly proximal to intermediate determinants of family functioning and health equity, we understand that the greatest impacts on improving health equity for First Nations populations will come from changes at the most distal levels.

{kind=link}
De Leeuw and Greenwood’s ‘Web of Being’, depicting the social determinants of Indigenous people’s health.44 Used with permission from the National Collaborating Centre for Aboriginal Health.
Overview of collaborative research approach and research questions
The purpose of ENVISION is to evaluate the impact of the off-reserve FFHV and on-reserve SF-MCH programmes for First Nations families. From the very conception of this research, we recognised that collaboration with First Nations stakeholders was vital to the success of the study. Engaging partners from Nanaandawewigamig (the Spirit Name of the First Nations Health and Social Secretariat of Manitoba) and the Manitoba government throughout the research design process has been key to ensuring that the research acknowledges cultural and historical contexts and uses the most relevant and appropriate measures of child health equity. This collaborative team approach will aid us in developing suitable methods to interpret the results of the study and determine how best to disseminate the findings to ensure that our work benefits on-reserve and off-reserve First Nations families. This will involve employing ‘two-eyed seeing’, which recognises and incorporates both Indigenous and Western ways of knowing in research as well as colearning and mutual respect among team members in addressing issues of health equity in First Nations communities.44–46
The study will examine three sets of outcomes in First Nations families living on-reserve and off-reserve: (1) child developmental health at kindergarten47; (2) parental functioning48 and family connection to health and social services49 and (3) child maltreatment-related outcomes.25
For each of these three sets of outcomes, we will answer the following research questions:
Among First Nations families living off-reserve, what is the relationship between participation in the FFHV programme and the three sets of outcomes compared with non-participating First Nations families living off-reserve?
Among First Nations families living on-reserve, what is the relationship between participation in the SF-MCH programme and the three sets of outcomes compared with non-participating First Nations families living in communities without access to SF-MCH?
In First Nations families living off-reserve, is participation in the FFHV programme associated with reduced inequities in the three sets of outcomes compared with non-First Nations families?
In First Nations families living on-reserve who participate in SF-MCH, is the programme associated with reduced inequities in the three sets of outcomes compared with similar First Nations communities who did not receive SF-MCH?
Data sources
Manitoba boasts a world-class collection of administrative and registry data in the Manitoba Population Research Data Repository at the Manitoba Centre for Health Policy (MCHP). The Repository holds individual-level information for over 99% of the Manitoba population on factors spanning several domains, including health, education and social services.50 This includes information on child developmental health, family functioning and contacts with the healthcare system and social services. Within the Repository is a suite of data files called the PATHS Data Resource,50 which follows individual children born between 1984 and 2014 from the prenatal period into adulthood. The PATHS Data Resource was specifically constructed for conducting intervention-focused health equity research and presents a unique opportunity to engage in cutting-edge population health intervention research. It provides a non-intrusive means for examining the impact of policies and programmes in the real world; it comprises population-based data on virtually all residents of Manitoba (including First Nations individuals), allowing tracking of families living in high-risk conditions who can be lost to follow-up in other research approaches; and it offers a cost-effective means for evaluating the impact of FFHV and SF-MCH on individual children and their families using several years of intervention and follow-up data. Data from the off-reserve FFHV programme are already stored in the PATHS Data Resource; SF-MCH data will be transferred to the Resource as part of ENVISION.
Outcomes: population-level measures of health and health equity
Using de Leeuw and Greenwood’s conceptual framework43 to lend a holistic, family-centred approach to the analyses, we will examine measures of child development using the population-level Early Development Instrument,47 measures of parental functioning using population-level indicators based on those examined by Olds et al,48 including mental disorder diagnoses, substance use, intentional injuries (eg, suicide attempts and completions) and measures of family connection to services (immunisation rates38 and participation in community support programmes).38 51 Child maltreatment is challenging to measure at the population level since only a small fraction of children who experience abuse and neglect come to the attention of health and child protection authorities.16 52 Following from Gilbert et al’s25 use of administrative data as a proxy for measuring child maltreatment at a population level, the maltreatment-related outcomes we will measure include violent deaths, maltreatment-related injury hospitalisations and involvement with child protection agencies. Table 1 provides more detail about each of the population-level measures, including their definitions and data sources. Below, we describe how these measures will be used to evaluate the interventions being studied and to measure health equity.
Population-level measures of child health and family functioning
Interventions
ENVISION will evaluate two home visiting interventions operating in Manitoba. The provincially funded FFHV programme offers home visiting services to at-risk families with children from 0 to 5 years of age who are living off-reserve. Eligibility for the programme is determined by a two-stage process where public health nurses first screen all births (excluding those occurring to women living in First Nations communities) in the postpartum period. Families who score high-risk on the newborn screens are further assessed with a parent survey based on the Kempe Family Stress Checklist53; those with scores≥25 are eligible for the programme. Enrolment in the FFHV programme is entirely voluntary. Under the supervision of public health nurses, paraprofessional trained home visitors develop a trusting relationship with the families in the programme and focus on strengthening parent–child relationships, guiding healthy child development and connecting families with social services54 using the Growing Great Kids Curriculum.55 Earlier evaluations of FFHV showed that the newborn screen was a valid tool for identifying families at risk.49 Using similar methodology (but not focusing specifically on First Nations families), we showed that FFHV was associated with improvements in immunisation rates,38 reductions in maltreatment-related hospitalisations within the first 3 years of life and in the rate of children taken into care in the first, second and third years of life.56 An internal evaluation by the Healthy Child Manitoba Office, which delivers FFHV, has found improved parenting skills, psychological wellness and social cohesion associated with the programme.54 While these evaluations included First Nations families along with other Manitobans, analyses were not run separately for First Nations. The impact of FFHV among First Nations families may differ from the general population since they experience a unique set of contextual and cultural factors. Therefore, it is important to isolate the impact of FFHV among First Nations. Approximately 38% of families involved in FFHV are First Nations living off-reserve.54
The SF-MCH home visiting programme is aimed at expectant mothers and families with infants and young children aged 0–6 living in First Nations communities. Similar to FFHV, enrolment in SF-MCH is voluntary. The SF-MCH programme also uses a screening process to identify the most at-risk families and the programme is delivered by professional supervisors (eg, nurses) and trained paraprofessionals using the Growing Great Kids Curriculum.29 55 Unlike FFHV, SF-MCH is offered to all families who wish to participate, if programme resources (eg, home visitors) are available. SF-MCH builds parenting and family skills to improve family relationships and child development and assists families with gaining access to other community supports and health services. The programme currently operates in 16 First Nations communities and is administered by Nanaandawewigamig. Previous internal evaluations of SF-MCH demonstrate positive influences of the programme on parental outcomes (eg, parenting skills, self-esteem and empowerment), child outcomes (eg, breastfeeding rates) and links to community resources (eg, referrals to specialists).29 57 Through ENVISION, we will now conduct a rigorous external evaluation of SF-MCH.
Data analysis plan
FFHV and SF-MCH are ongoing population health intervention programmes with established programme entry criteria; thus, it was not feasible to randomise participating families and communities to programme exposure and control groups for the purpose of this evaluation. We will use two analytic approaches to examine whether participation in Manitoba’s home visiting programmes is associated with improved health and social outcomes among First Nations families living off-reserve: (1) we will use an interrupted time series analysis to test for differences in rates and trends in rates in each of the outcomes before and after the implementation of the programme; (2) we will use a propensity score analysis to adjust for differences between First Nations families who participate in home visiting and First Nations families who do not, which will allow us to adjust for multiple confounding characteristics simultaneously, with minimal loss of power.58–63
Interrupted time series analysis
Interrupted time series analysis is a powerful, quasi-experimental approach to evaluate the impacts of an intervention over time.64 65 The Repository has longitudinal data spanningmany years before and after the implementation of FFHV and SF-MCH,50 allowing us to test whether changes in the outcomes are associated with the programmes.
Outcomes will be counted annually (for rare outcomes such as hospitalisation for child maltreatment), semiannually (for more common outcomes such as children being taken into care) or quarterly (for common outcomes such as vaccination). Rates will be calculated using generalised linear models with a log-population offset and appropriate distributions (eg, Poisson, negative binomial and so on, depending on the distribution of each outcome) and adjusted for maternal age at first birth to account for changes in the distribution of maternal age over time.50 We will conduct a descriptive analysis of the events for each time point and graph the counts, rates and adjusted rates over time.65
Data from the off-reserve FFHV programme are available from 2003 to 2009 and from the on-reserve SF-MCH programme from 2006 to 2015. The health and social services data in the Repository will allow us to model rates of outcomes from 1991 to 2016. For the off-reserve FFHV programme, we will account for a precursor off-reserve home visiting programme called ‘BabyFirst’, active from 1999 to 2003. In order to have a clean evaluation of the FFHV programme, we will divide the data into segments: (1) before implementation of the FFHV programme in Manitoba (at least eight data points available for each outcome); (2) early years of home visiting during the BabyFirst programme (at least eight data points) and (3) ongoing years of home visiting during FFHV (at least eight data points). We will use segmented regression analysis66 67 with a time variable, indicators for each time segment and an interaction between time and the segment:

where Yt is the outcome at time point t, T identifies the time point, X1 is an indicator for whether or not the observation occurs during BabyFirst (1999–2003); X2 is an indicator for whether or not the observation is from the time period of the intervention being studied. The coefficient on T (time) captures secular trends in the outcome over the entire observation period. The coefficients β2 and β3 test for changes in the outcome when compared with the first time period (eg, β2 tests whether the second time period has a different rate compared with the first time period). β4 and β5 both test whether the outcome’s time trend during the second and third period, respectively, differs from the time trend during the first period.
Segmenting the data for the on-reserve SF-MCH will be simpler, because there was no prior home visiting programme operating on-reserve in Manitoba. For SF-MCH, we will create only two time segments (one for before SF-MCH programme implementation and one for after) with at least eight data points for each outcome in each time segment.
Thus, interrupted time series analysis will allow us to test whether home visiting is associated with different rates in the outcomes and with different time trends for each outcome of interest.66 67 Because of the longitudinal nature of this analysis, we will test for autocorrelation using the Durban-Watson statistic.65 68 We will use the Yule-Walker method if autocorrelation exists.68 We will also test for nonstationarity—whether there is an underlying trend in the outcome not attributable to home visiting—using the Dickey-Fuller test.68 We will use Auto-Regressive Integrated Moving Average modelling in the presence of nonstationarity.69
Propensity score analysis
The propensity score analysis will follow a six-step process:
Select a subsample of First Nations families from the PATHS Data Resource who are eligible for the home visiting programme in question, as measured by the screening tools for each programme (described above).
Divide this cohort into two groups: those who were eligible for and participated in home visiting and those who were eligible for but did not participate.
Develop a logistic regression model to estimate propensity scores for whether or not an eligible First Nations family participated in home visiting with a dichotomous indicator for whether the family participated as the dependent variable. The predictor variables will include a set of measured confounders held in the PATHS Data Resource (eg, maternal age at first birth, smoking, alcohol use—the full list is presented in box 2). Propensity scores will be used to construct inverse probability of treatment weights (IPTWs).70 71
Apply IPTWs to balance the distribution of confounding characteristics between participants and non-participants. We will assess whether participants and non-participants are comparable by examining the standardised differences between the participant groups before and after applying IPTWs to the data.72 An a priori cut-off of a standardised difference <10% will be used to establish that the propensity scores balanced confounding characteristics between exposure groups.72
Apply IPTWs in the outcome models to estimate the adjusted association between programme exposure and each of the outcome variables. These models will compare a group of participants who are similar to non-participants across all measured confounders. Confidence intervals (and p values, where appropriate) will be calculated to indicate statistically significant associations between participation in home visiting and the outcome being considered.
Conduct gamma sensitivity analyses to quantify the strength of unmeasured confounding that would need to be present to explain any statistically significant associations. This analysis allows us to quantify how strongly an unmeasured confounder must influence whether or not a mother–child dyad receives the programme under study in order to undermine our inferences about the programme’s effect on the study’s outcomes; essentially, we will quantify the degree to which any statistically significant associations rest on the assumption that we have adequately adjusted for confounding.73
Risk factors used to balance the study cohort’s sociodemographic characteristics
Family is socially isolated
Parental alcohol and/or drug use
Mother has depression and/or anxiety diagnosis
Mother has antisocial characteristics
Mother has a history of child abuse
Mother has mental disability
Father has antisocial characteristics
Family has a history of disability
Mother has schizophrenia diagnosis
Mother has low educational attainment
Single parent family
No prenatal care before 6 months
No prenatal screening
Mother smoked during pregnancy
Family receives social assistance
Mother was a teen at first birth
High parent survey scores
Socioeconomic factor index II
Violence between parents
Relationship distress
We will synthesise the evidence generated by these two methodological approaches to determine whether Manitoba’s home visiting programmes are associated with improvements in First Nations child health and well-being. Results generated from IPTW analyses will be more sensitive to unmeasured confounding; thus, we will give precedence to findings generated from the interrupted time series analyses.
Equity analyses
Health inequities are conceptualised as unnecessary and avoidable differences in health which are unfair and unjust.73 Classifying differences in health outcomes as ‘unjust’ or ‘unfair’ involves cultural norms which can be difficult to quantify. Consequently, epidemiologists often revert to measuring health inequalities when engaging in health equity research. To examine whether home visiting is associated with reduced health inequities for First Nations families, we will both quantify health equalities and assess whether FFHV and SF-MCH reduced the unfair distribution of health through engagement with our First Nations partners.
FFHV: Health inequalities among off-reserve First Nations families will be measured by calculating the disparity rate ratio and disparity rate difference between First Nations families who participated in FFHV and non-First Nations families for each outcome, and we will compare these with the disparity rate ratio and disparity rate difference between First Nations families who did not participate in FFHV and non-First Nations families. If the disparity rate ratio among participants is smaller than for non-participants (p<0.05), we will conclude that the FFHV programme is associated with reduced inequalities in the outcomes for First Nations families living off-reserve.
SF-MCH: We will conduct two analyses to assess whether SF-MCH is associated with reduced health inequalities among First Nations families living on-reserve. Health inequalities will be measured by comparing the disparity rate ratio and disparity rate difference for each outcome between First Nations families in communities that have access to SF-MCH and First Nations families in communities without access to the SF-MCH programme. When groups do not lend themselves to natural ordering (eg, in the case of income-related inequalities), measuring the variance in health outcomes within and between groups provides another measure of health equity.74 We will measure the variance in outcomes in First Nations communities with SF-MCH and compare this with the variance in outcomes in First Nations communities without SF-MCH. After non-SF-MCH communities have been identified in collaboration with the Nanaandawewigamig knowledge users, we will match them on previously used measures of remoteness75 (distance from the nearest urban centre, whether the community is fly-in, travel time by train and/or by car), resources in the community (presence of schools, nursing stations and other services identified by our partners), cultural continuity as defined by Chandler and Lalonde76 77 and adapted to the Manitoba context through dialogue with First Nations partners and the Tribal Council to which the community belongs, wherever possible. First Nations communities with greater variance in outcomes, after adjusting for community characteristics, are indicative of greater health inequalities. If communities with SF-MCH have both improved outcomes and reduced variance in outcomes, then we will conclude that SF-MCH is associated with reduced health inequalities in First Nations communities.
In addition to evaluating whether FFHV and SF-MCH are associated with reduced inequalities, we will evaluate whether these programmes reduced the unfair distribution of outcomes among First Nations children. To achieve this, we will work with our First Nations collaborators to identify culturally appropriate measures of health equity. Several members of our team have established relationships with First Nations communities and have engaged with community members using an integrated knowledge translation approach. The proposed project will build on this experience to develop health equity measures which are relevant to community members. Team members will travel to First Nations communities to build partnerships and to engage communities in the proposed research. Elders, healthcare providers and other members will be invited to these partnership building meetings.
Ethics and dissemination
Ethical considerations
As much as possible, the evaluations of the FFHV and SF-MCH programmes will align with the OCAP principles.78 OCAP stands for ownership, control, access and possession and are principles that ensure First Nations communities have self-determination over all research involving their people. These principles allow the community to have full decision-making power over what data are collected, how the data will be used, where the data will be stored and how the results will be reported. In the past, much research has been conducted on First Nations peoples without consulting them first, resulting in non-useful findings, erroneous interpretations and a lack of trust between researchers and participants. OCAP ensures research conducted within First Nations communities is culturally appropriate, desired by the community and produces outcomes that will benefit all those involved. The evaluations will comply with the Canadian Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans, specifically Chapter 9: Research Involving First Nations, Inuit and Métis Peoples in Canada.79 Nanaandawewigamig’s Health Information Research Governance Committee and the University of Manitoba Health Research Ethics Board have already reviewed and approved our research plan.
Integrated knowledge translation and dissemination of findings
We are following the Canadian Institute of Health Research guidelines for the development of our integrated knowledge translation (iKT) plan. Our iKT goals are to (1) incorporate the expertise of knowledge users to ensure that the research objectives are meaningful to our intended audience; (2) increase the exposure of the results to policy makers; (3) fill a knowledge gap in evidence for effective prevention programmes for First Nations families living in conditions of risk.
The research design was developed through a series of meetings with knowledge users and study co-investigators. Feedback was obtained regarding objectives, potential methodology and dissemination of results. At least one meeting will be conducted during each phase of the study with coapplicants and collaborators, including an advisory committee comprising First Nations community members and knowledge users. During the active research phase, investigators will work with MCHP data analysts and troubleshoot any data issues that may arise throughout the data analysis process.
The researchers and knowledge users participating in ENVISION will submit abstracts for posters and oral presentations to disseminate research findings at national and international conferences. We will also write and submit publications to peer-reviewed journals that publish studies on population health intervention research. STROBE and RECORD statements will guide transparent reporting practices. To ensure the widespread dissemination of the results outside the academic community, we are also collaborating with the Evidence Network of Canadian Health Policy to make the latest evidence on health research available to the media. We will develop lay summaries and infographics of the results to be disseminated at a community level and to data providers to inform them how their data were used to improve the health and well-being of Manitoba First Nations families. Finally, we will brief government and First Nations partners on the findings. This study is expressly aimed to provide high-quality evidence about the effectiveness of home visiting programmes for First Nations families that can help policy-makers and programme developers make informed decisions about programme implementation and delivery.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.
- 83.
Footnotes
Contributors Led by MDB, NCN and JEE, all authors were involved in the conception of the research and contributed to writing the Canadian Institutes of Health Research grant proposal that funds this work. RS, WP-B and RC provided context for the proposal from their perspectives as program funders and administrators, respectively. This manuscript was drafted by MDB, JEE and NCN and critically reviewed by all other authors.
Funding This work was supported through a Canadian Institutes of Health Research Operating Grant in Population Health Intervention Research to Promote Health and Health Equity, with sponsorship from The Institute of Population and Public Health and the CIHR Pathways to Health Equity for Aboriginal Peoples Initiative in partnership with the Saskatchewan Health Research Foundation (grant number GI1-145122).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.