Article Text

Abstract
Objective Reconfiguration of trauma services, with direct transport of patients with traumatic brain injury (TBI) to specialist neuroscience centres (SNCs)—bypassing non-specialist acute hospitals (NSAHs), could improve outcomes. However, delays in stabilisation of airway, breathing and circulation (ABC) may worsen outcomes when compared with selective secondary transfer from nearest NSAH to SNC. We conducted a pilot cluster randomised controlled trial to determine the feasibility and plausibility of bypassing suspected patients with TBI —directly into SNCs—producing a measurable effect.
Setting Two English Ambulance Services.
Participants 74 clusters (ambulance stations) were randomised within pairs after matching for important characteristics. Clusters enrolled head-injured adults—injured nearest to an NSAH—with internationally accepted TBI risk factors and stable ABC. We excluded participants attended by Helicopter Emergency Medical Services or who were injured more than 1 hour by road from nearest SNC.
Interventions Intervention cluster participants were transported directly to an SNC bypassing nearest NSAH; control cluster participants were transported to nearest NSAH with selective secondary transfer to SNC.
Outcomes Trial recruitment rate (target n=700 per annum) and percentage with TBI on CT scan (target 80%) were the primary feasibility outcomes. 30-day mortality, 6-month Extended Glasgow Outcome Scale and quality of life were secondary outcomes.
Results 56 ambulance station clusters recruited 293 patients in 12 months. The trial arms were similar in terms of age, conscious level and injury severity. Less than 25% of recruited patients had TBI on CT (n=70) with 7% (n=20) requiring neurosurgery. Complete case analysis showed similar 30-day mortality in the two trial arms (control=8.8 (2.7–14.0)% vs intervention=9.4(2.3–14.0)%).
Conclusion Bypassing patients with suspected TBI to SNCs gives an overtriage (false positive) ratio of 13:1 for neurosurgical intervention and 4:1 for TBI. A measurable effect from a full trial of early neuroscience care following bypass is therefore unlikely.
Trial registration number ISRCTN68087745.
- Organisation Of Health Services
- Neurological Injury
- Neurosurgery
- Trauma Management
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Head injury transportation straight to neurosurgery (HITS-NS) has rigorously sampled the preimaging head injury population that paramedics encounter and select for bypass according to clinical suspicion of traumatic brain injury (TBI) at the scene—unlike earlier postimaging studies.
HITS-NS pragmatic inclusion criteria selected head-injured patients with internationally accepted high-risk indications for TBI.
Bias was further avoided by the cluster randomised design whereby ambulance stations were preallocated to intervention and control.
The inclusion criteria differed by one Glasgow Coma Scale point between the two ambulance services to allow consistency with their major trauma bypass protocols.
Non-adherence was common in the intervention group due to lower study training resources in the larger ambulance service.
Background
The National Institute of Health and Care Excellence (NICE) 2007 and 2014 Head Injury Guideline revisions suggested that all patients with ‘severe head injury’ (abnormal CT brain scan suggesting traumatic brain injury (TBI) and arriving at the first hospital intubated or with a Glasgow Coma Scale (GCS) of <9 should be treated at or transferred to a specialist neuroscience centre (SNC).1 2 Consequently the current National Health Service (NHS) England reconfiguration of trauma services—with direct transportation of patients with head injury suspected to have TBI to SNCs bypassing nearer non-specialist acute hospitals (NSAHs)—could potentially improve outcomes by expediting neurosurgical intervention. The proportion of patients with TBI receiving SNC care could also be increased by bypass as not all are subsequently accepted for secondary (NSAH to SNC) transfer.3 This guidance is also reflected in international guidelines for TBI produced in Scotland,4 the USA and New Zealand.5 6 These guidelines vary in the stated indications for SNC care, largely due to the lack of a substantive evidence base.
However, delays in stabilisation of airway, breathing and circulation (ABC) and the difficulties in reliably identifying TBI at the scene of injury may worsen outcomes when compared with later selective secondary transfer from nearest NSAH to SNC.7 8 Delays in correcting hypoxia and hypotension associated with longer journeys to hospital for unconscious patients could worsen outcomes through secondary brain injury—particularly where patients are treated by prehospital practitioners who cannot provide a definitive airway.7 The occult nature of TBI could also mean that large numbers of patients are taken significant distances past their nearest hospital for no benefit (overtriage).8
Prior to our study two systematic reviews of trauma bypass had been conducted, one with a focus on head injury. These reviews synthesised observational studies using hospitalised patients with TBI as a denominator—rather than the unselected head injury population that present to Emergency Medical Services (EMS). Hence they are of questionable external validity, furthermore studies included patients whose nearest hospital was a SNC (no bypass required) and therefore lack internal validity. Not withstanding this, the meta-analysis did not suggest benefit from ‘bypass’ in the TBI population.8
The evidence base suggested equipoise and highlighted poor quality evidence with regard to the clinical and cost-effectiveness of early neurosurgery through bypass in this cohort. We sought to address this by establishing the feasibility of a cluster randomised trial to determine the impact of early neurosurgery through bypass in patients with head injury with suspected TBI injured nearest to an NSAH. The major feasibility considerations being a sufficient recruitment rate of patients with TBI on CT brain scan (enabling more precise early neurosurgery effect estimates), protocol adherence and acceptability of the trial to patients and staff.
Methods
The pilot cluster randomised controlled trial of bypass to SNC for early neurosurgery was conducted in two English ambulance services, Lancashire/Cumbria in the North West Ambulance Service (NWAS) and the North East Ambulance Service (NEAS) with the ambulance station (n=74) as unit of cluster. Ambulance stations were randomised within ambulance services using matched pairs by the trial statistician using a computer-generated sequence (JF). Pairs of ambulance stations were matched for number of full time ambulances in operation and median distance to nearest SNC and NSAH prior to randomisation by the head injury transportation straight to neurosurgery (HITS-NS) trial manager (WR). Prior to study roll out all paramedics in study clusters (and emergency medical technicians in NEAS) were trained in study inclusion criteria and procedures by study research paramedics and senior ambulance service personnel. Each ambulance station cluster remained within its original allocation for the duration of the feasibility pilot. As the study of early neurosurgery was being facilitated by hospital bypass, it was effectively ‘open label’. However the mortality outcome assessor was blinded to study allocation. Further details are described in online supplementary appendix 1; the Research Ethics Committee (REC) approved protocol.
Supplementary file 1
Head-injured adult patients with risk factors for TBI (GCS <13 in NWAS, GCS <14 in NEAS—to fit with different major trauma bypass criteria—see online supplementary appendix file 1) and stable ABC, injured nearest to an NSAH were transported either to that closest hospital (control clusters) with selected patients subsequently undergoing secondary transfer to a SNC, or bypassed with direct transport from scene of injury to the nearest SNC (intervention clusters). Paramedics were also able to enrol patients with rarer findings such as focal neurology and obvious skull fracture or their own clinical concern (see online supplementary appendix file 1 for study protocol). Eligible patients attended by Helicopter Emergency Medical Services or transported by other Ambulances Services into study hospitals were excluded as were patients injured more than 1 hour from the nearest SNC by land ambulance. The study was conducted between January 2012 and September 2013 with the majority of recruitment occurring from April 2012 to March 2013.
Study inclusion criteria were based where possible on high-risk criteria for TBI in patients with head injury1 2 from established Emergency Department Clinical Decision Rules for selecting patients with head injury for CT brain scan.1 2 However three of the indications for CT specified in these rules cannot be reliably applied at the scene of injury as they require observation of the patient for up to 2 hours after the incident. Inevitably this meant that the predominant indication for study enrolment was an impairment of consciousness as measured by the GCS. We estimated a study TBI (TBI or complex skull fracture detected on CT brain scan) prevalence of 80% in patients with GCS <13, supported by analyses of the Trauma Audit and Research Network (TARN) data (O Bouamra, personal communication, 2012).
During study roll out, the two ambulance services introduced major trauma bypass protocols for patients with ‘non-TBI’, that is, injured patients not meeting HITS-NS inclusion criteria. The major trauma bypass eligibility criteria differed by one GCS point (<13 in NWAS <14 in NEAS) between study ambulance services. The HITS-NS TSC and ambulance services advised study investigators to incorporate these differences into study inclusion criteria in NEAS and NWAS to avoid confusion (see merged protocol in online supplementary file 1), REC approval was given for this amendment to the original study GCS inclusion criterion in NEAS.
The primary feasibility targets were the recruitment rate (700 patients—80% (n=560) with TBI on CT scan equivalent to 20% or 1:4 overtriage ratio) and protocol adherence (90%). We also assessed any patient factors associated with protocol non-adherence and the trial’s acceptability to patients, their families and staff.
The secondary outcomes were those that would form the primary outcomes of a fully powered trial: 30-day mortality, 6-month Extended Glasgow Outcome Scale (GOSE)9 and the Euro QoL5-D (EQ-5D).10
Non-parametric descriptive statistics (medians and IQRs) were used to summarise patient variables in each trial arm, (missing variables were not imputed). Characteristics between groups were then compared by examining the difference with associated 95% CIs.
Sample size
We aimed to recruit 700 patients across the 2 ambulance services over 12 months. This was based on our full trial power calculation which for a 3-year full trial indicated that (3×1400) 4200 patients would have 80% power to detect an absolute 5% change in rate of poor outcome (two-tailed for 6 month GOSE <5) assuming a 30% event rate, an intracluster correlation coefficient of 0.02% and 5% risk of type 1 error. The full trial would take place in approximately 120 clusters in 4 ambulance services. The sample size target was half the required annual recruitment rate as in the pilot we recruited from two ambulance services (ie, 50% of possible clusters).
Ethics and governance
As altered conscious level formed part of our inclusion criteria, it was not possible to obtain informed consent for the trial from HITS-NS patients at the scene of injury. Consent for research in this situation is covered by the Mental Capacity Act Section 32[9] in England. Hence we obtained ethical approval to enrol patients into the trial at scene with later consent for follow-up and inclusion of data (10/WNo03/30—further details in appendix).
The conduct of HITS-NS and interim analyses were overseen by an Independent Trial Steering Group which was informed by an independent Data Monitoring and Ethics Committee (DMEC).
Results
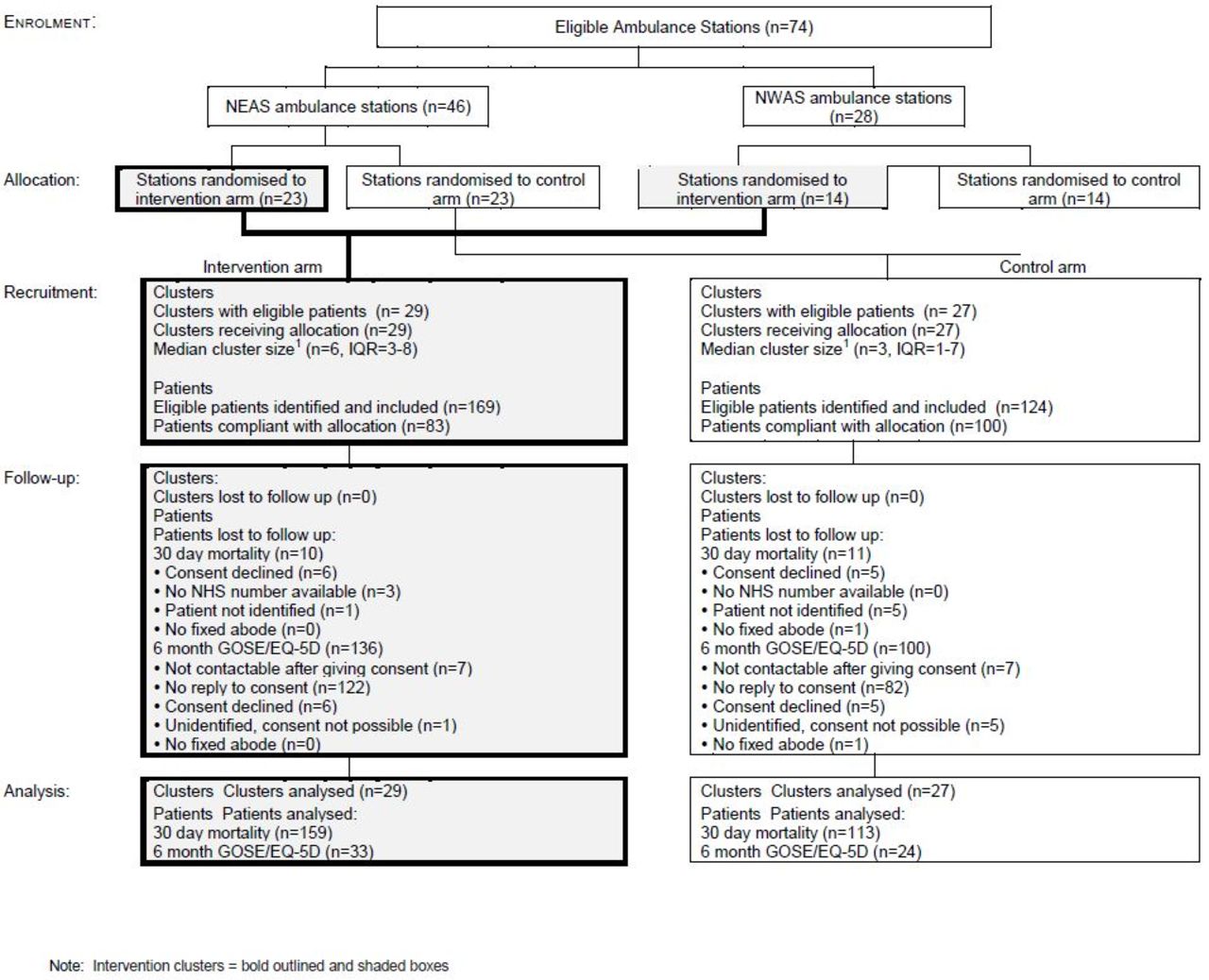
The study consort diagram (figure 1) shows that 56 clusters recruited 293 patients in 12 months. Rigorous screening of over 65 000 ambulance service records indicated that the remaining 18 clusters did not see eligible patients. Overall adherence from the paramedics in terms of taking patients to the hospital, their cluster was randomised to was (183/293) 62% but achieved (100/124) 80% in the control arm (figure 1). Non-adherence was significantly associated with estimated driving time to the SNC in both trial arms and with (5.2%) lower overall injury severity and (23% lower) prevalence of TBI in the intervention arm (p<0.05), there were no other differences between the populations in which the allocation was/was not complied with (see web online supplementary appendix 2 tables (i) and (ii)).
Supplementary file 2
{kind=link}
Study consort diagram. EQ-5D, Euro QoL5-D; GOSE, Extended Glasgow Outcome Scale; NEAS, North East Ambulance Service; NWAS, North West Ambulance Service.
Patients in the control and intervention groups were similar in terms of both factors the paramedics at scene would and may not have been aware of (tables 1 and 2) including age (median age: 45 (IQR 30–70) vs 49 (IQR 30–65) years, invention vs control), median GCS (12 (IQR 8–13) in both groups) and median overall severity of injury (median ISS=1 in both groups, intervention IQR,1–9 control IQR1–16). The 30-day mortality rates were similar in the control and intervention groups (8.8 (2.7–14.0)% vs 9.4 (2.3–14.0)%) in the 272 patients with data available.
Basic clinical data: factors apparent at scene of injury
Basic clinical data: factors not necessarily apparent at scene of injury
Less than a quarter of recruited patients had TBI on CT brain scan (70 out of 293, 24%) with 7% (n=20) requiring neurosurgery (craniotomy, elevation of bone flap or intracranial pressure (ICP) monitoring±subsequent surgery) and a further 6% (n=18) requiring admission to an intensive care unit (ICU). This equates to a 4:1 overtriage ratio for TBI and 13:1 for neurosurgery. Very low response rates to postal ‘opt in’ invitations to consent for follow-up in the large number of mild head injury enrolled patients meant only 20% of patients had 6-month disability outcomes or satisfaction questionnaires (data not shown). The rates of recruitment, adherence and most importantly of TBI/need for neurosurgery were below the prespecified feasibility requirements. It was not possible to generate an ‘effect estimate’ of early neurosurgery from the trial data due to the small numbers who required any neurosurgical intervention.
Discussion
To our knowledge HITS-NS is the world’s first trial that randomised patients to different hospitals from the scene of injury. The important new finding of the low rate of TBI (<25%) and requirement for neurosurgery (<10%) in the head injury population eligible for trauma bypass—means that the potential effect of the intervention (early neurosurgery) is diluted. A meaningful effect from the intervention is thus unlikely to be plausible or detectable, even in a large trial. The total number of study patients enrolled with TBI, minor head injury and other pathologies (n=293) and rates of protocol adherence (62%) also fell below prespecified feasibility targets.
The inclusion criteria for HITS-NS are typical of current Trauma Triage Tools.11 12 Hence by extrapolation, current EMS bypass practice of suspected patients with TBI to SNCs results in overtriage ratios of 13:1 for neurosurgery and 4:1 for TBI.
The major barrier to a full trial of early neurosurgery by bypass is the low numbers and prevalence of patients with TBI or who need neurosurgery within the study cohort. This could not have been predicted by existing evidence at the time of study design but is an important finding from the study. Prior to conducting the trial the investigators established that 80% of patients with on scene GCS <13 on the TARN database have a TBI on CT scan. However the TARN denominator population now appears to differ significantly from those with GCS <13 at scene because of the TARN eligibility criteria3 which most of the recruited HITS-NS study cohort did not meet (surviving patients with head injury need to stay in hospital >72 hours or need critical care to be included on TARN). The predominant injury within the study cohort was mild head injury with normal CT brain scan and discharge from hospital within 24 hours of presentation; this was true even in the GCS <13 subgroup where >65% had no TBI on CT. The likely explanation for these discrepant findings are short-term depressors of the conscious level such as alcohol which is consistent with the median age of patients (45 and 49 years in intervention and control), predominant mechanism of injury being falls and male gender preponderance. The study inclusion criteria were consistent with NICE high-risk criteria for identifying patients with TBI in Emergency Departments who require neurosurgery and therefore urgent CT scan. However these criteria also require observation of patients with GCS of 13–14 for 2 hours after injury. Hence they cannot be fully applied at the scene of injury.1
Protocol adherence in the intervention clusters within NEAS was limited and was a result of the same training resource (a single study coordinator) being available for each ambulance service for pragmatic reasons at this feasibility stage. In reality this made the face-to-face training that achieved almost 90% adherence in NWAS impossible in NEAS—due to its greater numbers of paramedics and larger geographical area; electronic media and cascade from team leaders were relied on instead.13 However had rates of TBI been sufficient we would not see this as a barrier to a full trial as it could be addressed by increasing resources for training.
The REC directive of an active opt in for being approached for telephone consent in early discharge study patients limited meaningful follow-up of the study cohort beyond 30 days postinjury. This has been highlighted in the literature as a persistent problem in this mild head injury group.14 Again we believe that this could have been addressed in a full trial by using the evidence gathered as part of this pilot to demonstrate (to the REC) the value of allowing an opt out approach—which has been used successfully elsewhere.15
This evaluation is consistent with the systematic review of bypass, referred to earlier, which did not indicate benefit for patients with TBI (although from studies with questionable validity as purely patients with TBI, rather than scene of injury ‘head injury suspected patients with TBI’ were included). However this current feasibility evaluation was not powered to detect clinically significant effects.
Recent publications suggest that although the study inclusion criteria may be sensitive for ‘moderate to severe TBI’—as defined by a GCS <13 significant numbers of patients with TBI visible on CT scan present with an initial GCS of 14–15.12 Many of these patients require neurosurgery although less urgently than those with a lower conscious level.12 A second paper from NEAS suggests that the HITS-NS inclusion criteria are 95% specific when applied to head-injured patients at the scene where the prevalence of TBI is low at 5%.13 Hence the below target HITS-NS TBI prevalence of 24% (low positive predictive value of study inclusion criteria/high overtriage rate) is driven by low ‘scene head injury TBI prevalence’ and limited ‘all TBI’ sensitivity, in addition to imperfect HITS-NS specificity.
This challenging ‘high initial GCS’ TBI population is likely to mainly include older adult fallers with head injury. A recent study suggested that >50% of all patients over 65 with TBI have a scene GCS recorded as 15.16 Age-related cerebral atrophy is a putative explanation perhaps allowing early intracranial bleeding postinjury without the concomitant rise in ICP that lowers GCS. A second group are younger patients with extradural haematomas who require neurosurgery but have a median GCS of 14 on presentation.17 Our findings suggest that the majority of patients with head injury attended by EMS are mildly disorientated or fully conscious at the scene (GCS 14–15) and do not meet HITS-NS study inclusion criteria , hence the below target recruitment rate (n=293 vs 700). However solely raising the GCS threshold for bypass would not make an evaluation of early neurosurgery feasible as specificity for TBI would fall significantly. Study numbers could increase, but the TBI study prevalence would reduce further.12 13 Conversely more restrictive inclusion criteria (a lower GCS cut-off) may increase specificity but will reduce sensitivity and numbers of patients with TBI recruited further.18 Hence it does not appear possible to study sufficient numbers of bypassed patients with TBI within the context of a controlled trial—due to the challenges of reliably identifying TBI in head-injured patients at the scene.
The lack of current trauma triage criteria which are both sensitive and specific enough for optimum system functioning have been highlighted elsewhere but mainly with regard to all major trauma rather than head injury per se, however, within the NHS 75% of all major trauma victims (defined as an injury severity score of >15) have a TBI.19
We observed that study mortality was relatively high (25/273=9.2%) for a population with a low severity of injury—and that only 12 out of 25 deaths occurred in the context of TBI on CT; the remainder occurring as a result of medical conditions or elderly frailty. The latter are not amenable to specialist neuroscience care.
Current trauma reconfiguration for head injury—where bypass is now standard practice for patients meeting the HITS-NS inclusion criteria—has been implemented based on extremely limited research evidence and implicit expert opinion. The low numbers of patients in the HITS-NS cohort requiring neurosurgery suggests that this decision may not result in effective or cost-effective care. However, given that bypass is now standard care, further challenging research is required for evaluating the key trauma system questions of which patients with TBI definitely benefit from SNC care, and how to reliably identify TBI in the prehospital environment.2 3
It may now be possible to conduct a further evaluation of ‘early neurosurgery through bypass’ in patients with TBI using registry (TARN) data and a comparative effectiveness or case control design. Until now this has not been possible in the pre ‘trauma system’ climate in which HITS-NS was conceived and no land ambulance bypass was occurring. In the interim, secondary transfer to neurosurgery will remain a necessary pathway for patients with TBI injured nearest to an NSAH with a high (GCS >13) level of consciousness at the scene.
Acknowledgments
The authors would like to acknowledge the help and support of the following: Professor Jonathan Benger who chaired the HITS-NS Trial Steering Group and the independent members Alastair White and Mike Page. Professor Helen Snooks who chaired the HITS-NS Data Monitoring and Ethics Committee and the independent members Professor Peter Hutchinson, Dr Simon Gates and Dr Rod Mackenzie. All the staff in NEAS, NWAS, the Royal Victoria Infirmary Newcastle, James Cook University Hospital Middlesboro, the Royal Preston Hospital, HITS-NS 8 acute hospital trusts, Lancashire and South Cumbria, Durham and Tees Valley and Newcastle Tyne and Wear CLRNs, who helped in making this challenging study possible. Laura White, Tom Jenks and Thomas Stacey from the Trauma Audit and Research Network (TARN) for their expertise and support with data collection, coding and management. Antoinette Edwards from TARN for creating and developing the HITS-NS website. Joanne Hinde for assistance in report preparation and administration. Hannah Newcombe and members of Salford and Trafford Headway for developing the HITS-NS patient satisfaction questionnaire. Staff from the University of Manchester, Greater Manchester CLRN and the North Wales REC NW10 who assisted with research governance/study amendments.
References
Footnotes
Contributors FEL, SG, SM, TC, KM-J, AC, KH and GF are emergency physicians with expertise in prehospital/trauma research. FEL was HITS-NS lead applicant/chief investigator. FEL led in the conduct of the cluster randomised trial, chaired the Trial Management Group (TMG), wrote the HITS-NS report and paper. GF conducted a cost effectiveness analysis. GM and EP are paramedics who were employed full time during recruitment and coordinated HITS-NS in NEAS/NWAS (paramedic training, study role out, patient screening, identification, consent and data collection) supervised by WR the HITS-NS trial manager, SB and MP the ambulance service R&D leads, and KH and KM-J the ambulance service medical directors. AC and KH were Principle Investigators (PI) at two (Royal Preston, James Cook) of the three neuroscience centres, DH a neurosurgeon was PI at the Royal Victoria Infirmary in Newcastle. WR managed all aspects of HITS-NS, wrote interim HTA reports. NC, University of Sheffield medical student, studied the conduct of HITS-NS as his B Med Sci intercalation and took part in the TMG. JF is an experienced statistician who conducted the cluster randomisation, study analyses in the manuscript and interim analyses for the DMEC. All the aforementioned, along with JS the Yorkshire Ambulance Service R&D Director, took part in the TMG. The majority were coapplicants on the original 2008 application. HP a personal injury solicitor and secretary of Salford and Trafford Headway was an applicant and took part in the TSG—leading on patient and public involvement in the review of progress, information sheets and satisfaction questionnaires—and representing Headway. All authors have viewed and contributed to the writing of this report.
Funding The study was funded by the National Institute of Health Research Health TechnologyAssessment Programme HTA08/116/85. GF was also supported by an NIHR Doctoral Research Fellowship.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval North Wales REC 10.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement HITS-NS data are available upon request from the corresponding author.