Article Text

Abstract
Introduction There is a growing proportion of population aged 65 years and older in low-income and middle-income countries. In Malaysia, this proportion is predicted to increase from 5.1% in 2010 to more than 15.4% by 2050. Cognitive ageing and dementia are global health priorities. However, risk factors and disease associations in a multiethnic, middle-income country like Malaysia may not be consistent with those reported in other world regions. Knowing the burden of cognitive impairment and its risk factors in Malaysia is necessary for the development of management strategies and would provide valuable information for other transitional economies.
Methods and analysis This is a community-based feasibility study focused on the assessment of cognition, embedded in the longitudinal study of health and demographic surveillance site of the South East Asia Community Observatory (SEACO), in Malaysia. In total, 200 adults aged ≥50 years are selected for an in-depth health and cognitive assessment including the Mini Mental State Examination, the Montreal Cognitive Assessment, blood pressure, anthropometry, gait speed, hand grip strength, Depression Anxiety Stress Score and dried blood spots.
Discussion and conclusions The results will inform the feasibility, response rates and operational challenges for establishing an ageing study focused on cognitive function in similar middle-income country settings. Knowing the burden of cognitive impairment and dementia and risk factors for disease will inform local health priorities and management, and place these within the context of increasing life expectancy.
Ethics and dissemination The study protocol is approved by the Monash University Human Research Ethics Committee. Informed consent is obtained from all the participants. The project's analysed data and findings will be made available through publications and conference presentations and a data sharing archive. Reports on key findings will be made available as community briefs on the SEACO website.
- Ageing cohort; health and demographic surveillance; chronic illness monitoring; cognitive function
- PUBLIC HEALTH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Ageing cohort; health and demographic surveillance; chronic illness monitoring; cognitive function
- PUBLIC HEALTH
Introduction
Cognitive ageing and dementia are global public health priorities. The number of people living with dementia globally is predicted to increase from 46.8 million in 2015 to 74.7 million in 2030 and 131.5 million in 2050; and more than 70% of them will be from the low-income and middle-income countries.1 Malaysia is undergoing a rapid demographic transition. It is projected that, by 2050 the older aged population, defined as persons aged 65 years and older, will make up 15% of the country's population.2 This change in age structure will lead to an unprecedented increase in the number of people living with cognitive impairment and dementia and will have significant personal, financial and social impacts.
Malaysia is a multiethnic country with wide cultural diversity.3 Also, it is a very fast growing and transitional economy. Indeed, by 2020 it is projected that Malaysia will transition to a high-income country. Owing to these reasons, the prevalence and risk factors of dementia and cognitive impairment may not be consistent with those reported in other world regions.
The prevalence estimates of dementia in developed countries range from 4.7% to 7.2%.4 Few prevalence studies of dementia and cognitive impairment have been conducted in Malaysia and most have been undertaken in small non-representative samples (table 1). No research has been conducted on incidence. Where assessed, the prevalence of cognitive impairment and dementia, typically defined using Mini Mental State Examination (MMSE) cut-off scores or the Elderly Cognitive Assessment Questionnaire (ECAQ), has been found to range from 2.5% to 36% (table 1).
Summary of findings from prevalence studies of dementia and cognitive impairment in Malaysia
Risk factors for cognitive impairment have included age, sex, educational attainment and ethnicity.5 ,6 ,8 ,9 ,12 However, the link between health and cognition has been poorly explored in the community-based settings. Results from studies that have explored health cognition associations have been mixed including no association between body mass index or hypertension and cognitive impairment12 or dementia,9 an association between dementia and occupational pesticide exposure and history of stroke in a outpatients setting.10 In a community sample, cognitive impairment was not found to be associated with hypertension,7 while in another study dementia was found to be associated with cardiovascular illnesses defined as a combination variable including hypertension, diabetes mellitus, ischaemic heart disease, hyperlipidaemia and stroke.15 A more in-depth investigation of cardiovascular and metabolic risk factors in addition to assessment of other health and lifestyle factors, which are known risks for dementia; needs to be undertaken in the Malaysian population.
The main difficulties in conducting dementia studies in Malaysia have been limitations in assessment methods including a lack of availability of translations of commonly used cognitive screening tests, lack of normative data, literacy/educational attainment biases and lack of tests that are sensitive to ethnic differences (Malays, Chinese and Indians). This project will redress these through the development and piloting of a neuropsychological battery incorporating various cognitive assessment tools that have been validated in similar settings.
Knowing the burden of cognitive impairment and dementia and their risk factors in Malaysia will be necessary for the development of treatment and prevention strategies and to inform public health policies focused on an ageing population. Therefore, the objective of this study is to evaluate the feasibility of detailed cognitive and health assessment using a set of cognitive battery specifically designed to assess cognition in Malaysia. The long-term aim is to develop a comprehensive epidemiological research platform for investigating cognition and dementia in Malaysia, and, thereby, maximise the number of years free of cognitive impairment and dementia. This research platform will then provide a unique resource for studying ageing during economic transition and across ethnic and religiously diverse groups.
Objectives
To assess the feasibility and acceptability of a tablet-based neuropsychological battery, to screen for cognitive impairment and dementia in individuals aged 50 years and over within a health and demographic surveillance site in Malaysia.
To assess the feasibility and acceptability of collecting physical measurements including gait speed, hand grip strength, single lead ECG and dried blood spots (DBS).
To assess the feasibility of establishing an ageing cohort in order to monitor incidence of dementia, cognitive decline and other ageing-related health risks.
Methods and analysis
Participants
This study is embedded within the South East Asia Community Observatory (SEACO) population.16 SEACO is a health and demographic surveillance site (HDSS); a unique research platform in population health and well-being focused on a middle-income community in Segamat, Johor in the southern tip of the Peninsular Malaysia. The district of Segamat comprises urban, rural and plantation areas with an ethnic mix including Malays, Chinese and Indian, close to national proportions. SEACO runs its HDSS research platform in five subdistricts (mukims) of the Segamat district: Bekok, Chaah, Gemereh, Jabi and Sungai Segamat. In total, 38 228 individuals completed the baseline census (March 2012 to February 2013) that included information on sociodemographic status and self-reported health conditions. Data were collected by trained interviewers at the person's place of residence. Individuals have been reseen after a year (August 2013 to June 2014) for the health round, which collected a detailed health profile of all the consenting participants.
Individuals aged 50 years and over, who are living in Segamat Johor and have been assessed as part of SEACO in its previous health round form the study population. Nearly 9000 individuals meet these inclusion criteria. Baseline data from the census, update and health rounds are used to identify participants for inclusion. Persons are excluded if they cannot communicate effectively, have severe hearing loss or visual impairment (ie, are unable to hear normal conversation and/or not able to see the newsprint), are untraceable or are unable to give consent. From the eligible population, 200 samples are selected by stratified random sampling. The target is to recruit 200 participants stratified by age (50–59 and ≥60 years) and gender, with equal numbers in each group. Participants are also stratified based on their ethnicity (Malay, Chinese, Indian and Orang Asli) to ensure that each group is represented proportionately to the composition of the elderly population of SEACO as shown in figure 1. Stratified sampling is used in order, not to miss any of these strata in the relatively small sample, so that operational issues across all the groups are captured. The SEACO health round data base is used as the sampling frame.
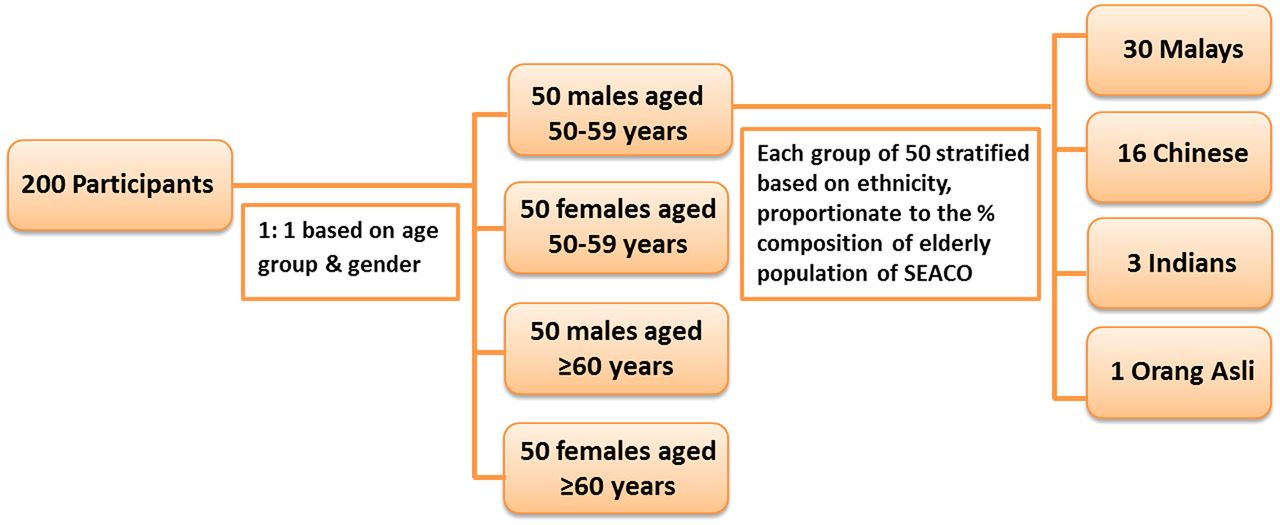
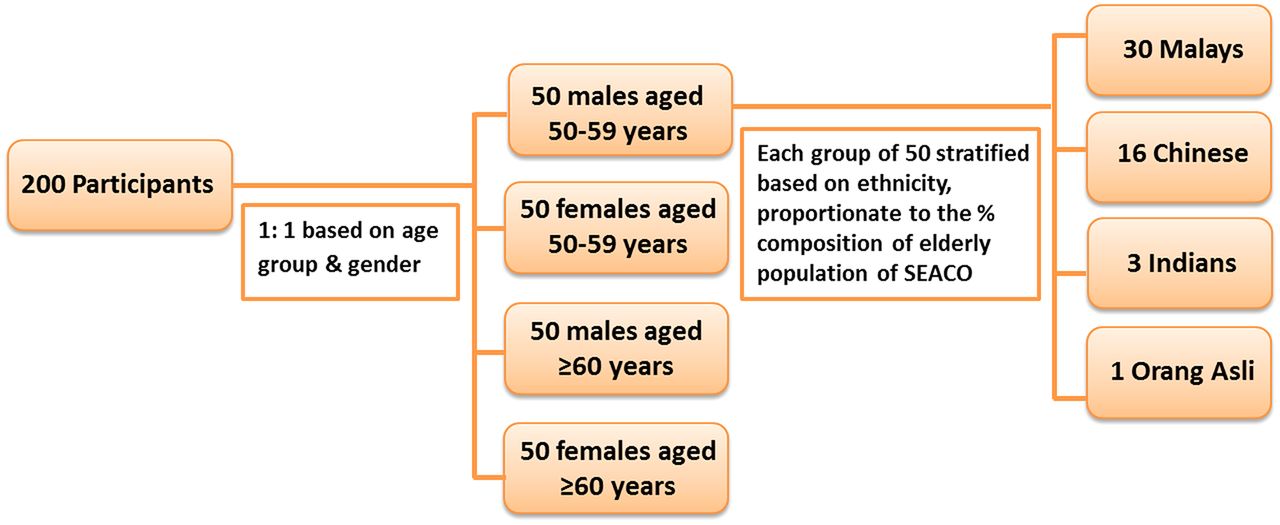{kind=link}
Stratification grid used for selecting the feasibility study samples from the SEACO population. SEACO, South East Asia Community Observatory.
Data collection
A home visit will be conducted to confirm eligibility, provide an information sheet, discuss any questions and to make an appointment for data collection. On the appointment date informed consent will be obtained. All interviews will be conducted in Bahasa Malay or Chinese according to the participant's choice. All data are collected on a Tablet (Samsung Galaxy Tab 3 V), unless otherwise specified. The assessment interview will take ∼1.5–2 hours to complete. The ordering of the measures will be standardised for all participants and will include:
Blood pressure (BP): resting BP will be measured in triplicate using an Omron electronic BP monitor. Participants will be resting in a seated position for at least 10 min before the measurement, and the three measurements will be taken 1 min apart.
Anthropometry: height and weight will be measured with a combined electronic scales and laser height measurement device. The participant will be barefoot and wearing light clothing.
Neuropsychological battery: the neuropsychological battery consists of four components:
Subjective memory compliant: a single item will ask participants: Do you have problems with your memory? (Possible answers are: ‘NO’ OR ‘YES’)? If they answer yes they will be asked additional questions about memory loss in the previous year; and memory in comparison to other of same age
Subjective memory symptom from the relative/caretaker: a close relative/caretaker will be asked a single question on problems with memory of the participant in the past year relative to previous years with possible answers: ‘NO’ OR ‘YES’.
MMSE: depending on the language chosen for interview by the respondent, the Malay (MMSE-7), or Chinese version will be used to screen for severe cognitive impairment. The Malay version was validated by Norlinah and colleagues among multiethnic elderly attending two hospitals in Kuala Lumpur.17 The Chinese version was validated among a Chinese population in Singapore.18 Scores range from 0 to 30, with higher scores indicating better global cognitive functioning.
Montreal Cognitive Assessment tool (MoCA) will be used to screen for milder forms of cognitive impairment.19 The Singapore Chinese20 or Bahasa Malay version21 will be used, based on the language of interview of the participants.
All the components of cognitive assessment will be administered using tablet, except MoCA, which will be administered in paper form. XLS Form will be used to create the questionnaire on the tablet, and this will be developed in consultation with the SEACO IT team. All MMSE questions, the tasks and the images (along with the rest of the questionnaire) will be incorporated into the form. Data collector will administer the tool and will enter the participant responses and scores for each question. The form will be programmed to calculate the total score (out of 30) for the participant once the data collector finishes administering the MMSE. This score will help the data collector to decide on need for referral.
Functional performance: two tests will be used to assess functional performance including: handgrip strength assessed in both arms (in duplicate) using a portable dynamometer; and, gait speed, which measures using a stop watch, the time it takes a participant to walk over a 4 m distance at their usual pace. The respondent will be asked to walk a distance of 6 m while the stop watch recording starts only at the end of the first 1 m and is stopped at the end of fifth meter of walk. In the field this is done using a foldable custom-made device colour coded for easy understanding. The participant will also be asked about the history of imbalance on walking.
Health and lifestyle questionnaire: participants will be asked to complete a questionnaire including the following:
Information on self-rated health status: self-rated health will be measured by the question ‘How would you rate your current health?’ and the response will be captured in a five-point Likert scale of very poor, poor, neither poor nor good, good and very good.
Global Activity Limitation Indicator (GALI)22 which underlies the European Healthy Life Years indicator includes a single item that asks ‘For the past 6 months at least, to what extent has you been limited because of a health problem in activities people usually do?’
Activities of daily living measured using Katz Index of Activities of Daily Living (adapted version).23
Lifestyle factors including tobacco and alcohol use—tobacco use: the participant will be asked if he or she has ever smoked, history of current smoking, age of initiation, type of tobacco product used, number of cigarettes smoked and attempts to quit. Alcohol use: single item asking ‘Have you consumed alcohol in the past 30 days?’
Self-reported exhaustion—a single item asking ‘Have you felt that everything you did was an effort/you could not get going—for at least 3 days during the last week?’
Level of activity—two items asking: (1) ‘How often in the last week did you engage in moderate activities like gardening, cycling or going for a walk?; and (2) Do you engage in at least 150 min of moderate-intensity aerobic physical activity throughout the week?’
A history of diagnosed conditions such as stroke, ischaemic heart disease, transient ischaemic attack, heart failure, hypertension, diabetes (type 1 or type 2) and cancer.
Depression Anxiety Stress Scores.24
Dry blood spot collection and blood glucose testing: four drops of blood will be collected on blood spot card (Whatman 903), under strict aseptic precaution. The DBS will be packed with desiccant packs and barcode labelled. The samples will be transferred to a freezer (−20°C) within a week of collection. The DBS will be used to determine glycated haemoglobin levels, lipid profile and C reactive protein levels. A drop of blood will also collected to check the random blood sugar using glucometer.
Single lead ECG for atrial fibrillation: the AliveCor Mobile ECG records, displays, stores and transfers single channel rhythms. It records a 30 s tracing and gives the diagnosis as normal or possible atrial fibrillation. The ECG recording will be validated against a diagnosis by cardiologist who is blinded to the diagnosis given by the app.
Data collector training and supervision
SEACO is an ISO certified research platform for its operations and hence training and supervision are carried out in accordance with SEACO's standard operating procedures. All data collectors are required to be fluent in the local language used for interview (Bahasa Malay or Mandarin) and have at least a working knowledge of English. To ensure data quality and consistency across interviewers, the field supervisor will undertake random concurrent supervisory visits to observe practice. The data collectors will also be periodically observed by the project leader and the field manager. Based on the scoring done during these sessions, onsite training or retaining will be carried out as appropriate.
Ethics and dissemination
The study protocol was approved by Monash University Human Research Ethic Committee (CF15/4367—2015001885). Informed consent will be obtained from all eligible participants through signed or video consent. Separate consent will be obtained from the relative before interviewing them on the participants' cognitive status. All participants will receive feedback from their interview which includes information about their height, weight, BP, MMSE score, glucometer blood sugar level and ECG diagnosis; with specific mention of the items that require a physician consultation and evaluation. The cut-offs used for referrals across the different measures are shown in table 2. All data and samples collected in the study will be delinked prior to analysis to ensure that anonymity is maintained.
Cut-offs used for referral of participants in the study across the different measures
The project data and findings will be made available through publications and conference presentations. There is also a searchable data archive under development that would ensure data sharing. Reports will be made available as community briefs on the SEACO website.
Discussion
What is unique about the study?
Malaysian economy is growing and it is predicted that by 2020 Malaysia will transition to becoming a high-income country. Further, Malaysia is a multiethnic country. Therefore, the proposed project will provide a unique resource for studying ageing during economic transition and across ethnic and religiously diverse groups. Risk factors and disease associations may not be consistent with those reported in other world regions where the focus has been on Caucasian populations in a higher income context, and with access to higher quality healthcare and state of the art health technologies for diagnostics and treatment. The study provides the opportunity to evaluate these in the Malaysian context which is more typical of countries within the South East Asian region. The study can also draw on the extensive sociodemographic and health data infrastructure as well as access to populations facilitated through the SEACO community engagement process. This will enhance the response and retention rates towards the establishment of a sustained cohort of elderly people for the long-term assessment of cognitive function in Malaysia.
Why is the study important?
Knowing the burden of cognitive impairment and dementia and risk factors for disease in Malaysia will be necessary for the development of treatment and prevention efforts but it is also important to view these alongside continued increases in life expectancy through population-level indicators such as healthy life expectancy. A similar non-Caucasian resource is the 10/66 Research Study, a multicountry study that explores dementia and ageing in low-income and middle-income countries.25 While there are some data on variability in dementia prevalence and its risk factors (eg, level of educational attainment), questions about ethnic and cultural variation remain unanswered. Our study will therefore complement and extend the work undertaken by the10/66 Dementia Research Group. It will also provide the opportunity to develop a range of cross-culturally validated tools. The study will provide a comprehensive epidemiological research platform for investigating cognition and dementia in Malaysia, and, in the longer term, to maximise the number of years free of cognitive impairment and dementia.
Acknowledgments
The authors acknowledge the SEACO field operations team for their support in designing this study.
References
Footnotes
Contributors DM, BCMS and PA contributed to the drafting of this manuscript. CJ, MP, MS and DDR provided inputs in initial designing of the protocol and in final reviewing of the manuscript.
Funding Funding for SEACO is provided by the Research Offices of Monash University campuses in Australia and Malaysia; the Faculty of Medicine, Nursing and Health Sciences; the Jeffrey Cheah School of Medicine and Health Sciences; and the Faculty of Arts. Ethics approvals for the establishment of SEACO and for this protocol have been obtained from the Monash University Human Research Ethics Committee. This feasibility study is funded through a seed grant from the Monash-Newcastle Partnership Grants.
Competing interests None declared.
Ethics approval Monash University Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data generated from the study are encrypted and backed up by servers at Monash Sunway Campus and at Monash Clayton. Research staff have limited access to anonymised data. There is a searchable data archive under development that would ensure data sharing. It is anticipated that in the medium term, limited de-identified public use data sets will be made available for secondary analysis of the data.