Article Text

Abstract
Introduction Functional somatic syndromes (FSS) are common in adolescents, characterised by severe disability and reduced quality of life. Behavioural treatments such as acceptance and commitment therapy (ACT) has shown promising results in children and adolescents with FSS, but has focused on specific syndromes such as functional pain. The current study will compare the efficacy of group-based ACT with that of enhanced usual care (EUC) in adolescents with a range of FSS operationalised by the unifying construct of multiorgan bodily distress syndrome (BDS).
Methods and analysis A total of 120 adolescents aged 15–19 and diagnosed with multiorgan BDS, of at least 12 months duration, will be assessed and randomised to either: (1) EUC: a manualised consultation with a child and adolescent psychiatrist and individualised treatment plan or (2) manualised ACT-based group therapy plus EUC. The ACT programme consists of 9 modules (ie, 27 hours) and 1 follow-up meeting (3 hours). The primary outcome is physical health, assessed by an Short Form Health Survey (SF-36) aggregate score 12 months after randomisation. Secondary outcomes include self-reported symptom severity, symptom interference, depression and anxiety, illness worry, perceived stress and global improvement; as well as objective physical activity and bodily stress response measured by heart rate variability, hair cortisol and inflammatory biomarkers. Process measures are illness perception, illness-related behaviour and psychological flexibility.
Ethics and dissemination The study is conducted in accordance with Helsinki Declaration II. Approval has been obtained from the Science Ethics Committee of the Central Denmark Region and the Danish Data Protection. The results will be sought to be published according to the CONSORT statement in peer-reviewed journals.
Discussion This is one of the first larger randomised clinical trials evaluating the effect of a group-based intervention for adolescents with a range of severe FSS.
Trial registration number NCT02346071; Pre-results.
- Functional Somatic Syndromes
- Adolescents
- Randomised Controlled Trial
- Study protocol
- Psychotherapy
- Medically Unexplained Symptoms
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Functional Somatic Syndromes
- Adolescents
- Randomised Controlled Trial
- Study protocol
- Psychotherapy
- Medically Unexplained Symptoms
Strengths and limitations of this study
Large-scale study in an area with limited knowledge.
Evaluation of psychosocial and biological predictors and moderators of outcomes.
Thorough assessment of all patients providing them with evidence-based understanding of their illness.
Assessment and treatment are carried out in a specialised setting which might affect generalisation.
Results not automatically applicable to younger adolescents given the developmental perspective, with multiple symptoms being less common in children and younger adolescents.
Background
Functional somatic syndromes (FSS), including chronic fatigue syndrome, juvenile fibromyalgia, functional gastrointestinal disorders and idiopathic pain syndromes, are well-known conditions in adolescents. FSS are diagnostic unities representing clusters of related functional somatic symptoms. Prevalence rates vary considerably due to differences in case definitions, assessment instruments and study populations.1–3 Studies attempting to cover the whole range of different functional somatic symptoms suggest that 5–10% of children and adolescents in the general population are substantially affected and likely to need care.4 ,5 Suffering from FSS during adolescence often has high personal and societal consequences. Adolescents have a higher risk of psychosocial problems such as social isolation, long-term school absence and reduced quality of life,6 and anxiety and depression are common comorbidities.7 ,8 A substantial proportion show continuity of functional symptoms into adulthood9–11 and are less likely to obtain a college education.9 Furthermore, adolescents diagnosed with FSS have higher overall healthcare costs due to increased use of medication and healthcare services.9 ,12 The aetiology of FSS remains unknown. Recent studies suggest a potential correlation between physiological stress and FSS, with physical inactivity as a potential covariate.13–16 It is proposed that a (patho)physiological response to prolonged or severe mental and/or physical stress in genetically susceptible individuals may trigger symptom development.17
High co-occurrence of different types of FSS, especially various pain syndromes, has been shown in children and adolescents.18–20 Children reporting multiple symptoms have an associated higher frequency of distress and impairment (eg, higher kindergarten/school absenteeism and consultations with physicians).21 Moreover, adult patients presenting with multiple symptoms from several organ systems have a poorer prognosis and a higher risk of chronification.22–24 Thus, an attempt to recognise the most severely affected patients with the highest illness burden may encompass sampling patients with the highest symptom load (ie, multiple symptoms from several organ systems). Recently, the empirically based unifying diagnostic category bodily distress syndrome (BDS) was introduced.25 The diagnosis describes specific symptom patterns and includes a multiorgan subtype and four single organ subtypes; in adult samples, it has been shown to capture a range of FSS including fibromyalgia, irritable bowel syndrome, non-cardiac chest pain and chronic fatigue syndrome.26 Multiorgan BDS comprising multiple symptoms from at least three specific symptom groups thus offers a diagnostic unity potentially including the most severely affected patients.
Cognitive–behavioural therapy (CBT) has been shown to reduce symptoms and increase functioning in adults with FSS,27–30 whereas the evidence for treatment in adolescents is sparse. Family-based CBT and internet-delivered CBT have proven effective in young patients with specific FSS.31–36 However, the development of specifically tailored treatments for each FSS or symptom profile seems to be an inefficient strategy due to the costly nature of establishing separate clinics in each medical (sub)specialty, the fragmented care available and difficulty in handling multisymptomatic patients at those clinics.17 ,37 ,38 Recent studies suggest that adult patients with various FSS can feasibly receive the same treatment delivered in a group format, regardless of their main functional symptom.39 ,40 In adolescents, group treatment has been widely used and shown to be feasible in the treatment of psychiatric and non-psychiatric diseases.41 ,42 Group format offers several benefits including peer modelling, diminishment of stigma, increased motivation and higher acceptance of feedback from peers as opposed to professionals.43 Hence, a unified group-based treatment may be advantageous for adolescents with various FSS due to feasibility, accessibility of treatment and potential healthcare savings.
Acceptance and commitment therapy (ACT), which derives from CBT, has shown promising results in children and adolescents with chronic functional pain.44 ,45 Evidence suggests that acceptance of pain is related to enhanced physical and emotional functioning, whereas attempts to control pain may lead to higher pain and disability.46 ,47 By reducing avoidance behaviour and symptom interference, ACT can increase functioning and enhance quality of life, through value-driven acceptance and exposure strategies.48 Symptom avoidance seems to be a general problem leading to disability and lower quality of life in patients with FSS.49 This provides a rationale for a therapeutic approach focused on reduction of avoidance behaviour and acceptance of somatic symptoms.
The objective of the present trial is to examine the efficacy of ACT-based group therapy for adolescents with a range of FSS grouped under the unifying diagnosis of multiorgan BDS.17 To do this, we will examine physical health and a range of other outcomes including level of functioning, symptom interference and emotional distress at baseline, at different time points throughout the trial, and also at 12-month follow-up. An add-on study includes measurement of physiological stress response and physical activity level.
Methods
Design
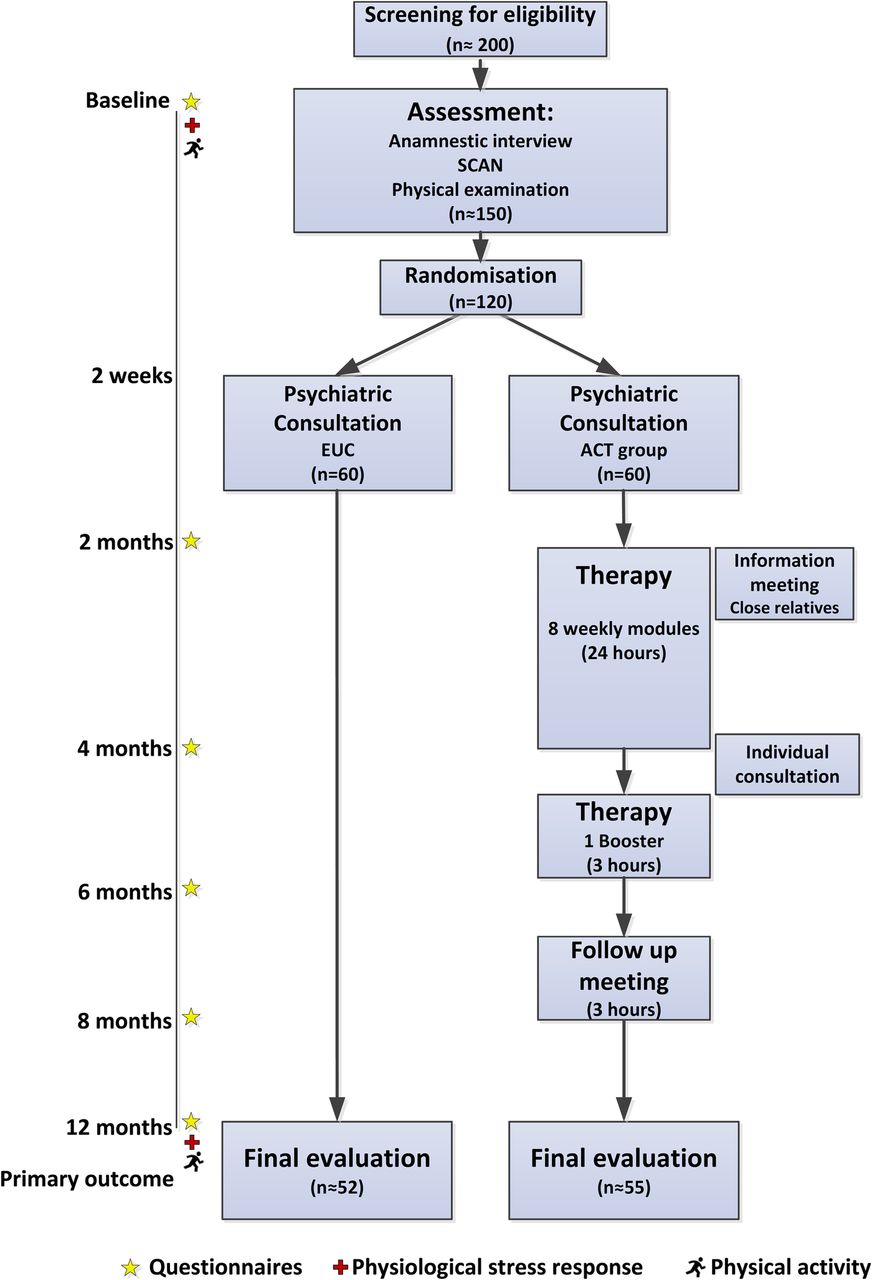
Single-site, non-blinded randomised controlled trial (RCT) with two conditions: (1) group-based ACT and (2) enhanced usual care (EUC). Overall study design is illustrated in figure 1.

Flow chart of participants with estimated numbers at each level. ACT, acceptance and commitment therapy; EUC, enhanced usual care; SCAN, Schedules for Clinical Assessment in Neuropsychiatry.
Setting
Patients will be enlisted from the Research Clinic for Functional Disorders and Psychosomatics, situated in a general medicine setting at Aarhus University Hospital, Denmark. The department is a specialist, tertiary service with extra resources allocated for assessment and treatment of patients with debilitating functional somatic symptoms. Enrolment starts in January 2015 and the data collection is expected to be finalised in June 2019.
Prior to enrolment, an uncontrolled pilot study was performed to test the applicability of the multiorgan BDS diagnosis for this specific age group as well as the feasibility of the new group-based treatment programme. Twenty-one patients were included in the uncontrolled pilot study.
Eligibility
Eligibility criteria are multiorgan BDS, that is, at least three functional somatic symptoms from at least three symptom groups, moderate-to-severe impairment in daily life and symptom duration for a minimum of 12 months (table 1).22 ,26
Inclusion and exclusion criteria
The study criteria are summarised in box 1.
Inclusion and exclusion criteria
Inclusion criteria
1. Bodily distress syndrome, multiorgan type of at least 12 months duration.
2. 15–19-year-olds at referral.
3. Raised since infancy in Denmark or born to Danish parents. Understand, speak and read Danish.
4. Moderate or severe impairment.
Exclusion criteria
1. Not completing informed consent.
2. Acute psychiatric disorder demanding other treatment, or if the patient is suicidal.
3. A lifetime diagnosis of psychosis, mania or depression with psychotic symptoms (International Classification of Diseases, 10th Revision (ICD-10): F20–29, F30–31, F32.2, F33.3), serious cognitive deficits or developmental disorders such as mental retardation and autism (ICD-10: F70, F84).
4. Substance abuse of, for example, narcotics, alcohol or medication.
5. Pregnancy at the time of inclusion.
6. Not suitable for group-based treatment, for example, patients with severe ADHD (ICD-10: F90), severe social phobia (ICD-10: F40.1) or conduct disorder (ICD-10: F91).
Recruitment procedures
A total of 120 adolescents (aged 15–19), referred from general practitioners (GP), practising medical specialists or hospital wards, will be recruited into the trial. All referrals are initially screened for eligibility by a team of physicians from the Research Clinic for Functional Disorders and Psychosomatics.
Assessment
Patients regarded as eligible undergo a standardised clinical psychiatric and somatic assessment, performed by a physician specialised or trained in child and adolescent psychiatry. The assessment consists of a: (1) review of former discharge letters, medical records and other relevant information, (2) standardised clinical interview, (3) Schedules for Clinical Assessment in Neuropsychiatry (SCAN),50 which screens for general psychopathology and contains a detailed section on functional somatic symptoms, (4) screening for child and adolescent psychiatric disorders not covered by the SCAN, that is, attention deficit hyperactivity disorder (ADHD), autism and conduct disorder with specific sections from the child and adolescent psychiatric interview Development and Well-being Assessment (DAWBA),51 (5) a clinicophysical/neurological examination and (6) standard blood tests.
Patients meeting the study criteria (see box 1) are offered participation in the study and are subsequently asked to complete the consent form before enrolment and randomisation. Figure 1 presents the flow of patients during the trial.
Randomisation procedure
Following baseline assessment, patients meeting all study criteria and consenting to participate are randomised to either EUC-based or group-based ACT. The randomisation is conducted by statisticians not involved in treatment. Permuted block randomisation with block sizes ranging from 14 to 16 made by means of a computer algorithm will be used to ensure balanced group sizes and allocation concealment. Patients consenting to participate receive an opaque envelope taken from a sequential order containing information on group allocation, ensuring that initial assessment is not influenced by group allocation.
Since the study compares a psychological treatment with EUC, blinding of participants and therapists is not possible.
Interventions
Enhanced usual care
Patients allocated to EUC will have a psychiatric consultation of 1½ hours duration, ∼2 weeks after clinical assessment, with participation of the patient and his/her parents or close relatives. The consultation is manualised and includes psychoeducation related to the diagnosis of multiorgan BDS, health promoting strategies, advice on medication or other treatment, supplemented with written information on the BDS diagnosis and general recommendations. ACT elements are not incorporated or used in the consultation. The aim of the consultation is to increase the family's understanding of BDS and to optimise management in primary care and social services support by an individualised treatment plan sent to the patient's GP. The consultation is carried out by the child and adolescent psychiatrist doing the initial assessment.
ACT-based group therapy
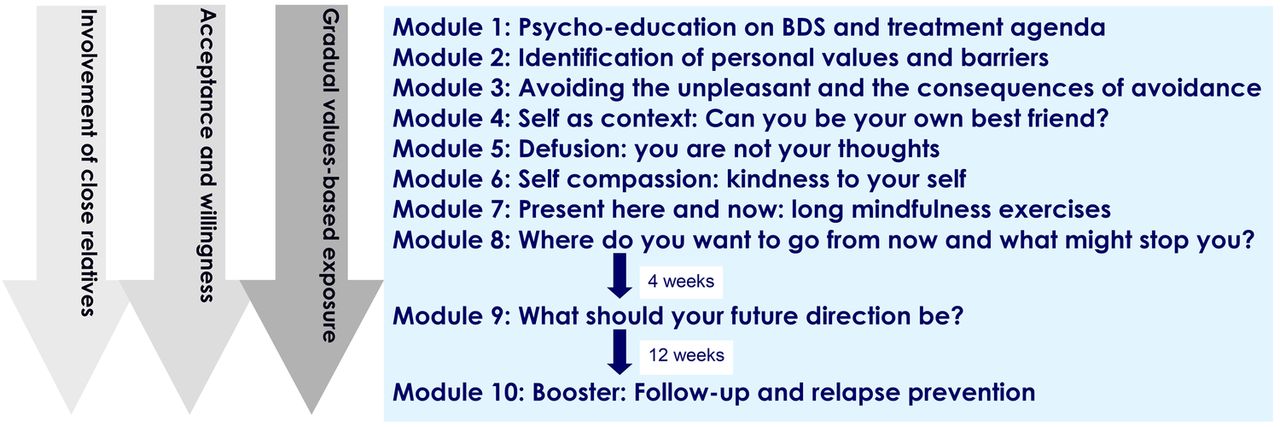
Patients allocated to ACT-based group therapy receive the same psychiatric consultation as described above, before starting the manualised ACT treatment developed specifically for this patient group. The therapy is given in groups of 7–8 patients with nine modules (ie, 27 hours in total) over a period of 3 months and one follow-up meeting (3 hours) 3 months after module 9. Detailed information on the treatment programme is presented in figure 2. The parents and other relevant close relatives (eg, siblings, boyfriends/girlfriends) are invited to participate in an information meeting, to support their resources to help the adolescent improve his/her functional level and ability to cope with the symptoms. One individual consultation with the adolescent and close relatives is offered shortly after module 8. After completed ACT therapy, an individualised treatment plan is sent to the patient's GP.
{kind=link}
{kind=link}
Overview of the group-based acceptance and commitment therapy treatment programme. The overall focus of the treatment is to increase the patients’ physical and emotional self-awareness, and to teach them skills to manage the distress associated with difficult thoughts, emotions and bodily sensations. Practical exercises throughout the treatment include experiential exercises focusing on identification of own values, barriers and avoidance behaviour, and mindfulness exercises focusing on allowance of the experience of here and now as it is and of being present. Gradual exposure is implemented through individually customised homework assignments in accordance with the identified personal values. BDS, bodily distress syndrome.
Patients assigned to ACT therapy have to agree not to have any other psychological treatment for BDS while in therapy.
Therapist training and adherence to treatment manual
Therapists are child and adolescent psychiatrists and psychologists with specialist training in ACT. Clinicians well experienced in ACT and group therapy supervise the treatment. Sessions are videotaped and assessed by an external panel to ensure adherence to the treatment manual.
Compliance and attrition
Treatment compliance is assessed by recording the number of completed ACT modules. When applicable, participants are asked for their reasons for poor compliance or dropout. In the case of dropout from the ACT group therapy, data collection continues as planned with the patients’ consent.
Outcome measures
Outcome measures are obtained at six different time points: at baseline (ie, before assessment and randomisation) and at 2, 4, 6, 8 and 12 months after randomisation. These time points have been designed to follow the time schedule of the ACT group therapy to allow for evaluation of process variables. Figure 1 depicts how these time points relate to assessment and treatment. Primary and secondary outcome measures are assessed by web-based questionnaires (table 2). The questionnaies are distributed simultaneously to all patients within the randomised blocks regardless of treatment group. The primary end point is 12 months after randomisation.
Outcome measures
Owing to a study population of adolescents approaching adulthood (15+ years), questionnaires developed and tested in adults are chosen.
Three questionnaires (Limitation Index (LI),52 Avoidance and Fusion Questionnaire in Youth (AFQ-Y8),53 and Psychological Inflexibility in Pain Scale (PIPS-12)54) have been translated with reference to standard procedures with initial translation, synthesis of translations and back-translation.55
Primary outcome
The primary outcome is improvement in physical health 12 months after randomisation, measured with an aggregate score of the Short Form Health Survey (SF-36) subscales physical functioning (PF), bodily pain (BP) and vitality (VT)56 ,57 with a score range from 15 to 65. This score has previously been used as the primary outcome in a comparable trial in adults39 due to well-known psychometric problems with the existing physical component score (PCS)73 and based on the rationale that these three subscales have shown to be key domains affected in this patient group.74 Danish norm data for adolescents are available.56
Self-reported secondary outcomes
Illness severity is measured by two questionnaires. (1) The Somatisation subscale of the Symptom Checklist Revised-9058 ,61 (12 items, 5-point scale), a widely used symptom checklist of commonly experienced physical symptoms. (2) The BDS checklist59 (25 items, 5-point scale), a symptom checklist added as a new measure for validation in adolescents. It is developed from the symptoms stated in the BDS criteria, hence evaluating symptom severity in four symptom groups.
The impact of symptoms on functioning, that is, symptom interference, is evaluated by self-report and parent report using the LI.44 ,52 LI is a modified version of the Pain Interference Index (PII) (6 items, 7-point scale), a validated questionnaire for children and adolescents measuring the impact of pain in performing everyday activities and impact on, for example, mood and sleep. The modification from PII to LI is limited and represents a change in wording from ‘pain’ to ‘symptoms’. Self-reported degree of absence from school or work is being registered.
Assessing symptoms of anxiety and depression brief versions of the corresponding subscales from Symptom Checklist Revised-90 are used (SCL-8, SCL-6, SCL-4)58 ,60–62 (13 items in total, 5 point scale). Level of illness worry is measured by Whiteley-763 (7 items, 5-point scale), a subscale of the Whiteley Index. Mental health is measured with the Mental Component Summary (MCS) from SF-36.56 ,57
Subjective perception of stress is measured by the Perceived Stress Scale (PSS)64 ,75 (10 items, 5-point scale). The scale is a widely used measure of the degree to which situations in life are perceived as stressful. Danish norm data for adolescents are available.
The overall impression of improvement is measured with the Patient Global Impression of Change (PGIC)65 (1 item, 7-point scale). Answers range from ‘no change (or condition has gotten worse)’ to ‘a great deal better and a considerable improvement that has made all the difference’.
Process measures
The process measures evaluate specific areas hypothesised to play a role in the development and perpetuation of functional somatic symptoms, and are hence addressed directly in the treatment.
Illness perception is measured by the Brief Illness Perceptions Questionnaire (BIPQ)66 (8 items, 10-point scale and additional item regarding cause of symptoms) which has been widely used in a range of illnesses. The perception of five core components (identity, cause, timeline, consequence and cure–control) is evaluated as they together form the perception of illness. In a comparable study with adults, changes in illness perceptions partly mediated the effect of treatment on outcome.76
Illness-related behaviour is measured by the Behavioural Responses to Illness Questionnaire (BRIQ)67 (13 item, 5-point scale). Specific illness-related behaviours have shown to be risk factors for development of FSS in adults.67
Psychological flexibility is an area specifically targeted in ACT. It is measured by the AFQ-Y853 (8 items, 5-point scale) and PIPS-1254 (12 items, 7-point scale).
Potential predictors and moderators
Relevant demographic data and potential important predictors for outcome, for example, predisposition to functional syndromes and number and kind of life events, are obtained as part of the diagnostic assessment.70
Family functioning is assessed by the subscale on general functioning from the Family Assessment Device (FAD)68 ,77 (12 items, 4-point scale). In addition, the patient’′s attachment style is assessed dimensionally by Experience in Close Relationships—Relationship Structure (ECR-RS)69 (9 items, 7-point scale).
Credibility regarding treatment is assessed before the individual standard psychiatric consultation.78 At end of treatment, that is, after module 9, the participants complete a standard questionnaire regarding their experience of the service at the clinic.
Concomitant treatment and serious adverse events during the trial period will be registered by self-report 1 year after randomisation.
Physiological measures
Bodily stress response is assessed with three different measures pretreatment and post-treatment:
Heart rate variability as an indirect measure of the balance between the sympathetic and parasympathetic system. It is measured in various standardised situations (resting state, standing, slow breathing and valsalva) with the handheld device Vagus.16 ,71 ,79
Hair cortisol as a biological marker for long-term bodily stress. It is measured from two strands of hair cut close to the scalp, since the proximal 1 cm segment of hair represents the cortisol level of the past month.80
Biomarkers for inflammatory and oxidative stress (including interleukin 6 (IL-6), tumour necrosis factor-α, high-sensitive C reactive protein, IL-1, neopterin, CD163, heme oxygenase-1 (HO1), monocyte chemoattractant protein-1 (MCP1) as well as newer proteo-based markers).81–84
Physical activity
Level of physical activity is assessed pretreatment and post-treatment by anthropometric measurements with an accelerometer (Actigraph wGT3X-BT).72 The accelerometer is worn on the right hip 24 hours-a-day for seven consecutive days.
A specific protocol for evaluation of physiological measures and physical activity will be made specifying hypotheses and analytical strategies. A large ongoing epidemiological study in Denmark (DanFunD) will be available for later comparison of results.85
Sample size estimation
Power estimation is based on the primary hypothesis regarding changes in self-reported physical health measured with the SF-36 aggregate score. Given the efficacy in a previous RCT study of ACT in adolescents with chronic functional pain44 as well as data on a subgroup of patients under 30 years from another RCT study of CBT with BDS,39 an improvement of self-reported physical health is estimated to be maximum three points (from 39 to 42) in the control group and at least five points (from 39 to 44) in the ACT group from baseline to 12 months after randomisation. The baseline value assumes an SD of 8 referring to the defined groups of patients. Using a random-effects model in a simulation setting shows that in order to statistically detect such a difference in improvement (test of no interaction), given a two-sided α of 0.05 and with 95% power, we need to allocate 60 patients to each group.
Statistical analysis
The efficacy of the ACT treatment will be evaluated on an intention-to-treat basis by means of random-effects model regression analysis adjusted for prognostic important baseline characteristics. The main efficacy analysis will pertain to the data obtained at 12 months follow-up. Baseline characteristics will be tabulated by treatment modality in order to evaluate success of randomisation. To judge possible bias due to missing data, a random-effect model on multiple imputed data will be performed.
An explorative mediation analysis will be performed to investigate to what extent the intervention can affect the primary outcome through each of the process measures. The analytical strategy previously used in a large-scale trial will be used.86
Dissemination
Results will be reported according to the CONSORT statement for non-pharmacological interventions,87 and will be submitted for publication in peer-reviewed English language journals. Positive, inconclusive and negative findings will be published. Trial findings will also be disseminated through conference abstracts.
Data monitoring and management
This trial is considered a minimal risk study and hence a data and monitoring committee has not been established. Questionnaires are administered electronically and saved in an online database. The database is secured with a password-protected access system, and access to files is limited to research staff that requires direct access. Baseline information obtained during assessment is registered in a Case Report Form (CRF). All CRFs are stored in locked file cabinets in areas with limited access.
Discussion
Adolescents with FSS are at risk of continuity of physical problems into adulthood implying reduced quality of life due to potential functional impairment, social withdrawal, lack of education and incapacity to work. To the best of our knowledge, this study will be one of the first larger randomised clinical trials, evaluating the efficacy of a group-based treatment for adolescents with a range of FSS grouped under the unifying diagnosis of multiorgan BDS compared with EUC.
Our study design has some limitations. First is the lack of comparison with an evidence-based control treatment. However, since the aim of this study is to compare ACT group therapy to the best treatment available (ie, EUC), we use a pragmatic design that offers systematic clinical assessment and an individual treatment plan also to patients in the usual care arm. Also, a unified treatment for adolescents with a range of FSS has not been tested before. Second, blinding is not possible to the clinician providing the standard psychiatric consultation. However, this is a general problem in trials of behavioural interventions. Third, the study design does not allow us to determine which treatment components are most important in achieving change. Accordingly, our aim is to assess whether the whole complex intervention as delivered is more effective than EUC in improving physical health. Fourth, the assessment and treatment are carried out in a specialised setting, which might not guarantee that the treatment, if proven successful, will work in everyday clinical practice across different populations, clinical contexts, etc. Finally, the results from the study cannot automatically be applied to younger adolescents given the developmental perspective, with multiple symptoms being less common in children and younger adolescents.
Important strengths of the study are the evaluation of potential psychosocial and biological predictors and moderators of outcomes. Furthermore, all patients are given a thorough assessment providing them with a positive and evidence-based understanding of their illness,88 ,89 and the treatment model is developed based on treatments with proven effect for both paediatric and adult patients with FSS and related disorders.39 ,40 ,44
Bias is minimised by the use of a manualised treatment, different therapists, valid outcome measures, multiple assessment points and by predefining and publishing all outcome measures before study start.
Anticipated difficulties conducting the study include recruitment problems due to stringent inclusion and exclusion criteria as well as lack of knowledge of available service for adolescents and social prejudices in terms of receiving psychiatric diagnosis and psychological treatment for functional symptoms.8
In conclusion, this study will provide important information about efficacy, processes of change and moderators. If the treatment is successful, it will improve the quality of life of adolescents with FSS and may, over the life course, lead to substantial savings in both healthcare costs and societal costs.
References
Footnotes
Contributors KHK took part in designing of the study, drafted the initial manuscript and prepared the final manuscript as submitted. AS took part in developing the research idea and in designing of the study, contributed with data for statistical power analysis and critically revised the manuscript. RKW took part in designing of the study, contributed with data for statistical power analysis and critically revised the manuscript. PF took part in developing of the research idea and critically revised the manuscript. EØ took part in the statistical design of the study, made the power analysis and description of the statistical method and critically revised the manuscript. CUR came up with the original research idea, took part in designing of the study, drafted the initial treatment protocol and critically revised the manuscript. All the authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding This study is supported by TrygFonden (grant number 100408) and the Danish Medical Associations Research Fund (grant number 2013-5480/912523-63).
Disclaimer None of the funding sources have authority over any of the study activities.
Competing interests None declared.
Ethics approval The project will be conducted in accordance with Helsinki Declaration II. Approval has been obtained from the Science Ethics Committee of the Central Denmark Region (journal number 1-10-72-181-14) and the Danish Data Protection (reference number 2007-58-0010; application number 1-16-02-290-14).
Provenance and peer review Not commissioned; externally peer reviewed.