Article Text

Abstract
Introduction Lower respiratory infections (LRIs) and pneumonia are among the leading causes of death worldwide, especially in children aged under 5 years, and these patterns are reflected in the South African population. Local epidemiological data for LRIs and pneumonia are required to inform the Second National Burden of Disease Study underway in South Africa. The aim of this systematic review is to identify published studies reporting the prevalence, incidence, case fatality, duration or severity of LRI and pneumonia in adults and children in South Africa.
Methods and analysis Electronic database searches will be conducted to obtain studies reporting on the prevalence, incidence, case fatality, duration and severity of LRI and pneumonia in South Africa between January 1997 and December 2015. Studies that are assessed to have moderate or low risk of bias will be included in a meta-analysis, if appropriate. Where meta-analysis is not possible, the articles will be described narratively. Subgroup analysis (eg, age groups) will also be conducted where enough information is available.
Ethics and dissemination This systematic review will only include published data with no linked patient-level information; thus, no ethics approval is required. The findings will be used to calculate the burden of disease attributed to LRI and pneumonia in South Africa and will highlight the type of epidemiological data available in the country. The article will be disseminated in a peer-reviewed publication.
PROSPERO registration number CRD42016036520.
- lower respiratory infection
- pneumonia
- south africa
- burden of disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
To the best of our knowledge, this will be the first systematic review on lower respiratory infection (LRI) and pneumonia in South Africa.
This review should provide epidemiological parameters necessary to model disease burden due to LRI and pneumonia in South Africa.
The protocol conforms to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA-P 2015) guidelines.
Depending on whether very wide or narrow case definitions are used for LRI and pneumonia, the burden of disease may be overestimated or underestimated and varying case definitions may limit comparison across studies.
All observational studies will have the robustness of their methods examined by using a risk-of-bias-tool and studies will be excluded if they have a high risk of bias as they may limit this study.
Introduction
Pneumonia is a common lower respiratory infection (LRI).1 Even though clear definitions do exist, the distinction between LRIs and pneumonia is often ambiguous as the terms are used interchangeably by researchers. In 2013, the Institute for Health Metrics and Evaluation (IHME) Global Burden of Disease (GBD) study found that LRIs accounted for 2.7 million deaths worldwide.2 They also reported that pneumonia was the leading cause of death in children aged under 5 years and contributed to 14% of total child deaths globally in 2013.3 Although pneumonia can affect people of all ages, children aged under 5 years, adults over 65 years and immunocompromised persons tend to be more at risk.4 The majority of pneumonia mortality (81%) occurs within the first 2 years of life.5 Globally, it has been estimated that ∼12% of pneumonia episodes progress to severe episodes in children.5
Pneumonia is an acute form of respiratory tract infections whereby the lung alveoli become filled with fluid, causing painful breathing and limiting oxygen intake.4 Various pathogens cause pneumonia, the most common being bacterial (eg, Streptococcus pneumoniae, Haemophilus influenzae type b (Hib)) or viral (eg, respiratory syncytial virus (RSV)).4 The pathogens that cause pneumonia vary by a number of factors; these include: age (eg, RSV commonly affects children aged under 2 years,4 S. pneumoniae appears to be the most common bacterial cause in children in the developing world4 ,6 and community-acquired pneumonia (CAP) in the elderly);7 and HIV status (Pneumocystis jirovecii (previously P. carinii) pneumonia is a common opportunistic infection and substantial cause of mortality in HIV-positive individuals).8 Nevertheless, identifying specific causal pathogens (especially bacteria) in children can be difficult, as the identification of a pathogen does not establish causality. Furthermore, mixed viral and bacterial infections are known to occur simultaneously.9
Definite risk factors for children in developing countries include malnutrition, low birth weight, non-exclusive breast feeding (first 4 months of age), lack of measles immunisation (first 12 months of age), indoor air pollution and crowding.10 Possible risk factors include mother's education, day care attendance, vitamin A deficiency, birth order, and environmental factors such as humidity, high altitude and outdoor air pollution.1 ,10 Other likely risk factors include: parental smoking, zinc deficiency, concomitant diseases (eg, diarrhoea, asthma), etc.1 ,10 The elderly are more prone to developing severe disease as their immunity and lung function tend to be compromised due to the ageing process.7 In addition, swallowing disorders, malnutrition, comorbidities (eg, diabetes, renal disease) and inactivity (bedridden status) also predispose the elderly to acquiring CAP.7 Immunosuppression can increase the risk of developing pneumonia at any age.4
LRIs and pneumonia in South Africa
Pneumonia is a major reason for health facility usage in low and middle income countries.5 The sub-Saharan African and South Asian regions have been disproportionally affected by deaths from pneumonia in children aged under 5 years.3 The first South African National Burden of Disease (SANBD-1) study ranked LRIs as the sixth leading cause of premature mortality in South Africa contributing to 3.8% of the years of life lost (YLLs) in the country in 2000.11
The second SANBD (SANBD-2) study,12 currently underway, intends to estimate the disease burden for the country using summary measures of population health for the years 1997–2012. The health loss from premature mortality (YLLs) needs to be combined with the loss of healthy life due to disability or morbidity from non-fatal outcomes (years lived with disability, YLD) in order to calculate the disability-adjusted life years (DALYs).13 The SANBD-2 has estimated the YLLs using vital registration and other data sources.14 In order to calculate the YLDs due to LRI and pneumonia, nationally representative epidemiological data are needed. If these are not available, findings from smaller studies can be included to estimate YLDs using a pooled meta-analysis. The YLD component can be estimated through disease modelling of at least three epidemiological parameters (prevalence, incidence, case fatality, duration or severity) pertaining to LRIs and pneumonia in South Africa. To the best of our knowledge, no systematic reviews have been conducted to determine the prevalence, incidence, case fatality, duration or severity of LRIs and pneumonia in South Africa.
AIM
In order to present evidence on epidemiological parameters relating to LRI and pneumonia in South Africa, a systematic literature review will be conducted to identify published studies that report the prevalence, incidence, case fatality, duration or severity of LRI and pneumonia. Furthermore, this review will also report on the variation of definitions used to describe LRI and pneumonia. The findings from this review will be used to estimate the morbidity burden due to LRI and pneumonia (to generate YLDs and DALYs) in South Africa.
Methods
Eligibility criteria
Studies will be selected according to the criteria outlined below.
Types of participants
Studies assessing the epidemiology (prevalence, incidence, case fatality, duration or severity) of LRI and pneumonia, in children and adults from anywhere in South Africa, will be included.
Case definition
The definitions for LRI and pneumonia can be problematic.14 ,15 Pneumonia in children is a diagnosis made on tissue pathology and thus there is no clinical definition that is completely accurate.9 The WHO's case definition for childhood pneumonia is widely used in resource-poor settings,16 although it lacks specificity.14 Definitions also vary by age group. Included studies should clearly state a case definition for LRI and pneumonia, whether it be a clinical description, radiological, laboratory-based or International Classification of Diseases (ICD) codes. Owing to variations in LRI and pneumonia definitions, we will extract the definitions as reported in individual studies (whether clinical description, radiological, laboratory-based or ICD codes).
Although LRIs and pneumonia are among the most common diseases in the world, many other conditions (eg, malaria, bacterial sepsis, severe anaemia) produce clinical symptoms that significantly overlap with those of LRIs and pneumonia and thus differentiating between conditions can be a challenge.14 This will be evaluated by carefully assessing the appropriateness of case definition in consultation with respiratory disease experts, and methodologies used by studies (eg, whether the investigator attempted to exclude bronchiolitis, sepsis, pertussis, measles, asthma, malaria or neonatal sepsis in children9).
Inclusion criteria
Studies will be included if they are conducted in South Africa, report one of the primary outcomes (listed below) and report a clear case definition for LRI and pneumonia.
Exclusion criteria
Studies will be excluded from this review if they are not conducted in South Africa, do not report any of the primary outcomes (listed below) and have no clear case definition for LRI and pneumonia.
Outcomes
Primary outcome
The primary outcomes of interest are prevalence, incidence, case fatality, duration or severity of LRI and pneumonia.
Owing to the acute nature of LRI and pneumonia, especially in children, incidence rather than prevalence is used to estimate the burden of the disease. In chronic cases, incidence and prevalence are appropriate. Therefore, both terms (ie, ‘incidence’ and ‘prevalence’) will be included in the search strategy to ensure that no relevant studies are unintentionally excluded.
For this review, the definitions for prevalence, incidence, case fatality and duration will be adapted from Bonita et al,17 Giesecke18 and Joubert et al.19 Prevalence is defined as the number of people with disease (LRI and pneumonia) at a specified time divided by the population at risk at the specified time. The point prevalence rate refers to data collected at one point in time and the period prevalence rate refers to the total number of cases at any time during a specified period, which is then divided by the population at risk midway through the period.17 The incidence of LRI and pneumonia refers to the number of new cases occurring in a population.17 Cumulative incidence is often measured over a longer period18 and refers to the number of people who get a disease during a specified period divided by the number of people free of disease at the start of the period,17 while the incidence rate (or incidence density) is the number of new cases in a specified time period divided by the total disease-free person-time of observation in the at-risk population. Case fatality refers to the percentage of cases with disease (LRI and pneumonia) who died of the disease out of those who contracted it.18 In terms of LRI and pneumonia, the definition for duration refers to the average duration spent in the diseased state, as described by the DisMod II help guide.20
Severity refers to the proportion of severe cases of LRI and pneumonia from a defined population with LRI and pneumonia. Studies may define severity differently. Studies on children may use the WHO Integrated Management of Childhood Illness (IMCI) classification21 which includes only two categories of pneumonia:
Pneumonia: pneumonia with fast breathing and/or chest in-drawing that can be treated at home with oral amoxicillin.
Severe pneumonia: pneumonia with any general danger signs which requires referral and injectable treatment.
Studies on adults may use the CURB-65 score to classify the severity of CAP.22 Each component has a score of 1 and if a patient scores either 0 or 1, they are classified as mild and can be treated at home (depending on social circumstances). If the patient scores 2, they are classified as moderately ill and hospital treatment may be necessary, while a score of ≥3 implies severe pneumonia.22 ,23
Secondary outcome
A narrative comparison of case definitions for all included studies that describe how LRI and pneumonia are defined.
Types of studies
We will include published population-based surveys, cross-sectional studies, prospective or retrospective cohort studies, case–control studies and studies on surveillance systems. Interventions studies, studies on diagnostic accuracy and grey literature will be excluded. Studies that include South Africa will be reviewed and only the South African data will be added to the review. Studies based on miners due to their specific exposure will be excluded.24 ,25 All English studies published from January 1997 to December 2015 will be included.
Search strategy
A comprehensive search strategy will be formulated. Disease content experts will be contacted to ensure that the search terms are relevant and optimal for our purposes. The search strategy will be modified, where necessary, according to the database or search engine used. Disease content experts will also be contacted to identify studies that they deem relevant. An example search strategy is shown in figure 1.
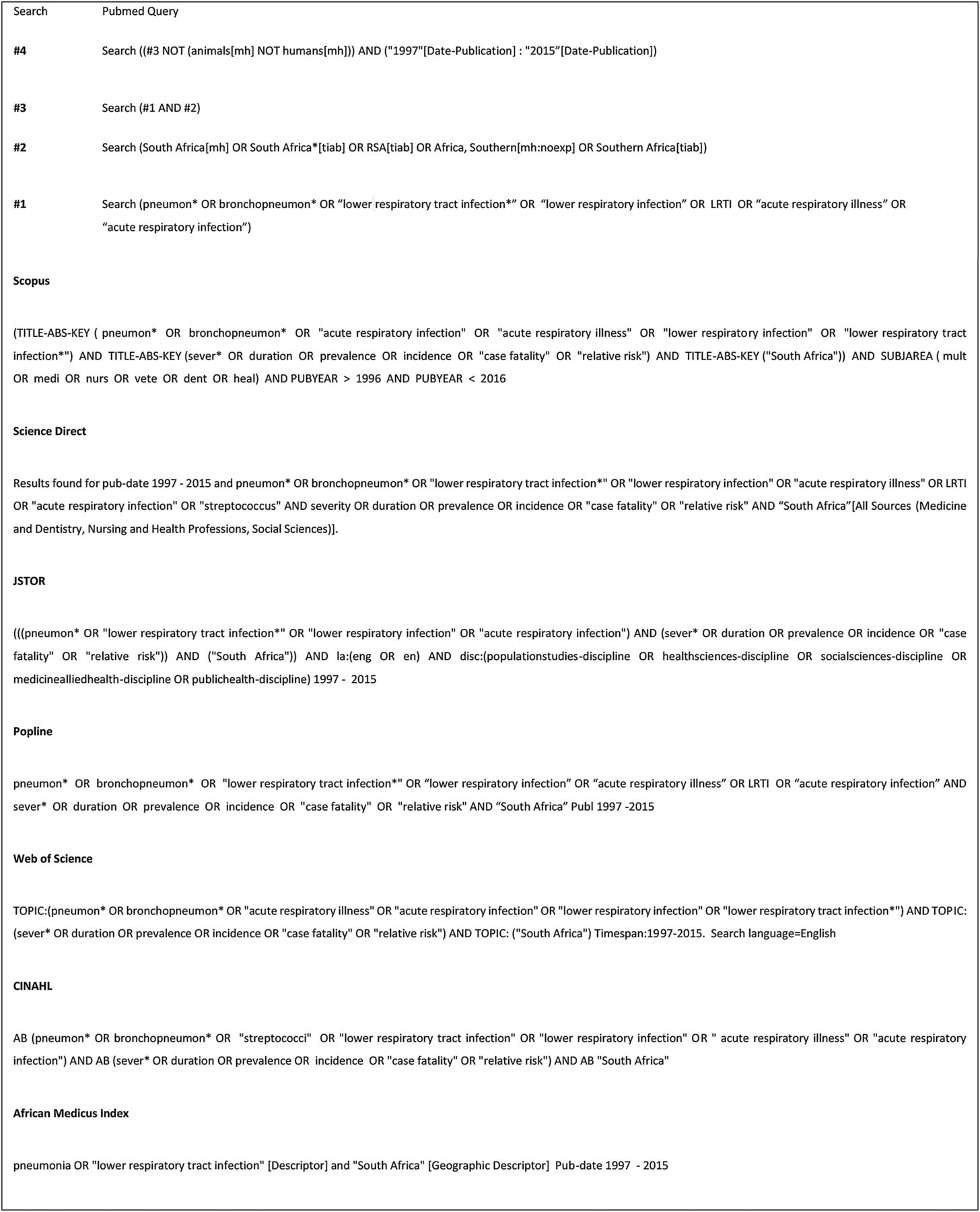
{kind=link}
Search strategy.
Electronic databases
The following electronic databases and search engines will be used: PubMed, Scopus, Science Direct, JSTOR, POPLINE, Web of Science, CINAHL and African Index Medicus.
Selection of eligible studies
Two researchers will independently screen the titles and abstracts from the search output against the inclusion criteria to identify potentially eligible studies. These studies will have their full-texts retrieved and independently reviewed for inclusion. Additional information will be requested from study authors where required. Any disagreements will be resolved through discussion between the two researchers. Reasons for exclusion will be recorded. The researchers will not be blinded to journal titles, study authors or institutions.
Data collection process
Relevant information will be independently extracted from included studies and recorded using an electronic system (the Burden of Disease Review Manager). Once completed, the reviewers will compare the data extracted and any disagreements will be resolved through consensus. If no agreement can be reached, a third researcher will be consulted. If needed, authors of studies will be contacted for additional information. The following data will be extracted:
Study details: year of study publication, study design, study period and study purpose.
Study population: country/province/district of study, study setting (community or health facility based).
Case definition: as reported in study.
Prevalence, incidence, case fatality, duration, severity of LRI and pneumonia; and definitions used to describe these parameters.
Characteristics of cases: age, sex, vaccination status, comorbid diseases (eg, HIV status).
Risk-of-Bias quality assessment
Two researchers will independently assess the risk of bias of each study using a modified checklist.26 This checklist was created by adapting the risk-of-bias tool for population-based prevalence studies described by Hoy et al,27 and the Newcastle-Ottawa Scale for assessing the quality of non-randomised studies.28 This new checklist (tool) was pretested and modified to suit our context. The tool assesses both internal and external validity, and each item is assigned a maximum score of four or minimum score of zero, depending on the question. The overall quality score ranges from 1 to 20 (high risk=1 to 6; moderate risk=7 to 13; low risk=14 to 20).
The researchers will discuss and resolve any discrepancies between their independent assessments and assign the study a final score. Studies deemed to be of poor methodological quality will be excluded and the reasons for exclusions will be noted.
Data synthesis
Only studies assigned to moderate or low risk in the risk-of-bias quality assessment will be included in the analysis. Case definitions along with other data will be presented in a narrative synthesis and tabulated.
In the event that the generated data are amenable to meta-analysis, we will perform separate meta-analyses for each of the epidemiological parameters using Stata 13 (College Station, Texas). We will pool estimates across studies and obtain an overall summary estimate and 95% CI. Clinical heterogeneity will be judged by the differences in types of participants and case definitions used for LRI and pneumonia. Statistical heterogeneity will be assessed using χ2 test. The statistically significant heterogeneity will be considered existent when χ2 p≤0.10.29 ,30 The I2 statistic will be used to determine the degree of heterogeneity. If the study results are found to be statistically homogeneous (ie, when χ2 p>0.10), we will pool them using the fixed-effect meta-analysis. Otherwise, we will use random-effects meta-analysis. Publication bias will be assessed by visual inspections of funnel plots, provided that there are at least 10 studies.31 The results will be presented in a systematic narrative synthesis when it is not possible to pool the data. This will be used to summarise each study's findings and similarities and differences between included studies.
Where possible, a trend analysis will be conducted to explore the epidemiological parameters of LRI and pneumonia in South Africa over time, taking the introduction of Prevention of Mother to Child Transmission of HIV (PMTCT), seasonality and vaccines into account. When analysing data, care will be taken to identify trends in the light of historical changes in the vaccination programme in South Africa, namely changes over time in Hib, pneumococcal conjugate vaccine-7 (PCV-7), rotavirus vaccinations, pertussis vaccine, Hib booster and the PCV-13.
Subgroup analysis
Where sufficient data exist, subgroup analysis will be conducted based on case definition criteria (eg, clinical description, radiological, laboratory based or ICD codes), setting (eg, community or health facility, geographical location), age groups (eg, children and adults aged >65 years), cases with comorbidities (eg, HIV) and time periods (eg, periods that certain vaccinations were introduced vs years prior to that vaccination; study periods for seasonality).
Confidence in cumulative evidence
The main findings will be summarised and include the strength of evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.32 GRADE classifies evidence into four levels (high, moderate, low and very low) based on study limitations, inconsistency of results, indirectness of evidence, imprecision and reporting bias. GRADE also allows for either ‘strong’ or ‘weak’ recommendation based on the strength of the evidence and other related factors.
Amendments to the protocol
Should protocol amendments occur, these will be dated together with a description and reason for the change.
Ethics and dissemination
This study will use the results of other published studies which cannot be linked to individuals and thus does not require ethics approval. The findings will be used to calculate the burden of disease attributed to LRI and pneumonia in South Africa and will highlight the type of epidemiological data available in the country. The estimated burden of disease due to LRI and pneumonia will be important in guiding policymakers. The findings of the systematic review will be written up in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 guidelines.
Acknowledgments
The authors acknowledge Ms Michelle Galloway for editing the final draft of the protocol.
References
Footnotes
Contributors RAR, VP-vW, OFA, AD, PG, JDJ, MDN, EN and DB conceptualised the study. RAR wrote the first draft of the protocol. VP-vW, OFA and DB reviewed the first draft and gave intellectual input. All the authors provided input for subsequent drafts. The study design was developed by RAR, VP-vW, OFA and MDN. All the authors gave approval for publication.
Funding This research and the publication thereof were partially funded by the South African Medical Research Council's Flagship Awards Project SAMRC-RFA-IFSP-01-2013/SA CRA 2 and Programme for Economic Evaluation of Child & Maternal Health Interventions (PEECHi).
Disclaimer The funders had no role in study design or writing of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.