Article Text

Abstract
Introduction Self-harm is a strong predictor for suicide. Risks for repeat behaviour are heightened in the aftermath of an index episode. There is no consensus on the most effective type of intervention to reduce repetition. Treatment options for patients who do not require secondary mental health services include no support, discharge to general practitioner or referral to primary care mental health support services. The aim of this study is to assess whether it is feasible to deliver a brief intervention after an episode and whether this can reduce depressive symptoms and increase the sense of well-being for patients who self-harm.
Methods This is a non-blinded parallel group randomised clinical trial. 120 patients presenting with self-harm and/or suicidal ideation to mental health services over a 12-month period who are not referred to secondary services will be randomised to either intervention plus treatment as usual (TAU), or control (TAU only). Patients are assessed at baseline, 4 and 12 weeks with standardised measures to collect data on depression, well-being and service use. Primary outcome is depression scores and secondary outcomes are well-being scores and use of services. The findings will indicate whether a rapid response brief intervention is feasible and can reduce depression and increase well-being among patients who self-harm and do not require secondary services.
Ethics and dissemination Ethical approval was granted by the UK National Health Service (NHS) Ethics Committee process (REC 6: 14/WA/0074). The findings of the trial will be disseminated through presentations to the participating Health Board and partners, peer-reviewed journals and national and international conferences.
Trial registration number ISRCTN76914248; Pre-results.
- randomised controlled trial
- self harm
- intervention
- depression
- social support
- suicide prevention
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The development of an enhanced contact intervention for people who have little or no support following self harm.
A focus on social issues that are present in the person's life.
A cost-effective intervention that can work alongside existing services, supporting patients during a vulnerable time and keeping them engaged whilst they are awaiting assessment from other services.
As this is an unblinded trial, there is a risk of bias in the data.
We are not collecting any social outcome measures.
Background
Self-harm is the strongest risk factor for future suicide1 resulting in over 200 000 hospital presentations annually in England and Wales2 ,3 and is associated with high personal, social and medical costs.4 Repetition is common, with 15–25% re-presenting to the same hospital within a year of the index episode.5 The highest risk of repeat self-harm is within 3–6 months after the index episode6 with the risk for suicide in the year following self-harm almost 50 times higher than in the general population.7
Depressive symptoms are prevalent among those with self-harm and suicidal ideation8 and is strongly linked with progression to attempt suicide.9 Owing to the strong link between a mental health condition and self-harm,10 the majority of interventions are based on psychological and medical approaches.11 However, it is not just mental health disorders that trigger self-harm, it is known that most patients who present with self-harm have numerous social and interpersonal problems which act as catalysts for self-harm behaviour.12 ,13 Hence National Institute for Health and Care Excellence (NICE) guidelines explicitly state that patients who present with self-harm should receive a psychosocial assessment14 to address their psychological and social needs. However, this is often not routinely offered15 and many patients who present to the emergency department with self-harm are discharged without any assessment16 despite evidence that psychosocial assessment is associated with a lower risk of repetition.17 Presentations to hospital tend to prioritise risk factors to determine medical needs, admission, referral or discharge, above psychosocial needs. A lack of psychosocial assessment leaves much of the impact of social situations underexamined. While addressing immediate psychological and medical needs are vital, a lack of exploration of the social milieu of the patient may miss important factors that might have been precipitous in the self-harm behaviour and therefore may be a recurring antecedent for self-harm. In the absence of routine psychosocial assessments,15 patients who present with self-harm and who do not have a known history of mental health problems, often receive little or no support from healthcare services, with signposting to community services or discharge to general practitioner (GP) being the main course of management. Supporting such individuals who do not require secondary mental health services to deal with stressors and enabling them to better manage stressors may help alleviate their impact and thus reduce rates of self-harm as a response to ongoing or repeated stress.
There have been calls to explore social factors when assessing self-harm as they are increasingly being identified as instrumental in these behaviours.18 Studies report that as many as 70% of self-harm episodes are triggered by interpersonal problems.19 The importance of recognising and responding to social factors in self-harm and suicide prevention has been described in the literature.20 There is global evidence of significant increases in suicide rates following economic recession21 with unemployment being strongly linked with suicide for men and women.20 Research has also linked an elevated risk of suicide with isolation and a lack of social integration.22
There is little effective primary care prevention for patients who self-harm either as a first episode or repeatedly.23 Numerous interventions have been trialled in attempting to reduce self-harm and suicidal behaviour.24 ,25 These vary significantly in content, and no single type of intervention has been found to deliver consistent results. Positive outcomes in reducing self-harm have been reported for non-pharmacological interventions26 such as provision of an emergency access card.27 Findings from contact interventions vary, with some reporting long-term positive impacts.28–31 Contact interventions, including telephone, postcard and letter interventions offer a cost-effective way of supporting individuals by reducing a sense of isolation and increasing a sense of social connectedness; it has been argued that perceived connectedness can reduce suicidal ideation.31 An elevated sense of support may encourage help seeking at times of crisis.31 Reviews of contact-based interventions (eg, postcards, crisis cards, telephone calls) after admission to a hospital have found inconsistent results across studies and concluded that more research is needed.30 ,31
This study draws on findings that suggest increasing social support through contact-based interventions can support those who self-harm and reduce suicide rates.29 An Australian study32 reported an intervention focusing on connecting individuals to relevant and available support led to a reduction in depression scores and an increase in well-being. This study adapts that intervention to offer a brief non-psychological and non-medical intervention delivered by trained practitioners. Initially, we intended to replicate the study, but a difference in healthcare systems and access across Australia and the UK, means that a full replication is not possible (see Willis et al33 for a description of the Australian healthcare system). In remaining as close to that study we are using the same outcome measures they applied— Beck Depression Inventory—II (BDI-II)34 to measure depression and Manchester Short Assessment of Quality Of Life (MANSA)35 to measure quality of life. Additionally we are collecting the Client Services Receipt Inventory (CSRI)36 to measure service use and the study is registered with the Secure Anonymised Information Linkage (SAIL) database for a 1-year follow-up of service use.37 ,38
The aim of this study is to assess whether an enhanced contact intervention is beneficial for patients who present with self-harm and/or suicidal ideation but are not referred to secondary services. We define it as an enhanced contact intervention as it goes further than what is usually termed contact intervention in the literature. Contact interventions tend to be more remote and use postcards or phonecalls.28–30 Our intervention involves regular face-to-face contact. It focuses on social factors and actively links individuals to services that can help with social problems including financial issues, housing, relationship difficulties, employment, literacy, etc. The intervention is flexible to meet the needs of the patient; it does not require patients to engage with services if they are not ready; for such patients, regular contact with the intervention practitioner provides support and a source of social contact at a vulnerable time. The intervention goes beyond signposting with assertively linking the individual to relevant support agencies (eg, community organisations) that already exist. By doing so, the individual becomes embedded in to a support network from which they can draw on at future times of stress.
Methods
Design and setting
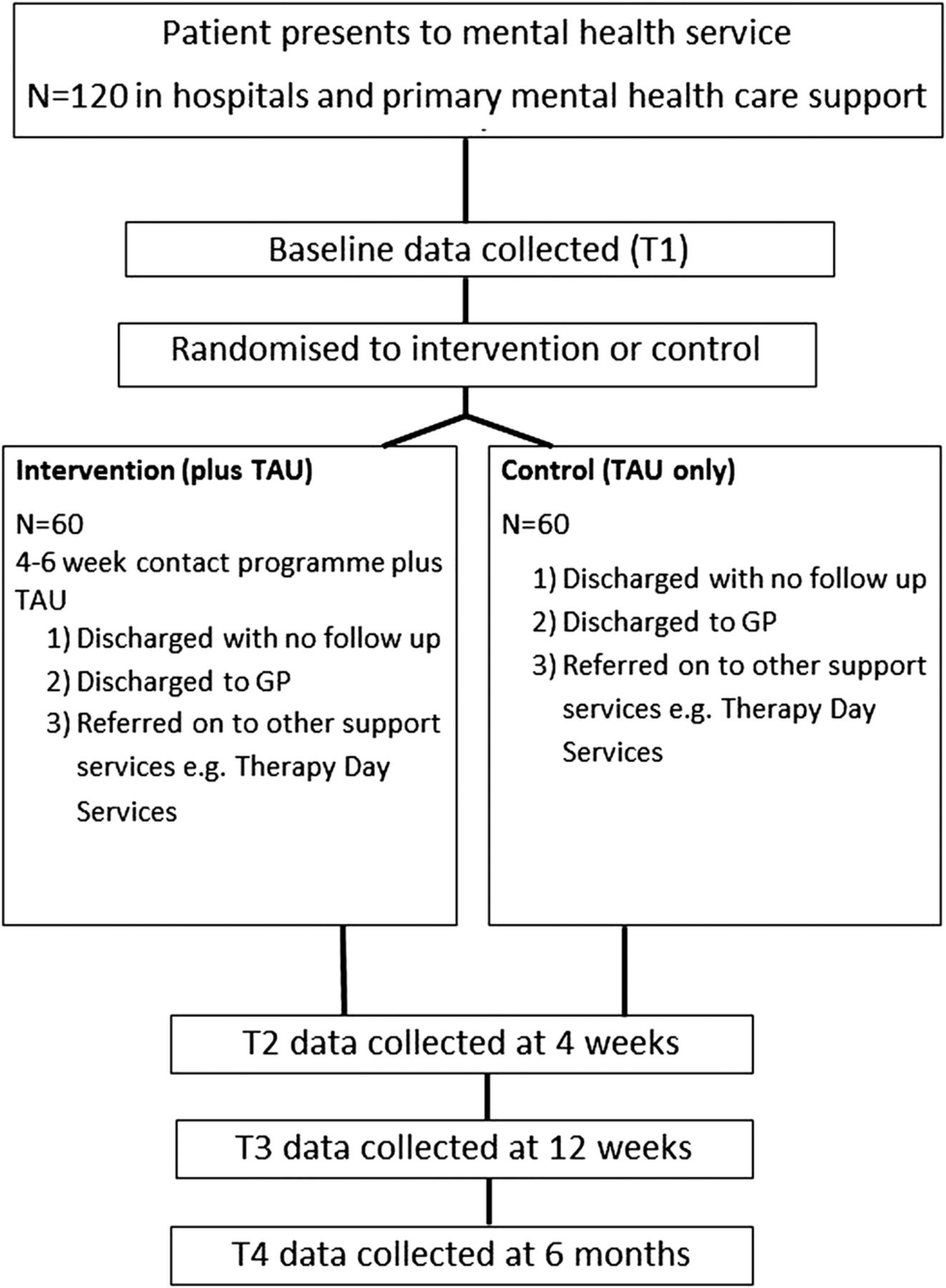
This is a randomised controlled trial (RCT) conducted by Swansea University in partnership with Hywel Dda University Health Board (HDUHB) running between January 2015 and March 2016 in Carmarthenshire, West Wales. The trial delivers an enhanced contact intervention to patients over 18 who present to mental health services (defined as hospital emergency department and local primary mental health support services) and who would ordinarily be referred back to primary care and/or community services. Patients who require admission or crisis intervention are excluded from Social support and Wellbeing Intervention following Self Harm (SWISH) and referred to appropriate services. Patients who meet the inclusion criteria are randomised to the intervention or control group. The intervention is a 4–6-week programme of face-to-face and phone call contact tailored to meet the needs of the individual in addition to treatment as usual (TAU) which ranges from discharge with no further support, signposting via leaflets to community organisations, or referral to primary care for ongoing care. The control arm is just TAU. The full duration of patient participation is 12 weeks with assessments collecting standardised measures for depression, well-being and service use conducted for all patients at baseline, 4 and 12 weeks. Where possible a 6-month follow-up using the same measures will be sought (see figure 1).

{kind=link}
Study chart. GP, general practitioner; TAU, treatment as usual.
Study population
Patients who present to mental health services (either directly to hospital or indirectly through referral from GP to local primary mental health support services) with self-harm and/or suicidal ideation are assessed by the mental health practitioners at these sites and those thought suitable for SWISH are referred to SWISH in addition to their TAU. A SWISH worker conducts a further eligibility test based on inclusion and exclusion criteria before inviting a patient who meets the requirements to participate. Patients are given a study information leaflet and time to consider whether they would like to take part. Written consent is obtained by the research assistant prior to baseline data collection. Once baseline data have been collected patients are randomly assigned to either intervention or control.
Inclusion criteria
Any person aged 18 or over who presents to mental health services with self-harm and/or suicidal ideation and is assessed by a mental health practitioner at these sites to not require secondary mental health services and be suitable for SWISH.
Exclusion criteria
Anyone who following assessment by a mental health practitioner meets at least one of the following criteria:
Unable to give informed consent;
Requires admission to a mental health inpatient unit;
Requires secondary mental health services;
Assessed as high risk for violence;
Known or assessed to have a severe mental illness and require other services;
Is under a current and active care and treatment plan with adult mental health services;
Is unable to communicate in English.
At any point, if a recruited patient meets any of the exclusion criteria they are withdrawn from the study, but their anonymised data will be retained for analysis.
Power and sample size
The power analysis is based on the primary outcome measure, BDI-II score. Based on published reviews and papers, a 5–10% change in the BDI-II score represents a clinically important difference and the SD varies between 6 and 10,39–41 which provides an effect size of ∼0.53. To detect a 5–10-point difference in the BDI mean score between intervention and the control conditions, with 80% power, requires a sample size of 120 (60 in each arm of the trial).
As this study is assessing feasibility for a full trial of a new intervention, we cannot anticipate the attrition rate, but will use the attrition at 6 and 12 weeks to inform the full trial. For the same reason there are no stopping guidelines, except the complete failure to recruit to the required sample size.
Randomisation
We performed an individual randomisation of the patients from the study population who met the inclusion criteria. As this is a feasibility study, we did not use any stratification for randomisation (eg, stratify between ideators and self-harmers). We will be looking at differences during analysis, and should there be any significant differences we intend to incorporate stratification in the future full trial. Patients are randomised by the intervention practitioner after completion of baseline assessment using an online randomisation tool managed by Swansea Trials Unit. Patients are randomised with a ratio of 1:1 to intervention and control and used random numbers generated from the New Cambridge Statistical Table.42
Intervention
The intervention is a 4–6-week enhanced contact programme which is a mix of face-to-face and telephone contact. It deliberately steers away from being a psychological or medical service; rather it is based on linking individuals into social support networks and encouraging access to, and engagement with, relevant services. It is an additional rather than alternative service for support services already in place, and encourages patients to engage with existing services. As such, as long as patients are not receiving support from secondary mental health services (an exclusion criteria based on higher support needs of secondary mental health service users); there is no contraindication to involvement with SWISH.
An awareness of local third-sector services is key to the role of the practitioner. The intervention can be delivered by a skilled individual who has experience of working with people with mental health issues. The practitioners delivering the intervention in this trial have worked in mental health services but are not registered mental health practitioners. They have experience of working in Carmarthenshire within mental health services and/or developing mental health services for vulnerable populations. By not requiring practitioners to hold registrations, the intervention is more cost-effective to deliver as it relies on locality-based training and awareness above registration. A condition of employment is to have enhanced disclosure and barring service clearance before initiation. The practitioners receive training on mental health service delivery in Carmarthenshire from an advanced nurse practitioner in mental health services. Formal clinical supervision with the advanced nurse practitioner is once a fortnight or more depending on requirements; the supervisor is available at all times on the phone for immediate questions, and monitors the delivery of the intervention and patient contact.
The intervention encourages individuals to link with local services. In this trial some of the agencies patients are linked into include Men's Shed projects, adult education courses, knitting groups and volunteering services, as well as services supporting individuals with drug and alcohol issues and domestic abuse. The choice of service is decided alongside the patient based on the type of support and engagement they would like. The intervention primarily focuses on the social dimensions of a person's life; the medical and psychological needs of the patient will have been assessed prior to the patient's referral to SWISH. If at any time during the intervention the practitioner is concerned that these needs may be escalating and require specialised support, or there is a crisis situation this will be immediately discussed with the clinical supervisor who will refer the patient accordingly; and SWISH will continue to support the patient for the duration of the intervention, or until they meet the exclusion criteria and are engaged with relevant support services.
The first patient–practitioner contact is as soon as possible after baseline has been collected by a research assistant. At the first meeting, the patient is encouraged to discuss recent events and explore the reasons which they feel led to their current situation. This meeting typically lasts about an hour. The practitioner works with the patient to identify the main social issues they feel precipitated this and discuss relevant agencies that may be able to offer support and information. A plan of action is then worked out with the patient where the patient is given suggestions for services that they can link in with. This plan is written up by the practitioner and sent to the patient with information and contact details for services.
TAU for patients with low or no mental health history who present to the hospital emergency department is usually a referral back to the GP, although some might be signposted to services in the community usually by way of leaflets provided. TAU for patients referred by their GP to local primary mental health support services is an assessment within 4–8 weeks and appropriate referral or signposting. This intervention goes beyond signposting to assertively link the patient with relevant services to embed them within a supportive network at a time of emergency and vulnerability to try and ameliorate the negative impact of the self-harm episode. This ‘assertive community linkage’ is the basis for the intervention. It differs from signposting by actively encouraging patients to contact relevant community agencies who can provide specialised support and establish a supportive resource to help manage future periods of stress. The practitioner can follow-up whether they have made contact with any agencies and explore reasons for reluctance to engage. Where necessary, the practitioner can make a referral or initiate contact and support for patients, for example, one patient was keen to attend a local craft group but felt scared to attend alone, the practitioner made contact with the service and arranged for the patient to meet with the craft group coordinator alone prior to attending the group to discuss her fears and be reassured.
Follow-up contacts are a mix of face-to-face and telephone contacts depending on agreement and discussion with the patient. Patients are seen at a location that is convenient to them, this includes home visits; however, as part of the community linkage patients are encouraged to engage outside of the home and so meetings are held in local spaces including GP surgeries, coffee shops and arts centres. This is especially the case for patients who do not feel confident or willing to actively engage with available social networks or for whom there is no local service that suits their needs. In such instances, the practitioner provides a purely contact and listening service, encouraging the patient to leave the house and meet for a chat. Details of all contacts are logged on the FACE electronic recording system used by HDUHB as their healthcare notes recording system. The number and nature (face-to-face or telephone) and length of contacts vary depending on patient need and are mutually decided between the patient and practitioner. The minimum number is four and the maximum is usually six, with the first and final contact always being face to face. As this is a feasibility study we have been flexible with the final number of sessions to accommodate patients who may be waiting for another service. In this situation SWISH provides support until they are engaged with another provider. This has resulted in up to eight sessions in three cases.
This is an important feature of the intervention where besides providing a stand-alone service linking individuals to community services it acts as a bridging service for patients. Patients referred to local primary mental health support services and those who have been referred to other (non-secondary) mental health support services such as psychological therapy services typically face a 4–8-week wait for assessment. The intervention provides a point of regular contact and support during this waiting period.
Control
The control group receive TAU from the service they presented to. This ranges from no action, discharge to GP, signposting to community services and/or referral to psychological therapy services. These treatments do not conflict with SWISH.
Outcome measures
The primary outcome measure is the BDI-II, measuring depressive symptoms as this was the primary outcome measure in the Australian study. For the same reason our secondary outcome assesses whether a social intervention leads to overall increase in well-being, as measured by the MANSA. Additionally we are collecting data on whether the intervention reduces rates of representation to mental health services as measured by the CSRI and long-term follow-up of service use by SAIL.
Our choice of primary and secondary outcomes is based on remaining as close to the Australian study as possible based on the information available. For a further trial, we will seek to collect data on social outcomes, exploring the type and nature of social networks that individuals engage with as an outcome of the intervention.
Assessments
All patients complete assessments at baseline (before randomisation), 4 and 12 weeks. Those who fall in to the 6-month period while the study is running are invited to complete a 6-month assessment. A 1-year follow-up will be conducted by SAIL.
Baseline assessments
The baseline assessment consists of the BDI-II, MANSA and CSRI. Patients are asked to complete these questionnaires as soon as possible after they consent. The questionnaires are designed to be self-completed, however the researchers read out the questions and fill in the responses where requested by patients. Researchers note whether they are required to read out any/all questions, and any questions patients have asked for clarity or elaborated on while completing the questionnaire pack. Patients are given a £10 voucher for their time after completing the baseline assessment. All contact with patients is recorded on the Health Board electronic patient contact recording system.
Follow up assessments
Four-week follow-up
Follow-up assessments are conducted with the same questionnaires (BDI-II, MANSA, CSRI) at 4 weeks. Patients are given no incentive at the 4-week assessment.
Twelve-week follow-up
Patients are asked to complete the BDI-II, MANSA and CSRI. Patients who complete the 12-week assessment are given a £20 voucher for their time.
Additionally at the 12-week data collection patients are asked to complete an evaluation form of their experience of SWISH. There is room for additional comments. The researcher asks for the feedback on the contact and this is recorded verbatim for qualitative analysis, and to provide assessment of the service in the patient's own words. Initially, these data were only included for intervention patients; however, we have begun to collect it for control as well after control patients commented on the support they felt they were receiving from the researcher collecting assessment data.
Six-month follow-up
Early recruits are invited to take part in a 6-month assessment where possible, and a further £10 voucher is given for their time.
One-year follow-up
Patients have consented to being linked in anonymously to the SAIL Databank (http://www.saildatabank.com/). SAIL contains routinely collected anonymous data for Wales. We will use the SAIL data for the number of visits (or contacts) to primary (GP) and secondary care (hospital admission and emergency department visit) by the SWISH patients for the year preceding and the year following the intervention. We will be collecting the counts of contacts that relate to self-harm, suicidal ideation and depression.
Blinding
There is no blinding of researchers or participants. The information sheet clearly states the intervention is a 4–6-week contact programme. The researcher advises all patients that the intervention practitioner will be in touch within a few days if they are randomised to the intervention. It has proved impractical and almost impossible to blind the researcher conducting the assessments as at the week 4 assessment, there is often a clash with intervention meetings for the patient. It would be preferable for all assessments to be collected by the researcher; however, due to staffing issues in this trial and to minimise the time commitment on the part of the patient and maximise data collection, intervention patients are given the option to complete the 4-week assessment at an intervention meeting with the practitioner rather than the researcher. Some intervention patients prefer just to have one SWISH contact at the 4-week stage rather than find time for separate meetings with practitioner and researcher. The intervention always includes a discussion of how they are feeling and their social connectedness, so the administration of the questionnaire at the time of intervention avoids some repetition on the part of the patient where the questionnaire is being read to them. However, the majority of questionnaires are completed by respondents individually and put into an envelope after completion, so the practitioner is unaware of their responses. We acknowledge that this might introduce some bias into the methodology; but for a feasibility study and due to the reasons outlined above, we feel that maximum data return should be prioritised.
Trial management group
A trial management group, whose members include study the applicants (academics and Health Board practitioners), service users and representatives of community organisations meets once a quarter to monitor progress and discuss any issues arising. The chief investigator also attends a monthly trial managers meeting at the Swansea Trials Unit to update on progress and discuss the project.
Analysis
Statistical analysis
Our analysis will be based on the primary and secondary outcome measures which are the BDI-II score and MANSA and CSRI. The hypothesis of interest is that the change scores on these outcome measures will be significantly different in the intervention group compared with the control group. We will analyse changes in all outcome measures between baseline and follow-up at 4, 12 weeks and (where collected) 6 months by adopting repeated measures analysis of variance. We shall use the pertaining values of the outcome measure under analysis and consider participants' demographic characteristics (eg, age, marital status, sex education level) as covariates. Since both the BDI-II score and MANSA are well validated and use outcome measures, respectively, for depression and ‘quality of life’, they do not require checking of internal consistency.
As described above, we will be using SAIL to compare the number of contacts to primary and secondary care made by the SWISH participants before and after the intervention between the case and control group. We will use t-tests to assess any differences between the groups.
We will adopt the intention-to-treat population, consisting of all participants randomly assigned to the intervention and control. To deal with the missing values, we shall summarise the frequency of missing data for each variable, which affects the effective sample size and hence statistical power. If there is no reason to suspect that data are not missing completely at random, we shall consider the use of appropriate imputation methods to ameliorate the problem of missing data; otherwise, the trial statistician and chief investigator will further discuss the patterns in missing data. Outcome descriptions, summaries and comparisons will be expressed in accordance with appropriate CONSORT guidelines,43 including estimates with 95% CIs to summarise two-tailed tests at the 5% significance level.
Health economics
Health service resource use in primary care, secondary care and the community is collected using the CSRI from participants in both arms of the trial at baseline, 4, 12 weeks and 6 months. Questions will relate to all health service contacts (hospital appointments, hospital stays, GP contacts, visiting nurse appointments, etc) and prescription medicines dispensed during the trial period. Patient recall has been shown to be a valid method for collecting health service resource use data over this period (and, as clinical records are often fragmented, and sometimes unavailable, across different parts of the health service) patient-reported data are likely to remain more readily available and less costly to collect for research purposes.44 A descriptive analysis of CSRI data, along with estimates of the cost of providing the intervention, will provide a comparison of participant resource use between the intervention and control groups, and will provide indicators of the main resource use (and associated costs) drivers of those receiving the intervention.
The CSRI data will be summarised and presented descriptively. The resources used and associated costs will be summarised. The costs of the intervention will be estimated. These data will be used to compare the costs of the intervention and usual care and to inform the calculation of incremental costs. The sources of costs will be fully referenced to aid transparency of the analysis. Where possible, published unit costs will be used (eg, Personal Social Services Research Unit (PPRU) Costs of Health and Social Care, British National Formulary, National Health Service (NHS) reference costs) using the most recent published sources—2014/2015. Costs (mean and SD and/or 95% CIs) or non-parametric equivalent (median and IQRs) will be presented.
Dissemination
Findings will be fed back to the Health Board and to the third sector through presentations and contributions in local publications. Outcomes will be published in peer-reviewed journals and at national and international conferences.
Discussion
This paper describes the study protocol for a feasibility study for a RCT of an enhanced contact intervention for people who present with self-harm or suicidal ideation and do not require secondary mental health services.
Several limitations apply to this study. First, interventions tend to have a high attrition rate. Dropout can introduce a selection bias and pose a threat to validity. However, we are able to report a high rate of recruitment at 100% of our target and successful intervention completion at 77% across the whole sample. If those who were withdrawn from the study (due to meeting exclusion criteria) are excluded, the completion rate for all those eligible to complete the intervention rises to 83%.
Second, the services that SWISH is able to provide are limited. Encouraging social linkage is largely dependent on the availability of relevant options for individuals. In a large, predominantly rural county,45 there are limited choices, which are further reduced if there is no access to transport. A social linkage programme will be able to offer more resources in areas where there are more agencies and community services to engage with. The location and accessibility of services may affect the generalisability of findings to urban populations.
Third, while the assessments are intended to be self-completed, a lack of confidence on the part of patients in completing questionnaires themselves meant that a substantial number were read out by the researcher. This may have affected responses.
Finally, as discussed above, the study was conducted unblinded. Attempts were made to blind the researcher collecting assessments, however, this was not practical.
However, even with limitations, the findings will offer an insight into the applicability of a social intervention to be alongside medical and psychological interventions. SWISH offers a short-term crisis response to engage patients while they are waiting for referrals to medical and community services. Often there are 4–8-week waiting lists to be seen by other services. SWISH fills this void and at the very least it offers a contact and listening service to individuals at a vulnerable time. By engaging with patients while they are waiting for other appointments it can help reduce rates not attending appointments with other health and social care services by encouraging attendance. Through embedding patients in to existing local organisations and services, SWISH helps to provide a source of support for future stressful times.
References
Footnotes
Contributors NA is the chief investigator and drafted the protocol, designed the study and organised and supervised implementation. PH conceived the study in conjunction with RJ and AJ; AJ and PH provided methodological expertise. SI is the trial statistician and developed the statistical analysis strategy. RJ is the clinical supervisor and provides expertise and supervision to practitioners. PA and SH developed the health economics strategy. AK and CD worked on the data collection and data management. NA, AJ and SI worked on the preparation of this manuscript, and all authors provided comments on drafts and approved the final version.
Funding The trial is funded by Health and Care Research Wales (Ref: SCR-12-05) and sponsored by Swansea University (Ref: SKR-518).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Wales Research Ethics Committee (REC) 6.
Provenance and peer review Not commissioned; externally peer reviewed.