Article Text

Abstract
Background With recent focus on methicillin-resistant Staphylococcus aureus (MRSA) screening, methicillin-susceptible S. aureus (MSSA) has been overlooked. MSSA infections are costly and debilitating in orthopaedic surgery.
Methods We broadened MRSA screening to include MSSA for elective orthopaedic patients. Preoperative decolonisation was offered if appropriate. Elective and trauma patients were audited for staphylococcal infection during 2 6-month periods (A: January to June 2013 MRSA screening; B: January to June 2014 MRSA and MSSA screening). Trauma patients are not screened presurgery and provided a control. MSSA screening costs of a modelled cohort of 500 elective patients were offset by changes in number and costs of MSSA infections to demonstrate the change in total health service costs.
Findings Trauma patients showed similar infection rates during both periods (p=1). In period A, 4 (1.72%) and 15 (6.47%) of 232 elective patients suffered superficial and deep MSSA infections, respectively, with 6 superficial (2%) and 1 deep (0.3%) infection among 307 elective patients during period B. For any MSSA infection, risk ratios were 0.95 (95% CI 0.41 to 2.23) for trauma and 0.28 (95% CI 0.12 to 0.65) for elective patients (period B vs period A). For deep MSSA infections, risk ratios were 0.58 (95% CI 0.20 to 1.67) for trauma and 0.05 (95% CI 0.01 to 0.36) for elective patients (p=0.011). There were 29.12 fewer deep infections in the modelled cohort of 500 patients, with a cost reduction of £831 678 for 500 patients screened.
Conclusions MSSA screening for elective orthopaedic patients may reduce the risk of deep postoperative MSSA infection with associated cost-benefits.
- BACTERIOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Simple adjustment of laboratory method allowed detection of methicillin-susceptible Staphylococcus aureus (MSSA) as well as methicillin-resistant S. aureus.
Decolonising MSSA-positive orthopaedic patients before surgery protected them from deep MSSA infection in bone and joints.
The study highlights an important and costly deficit in the current national screening tool for high-risk surgery.
Study limited due to one site setting in Scotland.
Costs based on UK National Health Service (NHS) practices only.
Introduction
Approximately one in three people are colonised with Staphylococcus aureus (methicillin-susceptible S. aureus, MSSA) in contrast to the current low rate of methicillin-resistant S. aureus (MRSA) colonisation in the UK.1 Carriage is genetically determined and represents a risk for infection, especially when admitted to hospital for surgery. Endogenous MSSA is a common cause of postoperative infection.1 ,2 This risk is recognised by choice of specific antistaphylococcal antibiotics for surgical prophylaxis, especially high-risk procedures such as orthopaedic and vascular implant surgeries.3 ,4
Concern over increasing MRSA led to the introduction of a national MRSA screening programme for all hospital admissions, including elective surgical patients.5 The subsequent increase in screening swabs meant that laboratories had to streamline their methods and MRSA chromogenic agar was chosen to aid rapid identification.5 Unfortunately, this agar cannot yield MSSA. Thus, a patient might be deemed negative for MRSA carriage but could still be positive for MSSA. If elective patients awaiting orthopaedic implant surgery demonstrate MSSA carriage then they are known to be at risk of postoperative MSSA infection.2 ,3
Owing to ongoing sporadic MSSA infections among orthopaedic patients, our health board approved the decision to broaden preoperative screening to include MSSA as well as MRSA for elective implant patients from December 2013. Trauma patients receive immediate care and proceed to surgery without prior screening. This paper describes an audit of postoperative staphylococcal infection among all elective and trauma orthopaedic patients at one hospital within two separate 6-month periods: January to June 2013 (period A: MRSA screening only) and January to June 2014 (period B: screening for MSSA and MRSA). We compare and contrast the MSSA infection rate between all patients receiving orthopaedic surgery during both study periods and present an evaluation of the change to health service costs from a decision to adopt the enhanced screening programme.
Methods
The study hospital is a 550-bed acute district general hospital with 24-hour accident and emergency (A&E) department. The hospital offers a range of services including management of elective and trauma patients for orthopaedic surgery. Trauma patients are admitted through A&E and receive immediate surgery if appropriate. Elective patients attend the preassessment clinic for evaluation of surgical fitness, including MRSA screening in accordance with national protocol.5 Orthopaedic services are delivered by four consultants responsible for >95% of all implant surgeries undertaken by the hospital, which is the largest orthopaedic referral centre for the health board. A number of severe MSSA implant infections occurred in 2012, unrelated in time or space. It was decided to pilot an enhanced screening programme managed by preassessment for 3 months (July to September) in 2013 and audit the effect. Thus, patients were swabbed as usual (nasal, perineal±wounds) and request forms were tagged so that the laboratory could distinguish specimens from orthopaedic patients and process them for MSSA as well as MRSA. In the event of cancellation of surgery, some patients were recalled for repeat screening.
Laboratory methods
Swabs were transported to the laboratory and processed on the day of collection. Standard operating protocol was changed to encompass preliminary isolation of S. aureus by switching from MRSA chromogenic to S. aureus identification (SAID) chromogenic agar. Characteristic blue colonies were further tested for coagulase production (Staphylase) and indeterminate reactions were confirmed with tube coagulase. Positive isolates were characterised by automated technology (Vitek) including antibiotic susceptibilities. The results were authorised by the consultant microbiologist who reported appropriate susceptibilities (flucloxacillin; clarythromycin; vancomycin; gentamicin and mupirocin).
Patient decolonisation
Authorised results were fed back to preassessment. A standard letter detailing MSSA isolation and management options was sent to the orthopaedic consultant responsible for the patient. Confirmed MSSA carriage at skin sites was treated with 5 days Naseptin (chlorhexidine hydrochloride 0.1%; neomycin sulfate 0.5%) nasal cream applied three times a day and daily chlorhexidine gluconate 4% body washes. MRSA-positive patients received the same regimen but with mupirocin 2% (Bactroban) nasal cream rather than Naseptin. A known MSSA-positive patient would occasionally present for surgery without having received any clearance therapy; these patients were offered preoperative Naseptin and a chlorhexidine shower. MRSA-positive patients were deferred from surgery unless they had received the appropriate decolonisation protocol. Surgical prophylaxis for all orthopaedic patients was flucloxacillin±gentamicin or a glycopeptide, in accordance with local prescribing policy.
Audit strategy
Following encouraging results from the 3-month pilot study, additional MSSA screening for elective orthopaedic patients was implemented from mid-December 2013. We decided to conduct a formal audit of patient outcome in order to evaluate the screening programme. Two periods were chosen: the first 6 months in 2013, when only MRSA screening was performed, and the same 6-month period in 2014, when both MSSA and MRSA screenings were performed. These periods were chosen to reflect seasonal variation, bypass the effect from the 2013 pilot study and permit sufficient ‘wash-out’ time between old and new screening policies. We included orthopaedic trauma patients admitted during the same periods as control because these patients proceed to immediate surgery without screening. There were no policy changes in the management of either trauma or elective orthopaedic patients during the study period, including estates-related or infection control programmes.
Data retrieval
The hospital database was searched for all orthopaedic patients attending preassessment from 1 January to 1 July 2013 (period A) and for the same 6-month period (period B) the following year, 2014. A separate search of the microbiology database yielded every orthopaedic patient submitting one or more samples requesting a test for, or positive for, S. aureus from 1 January 2013 until 31 December 2014. Patients were then cross-checked against microbiology and hospital records in order to identify all elective and trauma patients presenting within the two periods; those screened for MRSA, those screened for MSSA and MRSA, patients colonised with MRSA or MSSA; and all patients identified with postoperative staphylococcal infection within 1 month after surgery (early-onset) or after 1 month following surgery (late-onset). Patients were followed up for 1 year after surgery. New patients presenting outside the two study periods were excluded. Postoperative patients who missed prior screening and subsequently developed infection were offered relevant screening. The number of return trips to the operation theatre, additional surgical interventions, intensive care unit (ICU) admission, A&E and outpatient attendance, microbiological investigations and length of stay (LOS) were documented for all patients with postoperative infection.
Cost data for screening activities and for laboratory and clinical management of infection were obtained from a number of resources, both local and national. Laboratory consumables were recovered from manufacturers' data at nationally agreed National Health Service (NHS) cost; biomedical scientist, hospital consultant, general practitioner (GP) and nurse time costs were based on national pay scales, with mid-point values selected for calculation. Health board data were used to estimate the costs of laboratory processing for individual tests, such as wound swabs, blood cultures and aspirates, etc. These included consumables, staff time, laboratory overheads (including quality control, training and waste disposal) and specimen transport. The costs of all antimicrobial drugs and other products were retrieved from the 2015 British National Formulary (BNF) Online database at http://www.bnf.org/products/bnf-online/. Clinical costs, such as ICU, hospital bed-days, surgical procedures and outpatient and A&E attendances were taken from NHS Scotland Tariffs published data (2013/2014) available via: http://www.isdscotland.org/Health-Topics/Finance/Scottish-National-Tariff/
Infection definitions
Each patient with postoperative MSSA infection was investigated to ascertain the severity of infection and subsequent management.6 ‘Superficial’ surgical site infection was defined as skin and soft tissue involvement only; ‘deep’ infection (also organ/space infection) was defined as infected implant necessitating intravenous antibiotics and further surgery. Patients with postoperative staphylococcal infections unrelated to the surgical site were not included.
Since it was not possible to calculate the total number of trauma patients presenting at the A&E department during the study periods, we selected all those who received emergency surgery in trauma theatre. This provided the denominator for sepsis rates among trauma patients during both study periods. We were able to ascertain the total number of elective patients who attended preassessment and this was used to calculate the overall sepsis rates among elective orthopaedic patients for both study periods.
Statistical analysis
CIs for the risk ratio were calculated using exact sample methods. Wilson's limit was used for the CIs for the proportion. Tests of association were carried out using Fisher's exact test. The joint effects of elective compared with trauma surgery and period were investigated through a logistic regression using a log link. R V.3.2 was used for the analysis, together with the epitools and Hmisc libraries.
Cost modelling
The expected change to total health services costs were modelled for a cohort of 500 elective orthopaedic patients. The extra costs from additional MSSA screening were included as were the cost-savings from changes to the number of cases of superficial and deep infection. All data uncertainties were included by fitting prior statistical distributions and running a probabilistic analysis of 1000 simulations. Parameters that describe the costs of additional MSSA screening (table 1) had uncertainties represented by a 10% positive and negative variance. Information on the resources used and subsequent treatment costs (table 2; see online supplementary appendices 1–3) for cases of deep infection were used to update a prior γ distribution to show the costs of treating a case of deep infection. The cost of treating a superficial infection is shown in online supplementary appendix 4 and uncertainties were represented by a 10% positive and negative variance. The relative risk of infection from additional screening over baseline screening was estimated from the data in table 3. Prior uncertainties (online supplementary appendices 5 and 6) were specified with a statistical distribution using calculated log relative risk and SE. Applying the starting risk of infection shown in table 3 under conditions of baseline screening provides estimates of the starting numbers of infections among the cohort. These were modified by the uncertain relative risks shown in online supplementary appendices 4 and 5 to predict the change in the number of infections (see online supplementary appendices 7 and 8). The expected cost of the enhanced screening (see online supplementary appendix 9) and the change in total costs was estimated.
Supplemental material
Additional costs of enhanced staphylococcal screening
Outcome of 16 postoperative deep MSSA infections among elective orthopaedic surgery patients during two 6-month periods (2013–2014)
MSSA infection outcome of all orthopaedic patients during two 6-month periods
Results
During 1 January to 1 July 2013 (period A), 232 patients underwent preoperative assessment before elective orthopaedic surgery compared with 307 patients during 1 January to 1 July 2014 (period B; table 3). Over the same two 6-month periods, 447 patients received emergency orthopaedic surgery during period A compared with 352 patients during period B. There were also an unknown number of patients admitted directly from outpatient clinics or transferred from other hospitals who underwent orthopaedic surgery (table 3).
During period A, 2 (0.45%) and 10 (2.24%) of 447 trauma patients had superficial MSSA and deep MSSA infections, respectively. These were similar to infection rates for trauma patients during period B (superficial: 4 of 352 (1.14%); deep: 5 of 352 (1.42%); p=1, Fisher's exact test; table 3). Of the 232 elective patients in period A, 4 (1.72%) patients had superficial MSSA and 15 (6.47%) had deep MSSA infections following implant surgery; during period B, 6 (2%) of 307 elective patients had superficial MSSA infection with just 1 (0.3%) deep infection (p=0.002; table 2 and 3). There is a significant interaction between trauma and elective surgery and each period on the risk of MSSA infection (p=0.044). Among trauma patients the risk ratio of any MSSA infection was 0.95 (95% CI 0.41 to 2.23) in period B compared with period A, while the corresponding risk ratio was 0.28 (95% CI 0.12 to 0.65) for elective patients. For deep MSSA infections, the risk ratio was 0.58 (95% CI 0.20 to 1.67) for trauma patients and 0.05 (95% CI 0.01 to 0.36) for elective patients (p=0.011). Four additional deep MSSA infections were identified during period B in patients who had not attended preassessment or received prior screening (table 3). They are not included in the above analysis.
Of the 307 patients screened by preassessment in period B, 89 (29%, 95% CI 24% to 34%) were identified as carriers. This supports the premise that around one-third of people are colonised with coagulase-positive staphylococci.1 There was only 1 (0.3%) deep MSSA infection among the 307 screened elective patients, whereas there were 30 (2.9%) deep MSSA infections among all the unscreened patients (n=1031), whether managed as elective or trauma (table 3). Formal comparison of patient cohorts is not considered further because we did not adjust for operation type, age or length of operation, all of which differ between trauma and elective patients. Although the numbers are small, elective patients were 2.89 times (95% CI 1.32 to 6.33; p=0.009) more likely than trauma patients in period A to suffer deep MSSA infection (elective 6.47% vs trauma 2.24%).
Patients with confirmed postoperative MSSA infection (superficial and deep) who missed prior MSSA screening were investigated further. Of the 44 patients with MSSA infection, 17 were screened and 14 of these demonstrated nasal MSSA (table 3). These figures include four elective patients admitted during period B who did not attend preassessment. There were three patients deemed negative following prior screening who suffered postoperative MSSA infection. Repeat nasal screening after confirmation of postoperative MSSA infection then established presence of MSSA.
Before and throughout the entire study period, patients were screened for MRSA in accordance with national guidelines.5 This occurred for elective patients before surgery but trauma patients usually received surgery before the screening took place. The number of MRSA infections among orthopaedic patients was negligible for both periods (A: one patient; B: no MRSA infections), although superficial carriage was occasionally identified. There were no patients with both MSSA and MRSA at the same time. Given that there were so few MRSA infections, these patients are not considered further.
Cost modelling
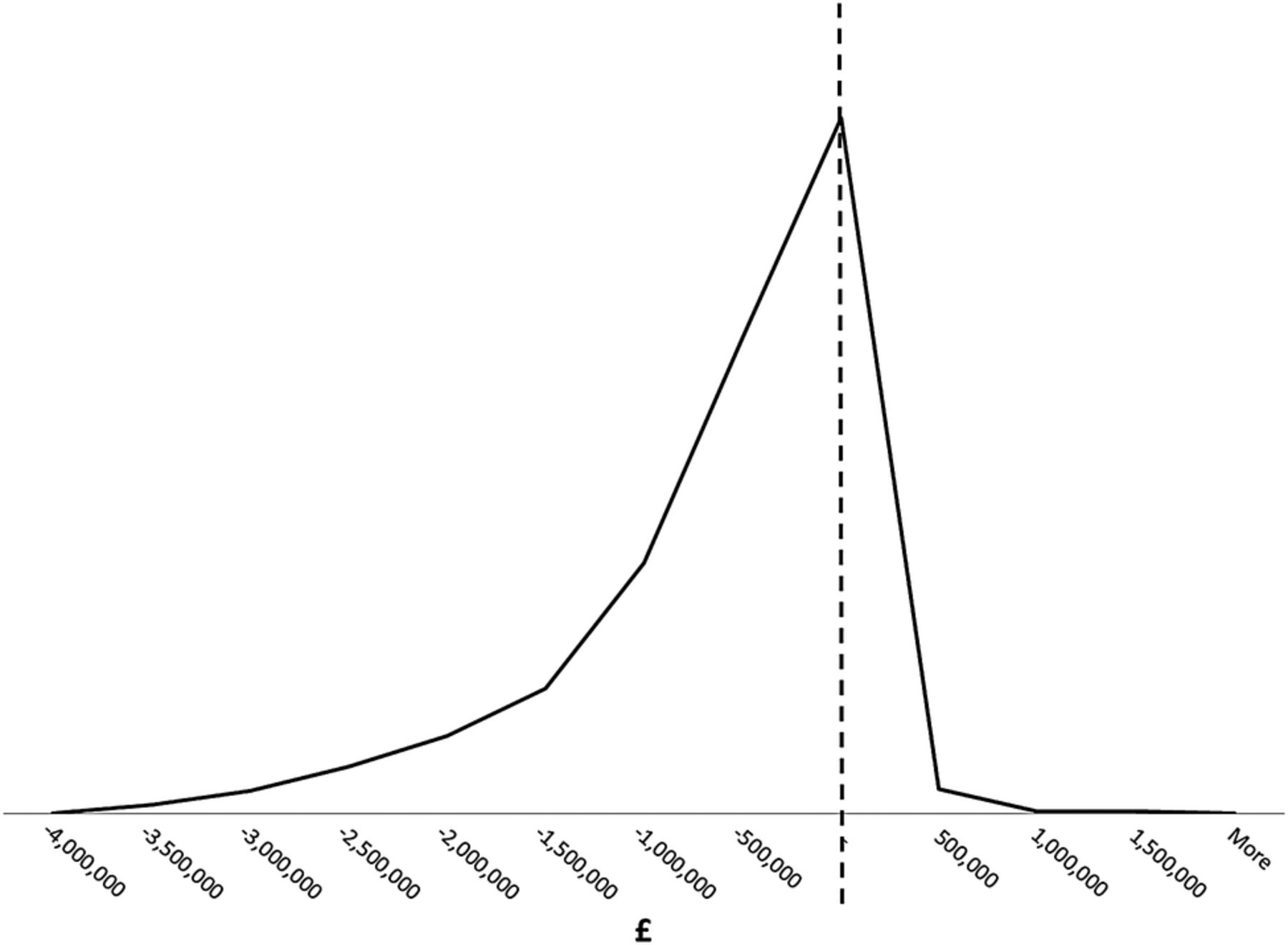
We estimate that enhanced screening costs £18 269 for 500 patients screened (table 4). There would be an additional 3.04 superficial infections arising but 29.12 fewer deep infections. The overall change in costs would be savings of £831 678; this is caused by the high costs of treating a deep infection that are avoided due to enhanced screening (see online supplementary appendix 3). The uncertainty in the estimated change in total cost is shown in figure 1. Interpreting this plot for decision-making suggests there is an 86.8% chance that implementing enhanced screening is cost-saving. A rational and risk neutral decision maker should adopt enhanced screening, and on average this will yield a saving of £831 678 per 500 patients screened.
Statistical summary of relative risks, screening costs, infections prevented and potential cost-savings
{kind=link}
Figure showing uncertainty in estimated change to total cost with enhanced screening of elective orthopaedic patients awaiting implant surgery. The area to the left of the dashed line is 86.8% of the distribution. This means that there is an 86.8% chance that implementing enhanced screening is cost-saving (see text).
Discussion
Given the focus on MRSA, it is not surprising that MSSA infections have continued unabated in UK hospitals. While the rate of MRSA bacteraemia has been decreasing since 2008, the MSSA bacteraemia rate has continued with little change.7 ,8 This study investigated patients receiving orthopaedic implant surgery, and found that MSSA carriage remains an important risk factor for postoperative infection, whether admitted for trauma or as a planned elective.
Most of the infections identified during the period without MSSA screening were classified as ‘deep’, which mandated the need for further surgery. Previous reports state that the average cost of a failed implant varies from £7000 to £36 000 depending on the site, debridement, antibiotics and/or revision surgery.9 ,10 These figures do not necessarily include extra LOS. We found that the average total cost of managing a deep MSSA implant infection occurring in period A was about £55 500, which exceeds the figures quoted. Since we included parameters such as LOS, intensive care days, microbiological tests, A&E and outpatient attendance, it is possible that our figures are a more realistic illustration of additional costs due to postoperative orthopaedic infection. A recent paper from a London teaching hospital (with a domiciliary antibiotic facility) found that the average LOS for 45 patients needing total knee arthroplasty was 21.49 days.10 Our 16 patients had an average LOS of 40 days (table 2), although if one single patient who stayed in hospital for 313 days is removed, 15 patients had an average LOS of 21.3 days, which is similar to the London hospital data.
There are caveats to our findings when balancing cost-savings from fewer failed implants against the screening costs (table 1). Broadening laboratory protocols to include MSSA identification were cost neutral due to the use of less expensive agar, but there were additional administrative and managerial costs for preassessment, orthopaedic secretaries and clinicians. Most of the product costs were absorbed by the hospital (nasal creams and antiseptic washes) but some patients obtained a prescription from their GP. Furthermore, some operations were postponed, in which case the patients concerned were asked to attend preassessment for repeat screening. Given this, it is possible that the overall cost of the screening programme (∼£18 000) may have been underestimated. The savings made from reduced numbers of deep orthopaedic infections were substantial, however, and it is assumed that they more than covered the costs of the screening initiative.11 ,12
The study has some strengths and limitations. Simple adjustment of laboratory method allowed detection of MSSA as well as MRSA without compromising laboratory staff or usual practices. The amendment to standard operating procedure was cost neutral. Decolonising MSSA-positive orthopaedic patients before surgery appeared to protect them from deep MSSA infection in bone and joints, although we accept the causal nature of the association. The study highlights an important and costly deficit in the current national staphylococcal screening tool for high-risk surgery. The findings are limited due to the single site setting in a relatively deprived area of Scotland, however, and the fact that costs are based on UK NHS practices only. This means that the reported outcome may not apply to other orthopaedic units, although they may be relevant during an ‘outbreak’ situation.
MSSA isolates were not retained for further molecular characterisation so we could not demonstrate identity between colonising and infecting strains in the same patient. This was due in part to the retrospective audit for period A. There have been many previous studies demonstrating genotypic links between colonising strains and postsurgical infection due to the carrier strain.1 ,11 We had no wish to duplicate this work. However, we did notice indistinguishable antibiograms between MSSA isolates recovered from screening swabs and those submitted days or weeks later from samples taken to confirm postoperative infection. Occasionally, there were multiple samples from the same patient, including blood cultures, aspirate and tissues, taken before or during revision surgery that generated unique antimicrobial susceptibility patterns, including minimal inhibitory concentration (MIC) values, to key antibiotics. We believe that patients habitually colonised with their own unique strain are at risk from infection due to their carried strain when compromised by a major surgical intervention.1–3 Three patients, originally negative for MSSA carriage, were found to be positive following confirmation of postoperative MSSA infection. They may illustrate transient staphylococcal carriage, which also poses an infection risk for surgical patients.1 An alternative explanation is that original screening swabs did not detect a colonising strain; or it failed to grow, or was overlooked by the laboratory. PCR might ameliorate some false-negative results, but this method requires costly consumables and delivers increased numbers of false positives.13
MRSA bacteraemia rates have fallen across the UK over the past 10 years.7 This fall may be attributable to the universal MRSA screening programme, which recommends the use of MRSA chromogenic agar.14 Selective agar facilitates the identification of MRSA but inhibits the growth of MSSA. This might explain why MRSA bacteraemia rates have reduced in the UK, whereas MSSA rates have not. These trends contrast with those in Australia, where MRSA chromogenic agar is not universally employed and both MRSA and MSSA rates have decreased in parallel over the same time period.15
In conclusion, broadening the national screening policy to include MSSA for elective orthopaedic surgery patients awaiting implant procedures identified preoperative carriage in nearly one-third of the patients. The screening programme may have facilitated a reduction in deep postoperative infection in the screened patient cohort. The cost-benefits from enhanced screening in this high-risk population of surgical patients are substantial.12
Acknowledgments
The authors would like to acknowledge all the staff in preassessment. They also thank orthopaedic secretaries and the Surgical Clinical Coordinator. The authors wish to dedicate this study to one of the co-authors (FC), who died before the study was completed.
References
Footnotes
Contributors SJD conceived, planned, managed and collected study data; she also analysed data and wrote the paper. AG, KP, AE and RM introduced enhanced screening into preassessment, managed colonised patients and performed all surgeries. They also managed postoperative patients and collected outcome data. FC was responsible for implementing the microbiology SOP in the laboratory, and searching hospital and laboratory databases for all relevant data. CR performed statistical analyses and NG provided cost-modelling for all study variables.
Funding The study was supported by NHS Lanarkshire.
Competing interests None declared.
Ethics approval Research & Development Department, NHS Lanarkshire.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All original data for the study are available from the lead investigator (SJD) by email request.