Article Text

Abstract
Objectives Public and patient engagement (PPE) is fundamental to healthcare research. To facilitate effective engagement in novel point-of-care tests (POCTs), the test and downstream consequences of the result need to be considered. Sequential simulation (SqS) is a tool to represent patient journeys and the effects of intervention at each and subsequent stages. This case study presents a process evaluation of SqS as a tool for PPE in the development of a volatile organic compound-based breath test POCT for the diagnosis of oesophagogastric (OG) cancer.
Setting Three 3-hour workshops in central London.
Participants 38 members of public attended a workshop, 26 (68%) had no prior experience of the OG cancer diagnostic pathway.
Interventions Clinical pathway SqS was developed from a storyboard of a patient, played by an actor, noticing symptoms of oesophageal cancer and following a typical diagnostic pathway. The proposed breath testing strategy was then introduced and incorporated into a second SqS to demonstrate pathway impact. Facilitated group discussions followed each SqS.
Primary and secondary outcome measures Evaluation was conducted through pre-event and postevent questionnaires, field notes and analysis of audiovisual recordings.
Results 38 participants attended a workshop. All participants agreed they were able to contribute to discussions and like the idea of an OG cancer breath test. Five themes emerged related to the proposed new breath test including awareness of OG cancer, barriers to testing and diagnosis, design of new test device, new clinical pathway and placement of test device. 3 themes emerged related to the use of SqS: participatory engagement, simulation and empathetic engagement, and why participants attended.
Conclusions SqS facilitated a shared immersive experience for participants and researchers that led to the coconstruction of knowledge that will guide future research activities and be of value to stakeholders concerned with the invention and adoption of POCT.
- Point-of-Care Testing
- Patient Engagement
- Patient Simulation
- Volatile Organic Compounds
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This article presents the use of sequential simulation (SqS) as a tool for public and patient engagement in new point-of-care diagnostic testing strategies.
SqS allows participants to appreciate the patient journey, including the possible downstream pathway consequences of introducing new diagnostic strategies.
This shared immersion of patients, publics and researchers allows coconstruction of knowledge that will guide future research, evidence generation and policy.
Patient engagement necessitates voluntary participation and convenience sampling was unavoidable.
The test device under evaluation is at a relatively early stage of development and therefore the SqS scenarios were based on assumptions.
Background
Public and patient engagement (PPE) is a fundamental component of healthcare research and actively encouraged by the Department of Health and major funding bodies. PPE refers to the dissemination of information and knowledge between healthcare providers and researchers, members of the public (including patients, carers and people who use health and social care services) and members of organisations representing service users.1 This participation ensures research is applicable to patients, and therefore, increases the likelihood that research findings will translate into clinical practice2 as well as addressing the ethical and political requirements of PPE within healthcare research.3 ,4 Involving patients in the management of their healthcare is widely recognised to improve quality of care, patient safety and health outcomes.5–8 However, PPE can be expensive and, if not rigorously undertaken with appropriate methodologies, there is a risk of reducing it to a mechanistic ‘paper exercise’ that restricts the quality of information generated from the process.4 Ocloo et al9 in their recent narrative review of patient and public involvement (PPI) in healthcare call for ‘models and frameworks that enable power and decision-making to be shared more equitably with patients and the public in designing, planning and co-producing healthcare’.
PPE is particularly important in the implementation of innovation and healthcare delivery improvements.10 Technology advancement such as new diagnostics play an important role in such innovation but development must be in keeping with patient's health needs and expectations.11 ,12 More tests are making the translation from the laboratory to point-of-care test (POCT) devices, creating new diagnostic strategies that may disrupt traditional clinical pathways. It is rare for a patient to directly benefit from a diagnostic test in isolation;13 instead the impact comes from the decisions and interventions that are undertaken as a result of its introduction. Therefore, to allow informed input from public and patients into the research and development of novel diagnostic tests, the test process and any subsequent effects to downstream clinical pathways must be demonstrated.
Sequential simulation (SqS) is a tool that demonstrates key elements in a patient's journey and can highlight the consequences of intervention at each step. SqS workshops can provide an innovative framework for PPE, especially when aligned to the four key assumptions of the Shared Immersion Model as described by Tang et al:14
Public engagement activities can be experiential, involving participation as well as acquisition of information
The shared experience constitutes an event
Being immersed in the shared experience is central, for researchers and publics alike. Critical evaluation of this process is equally valuable for both
Simulation can provide immersive engagements between science and publics, especially with healthcare activity and research
Simulation has previously been used by our group as a tool for engagement with integrated care,15 multidisciplinary teams and adolescents16 and for surgical devices.17 In the first two examples, SqS addressed clinical care pathway redesign; while in the latter, the focus was on the use of novel devices in healthcare environments. The current study combines these two approaches to facilitate PPE in the development of POCT diagnostics by exploring the stakeholder perspective on a new diagnostic test device and investigating its potential impact on the patient's journey.
The aim of this study is to introduce, through a case study, SqS as a methodology for active PPE in the development of novel POCTs and appraise the approach.
Case study
Oesophagogastric (OG) cancer represents the fourth and fifth most common types of cancer death.11 Each year in England, 12 900 people are diagnosed with OG cancer and of these only 37.3% are considered curable at the time of diagnosis.11 ,12 However, when diagnosed at its earliest stage, the 1-year survival is 75–87%.11 Public awareness of these cancer types is poor and the symptoms (dyspepsia (heartburn or indigestion), dysphagia (difficulty swallowing), unexplained weight loss, persistent vomiting, tiredness (anaemia) and upper abdominal pain) are common and often not associated with cancer.10 This leads to a delay in presentation to healthcare services and therefore treatment. In view of this, National Health Service (NHS) England recently undertook a ‘Be Clear on Cancer’ campaign for OG cancer targeting patients with heartburn and indigestion.18 Within our department, research is investigating the use of volatile organic compounds (VOCs) for early OG cancer diagnosis. Previous experimental work has demonstrated that exhaled breath analysis using mass spectrometry can distinguish oesophageal and gastric adenocarcinoma from non-cancer controls,19 demonstrating the potential for a VOC-based breath test to provide point-of-care risk stratification for patients with suspected OG cancer. This new approach aims to provide a readily available, non-invasive and cost-effective test to streamline patients with the early symptoms of cancer to further investigation with endoscopy. It is hoped that by increasing the number of patients diagnosed early, a higher proportion of these patients will have early stage disease and be able to enter a treatment pathway with curative intent. Much remains to be learnt about the social, cultural and practical implications of this new technology.
Methods
Three 3-hour workshops were undertaken in central London. For workshop 1, we invited members of the Oesophageal Patients Association through their mailing list and social media, providing access to participants with prior experience of OG cancer and its diagnostic pathway, either personally or as a relative or carer. Workshops 2 and 3 were aimed at the general public without previous experience of OG cancer. Recruitment to workshop 2 was through an open invitation advertised in venues local to the workshop, and in workshop 3 a focus group recruitment firm (Focus4People, Herts, UK) was used.
The three workshops followed the same structure and comprised presentations, clinical pathway SqS and facilitated group discussions. Following a brief introduction to the day, a presentation covering the background to OG cancer including the current diagnostic strategy was given. This led into the first clinical pathway simulation—a scenario that was designed to represent a relatively common patient journey. It was unscripted and followed a storyboard of a patient, played by a professional actor, noticing the symptoms of an oesophageal cancer and undergoing a typical diagnostic pathway (figure 1). The storyboards were designed to represent a ‘typical’ uncomplicated diagnostic pathway for a patient with oesophageal cancer and created in consultation with specialist clinicians. To validate the storyboard participants with a personal experience of OG cancer, were asked to feedback on how the scenario related to their own experiences during the first workshop. Actors were used to ensure a personalised approach to the scenario, while maintaining confidentiality and ensuring consistency across workshops. Clinicians played their own healthcare roles in the simulation scenarios. The clinicians also respond well to actors who appear very realistic. The sets were created using distributed simulation20—versatile transportable screens and props including beds, desks and medical equipment (figure 2). The simulation scenario was followed by the workshop breaking down into small groups (5–10 people) for facilitated table discussions regarding the current diagnostic pathway. The groups were then brought back together and table discussions were summarised in a plenary session. After a coffee break, a member of the research team gave a presentation describing the current research achievements in lay terms and introduced the concept of the novel breath test, as well as our future ambitions. A second SqS followed the same patient through his journey, although this time we incorporated the breath test into the scenario to demonstrate the potential downstream consequences to the clinical pathway. Again, small table discussions followed.

Storyboard of diagnostic pathway for oesophagogastric cancer used in sequential simulation scenarios. GP, general practitioner; POC, point-of-care.

Sequential simulation (SqS) sets to illustrate (i) the patient's home (ii) an endoscopy unit and (iii) general practice consultation.
Participants completed pre-event (see online supplementary appendix 1) and postevent (see online supplementary appendix 2) questionnaires that included a series of statements regarding attitudes and feedback related to the novel test device and also on the SqS workshop experience itself that participants were asked to rate on a 5-point Likert scale (strongly disagree to strongly agree). Participants were given copies of presentation slides and contact details if they would like to discuss anything from the workshop further.
Supplementary appendix
Supplementary appendix
The workshop discussions were filmed and recorded for subsequent analysis. Workshop recordings were transcribed and emergent thematic analysis undertaken independently by two members of the research team (JRH and SR), who were not directly involved in the test device research. Qualitative data were analysed with NVivo V.10.1.1 software (QSR International, Melbourne, Australia). Ethical approval for the workshops was provided by the Imperial College Joint Research Compliance Office (reference number ICREC_11_5_8) and informed consent was obtained from all workshop participants.
Results
In total, 38 participants attended the 3 workshops, 26 (68%) of whom had no previous experience personally or as a relative or carer of the OG cancer diagnostic pathway. A total of 12 participants were recruited through the Oesophageal Patients Association, of which 11 (92%) attended; 14 participants replied to public poster and email campaign, of which 8 (57%) attended; and 20 patients were recruited by the focus group recruitment company, of which 19 (95%) attended. Two participants have subsequently volunteered to contribute further to our research activities and now have a role in PPI within the group.
Thematic analysis of workshop audio recordings
Two analyses were undertaken: (i) an analysis of participant attitudes towards the use of SqS for PPE in POCT diagnostics; and (ii) an analysis of patient feedback regarding the breath test device, diagnostic strategy and clinical pathway.
Three themes emerged regarding the use of SqS for public engagement in novel POCT diagnostic test: participatory engagement, simulation and empathetic engagement, and why participants attended. Theme summaries and quotations from transcripts are included in table 1.
Summary of themes relating to use of sequential simulation for public engagement in novel diagnostics
In respect to the diagnosis of OG cancer and the proposed new breath test and diagnostic test strategy, five themes emerged from the workshop: awareness of OG cancer, barriers to testing and diagnosis, design of new test device, new clinical pathway and placement of test device. Theme summaries and participant quotations are presented in table 2.
Summary of themes relating to current and novel diagnostic strategy for Oesophago-gastric cancer
Table 3 demonstrates the ‘co-construction of knowledge’ document. This collective output of shared experiences from researchers, patients and public summarises the key outputs raised from the workshops with proposed solutions to guide future research and implementation strategies.
Coconstruction of knowledge from researcher–participant shared experience
Participant feedback questionnaire
All patients completed a questionnaire at the start and on completion of the workshop.
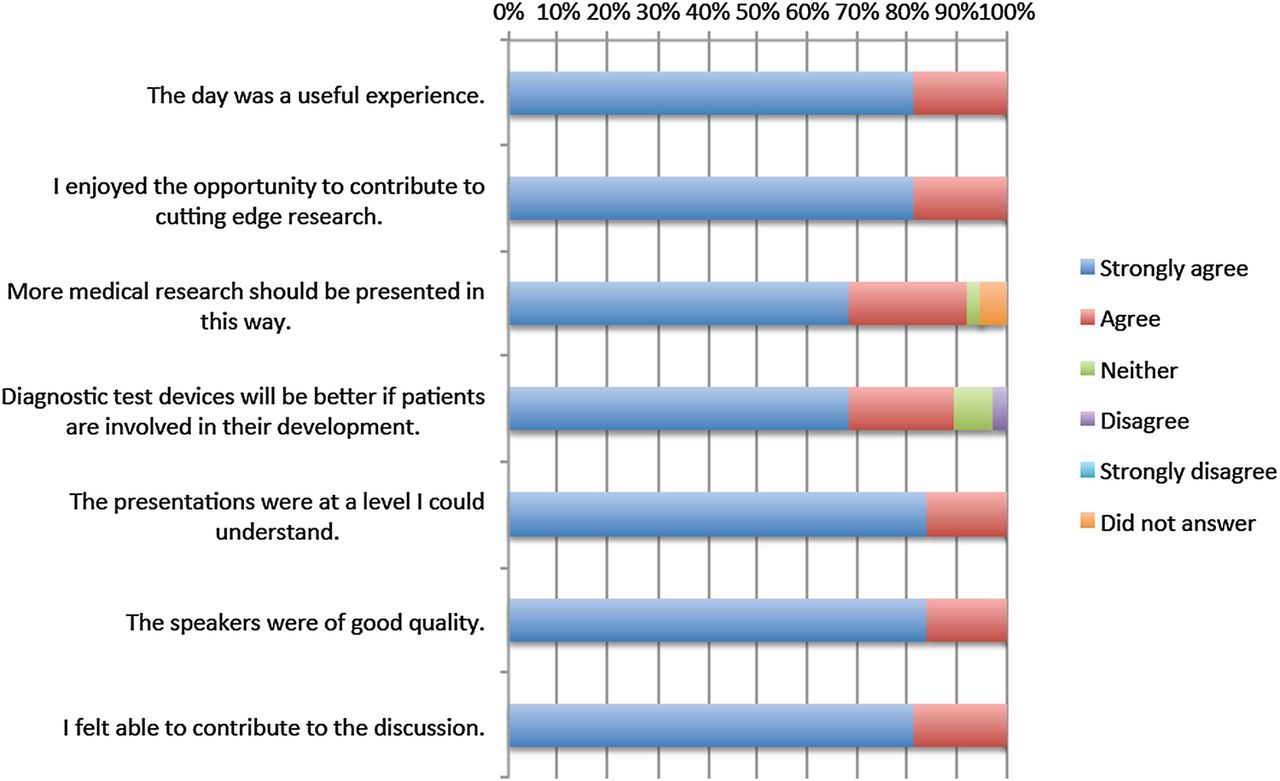
Feedback relating to the SqS workshop experience is shown in figure 3. All patients reported they felt able to contribute to the discussion (strongly agree n=31 (82%); agree n=7 (18%)), that presentations were at a level they were able to understand (strongly agree n=32 (84%); agree n=6 (16%)) and that the day was a useful experience (strongly agree n=31 (82%); n=7 (18%)). The majority of participants felt that diagnostic test devices will be better if patients are involved in their development (strongly agree n=26 (68%); agree n=8 (21%); neither agree or disagree n=3 (8%); disagree n=1 (3%)).

Participant questionnaire feedback relating to the sequential simulation (SqS) workshop experience.
Feedback relating to the breath test strategy is shown in figure 4. All patients liked the idea of a breath test for OG cancer (strongly agree n=32 (84%); agree n=6 (16%)) and stated they would like a breath test before an endoscopy (strongly agree n=36 (95%); agree n=2 (5%)). The majority of patients did not agree that the breath test would add to their anxiety (agree n=2 (5%); neither agree or disagree n=7 (18%); disagree n=10 (26%); strongly disagree n=16 (42%); 3 (8%) did not answer) and agreed that a ‘low-risk’ result from the breath test would provide reassurance without specialist referral (strongly agree n=7 (18%); agree n=19 (50%); neither agree or disagree n=9 (24%); disagree n=3 (8%)).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Participant questionnaire feedback relating to the novel breath testing strategy for the diagnosis of oesophagogastric cancer. GP, general practitioner.
Discussion
SqS workshops provided an effective immersive environment for public and patient engagement around device development and future diagnostic strategy, creating a shared experience that was beneficial to participants and researchers. Rich data provide feedback on research activities to date and will help guide future research activities.
The outputs from the current workshops have already influenced future research plans regarding the VOCs breath test for OG cancer as follows: identifying a broader scope of where the test could be located, including general practice, pharmacies and workplaces; how the test result is presented to manage associated patient anxiety; and the migration from currently used breath bags to sensor technology. The workshops confirmed patient acceptability of the proposed breath testing strategy for cancer diagnosis and reinforced the lack of awareness that exists with regard to OG cancer and its symptoms.21 Furthermore, the workshop outputs have provided valuable information to other stakeholders concerned with POCT invention and adoption, including device designers, clinicians, commissioners and policymakers. As such, we believe results from PPE activities should be routinely published alongside clinical studies and cost-effectiveness arguments as part of a complete evidence package.
The largest challenge in running the workshops was recruitment. Three strategies were trialled, providing an opportunity to weigh the benefits and challenges of each and to recruit different participants with different backgrounds and motivations. The professional focus group recruitment firm was convenient and allowed the tailoring of the group to ensure a representative sample. However, this entailed greater cost as a recruitment commission was paid to the company. Recruitment to workshop 1 was also straightforward as replies to invitations sent to members of the Oesophageal Patients Association were forthcoming. Workshop 2 provided the greatest challenge in recruitment, requiring members of the research group to explore the locality of the workshop venue and placing posters in a variety of venues to encourage interest. Response rate was low, and there was a high rate of non-attendance on the day.
Other costs associated with running the workshops were venue hire including refreshments and lunch, professional actor fees, scenery and props for the simulation scenarios, and transport of equipment. PPI workshops do have an associated cost, for these three events we allocated a budget of £12 000 (although this included the purchase of equipment that can be reused in subsequent events); it is therefore vital that the cost of PPE activities be incorporated into research budgets and funding applications.
This methodology does have limitations. Patient engagement necessitates voluntary participation, and convenience sampling was unavoidable. By varying the recruitment strategy, incentives for attendance and previous knowledge of OG cancer, we hope to have achieved an overall representative sample in the course of the three events, although sociocultural and clinical characteristics of participants were not recorded. Screening participants for their level of engagement using the Patient Health Engagement Scale22 or Patient Activation Measure6 would have provided a useful measure to interpret the comments of participants. The transcripts from the events were analysed by two researchers who were not directly involved with the development of the breath test or VOC research, minimising bias in emergent theme analysis. Finally, the test device under evaluation is at a relatively early stage of development and therefore the scenarios were based on assumptions.
Patient engagement is vital at this early stage to guide device development, ensure the proposed clinical pathway is acceptable to patients and guide future research activities. To be effective, patient engagement must not be seen as an isolated event and needs to continue alongside evidence generation and device development to improve the acceptability of POCT.
The value of PPE is increasingly recognised in the development of medical devices and care pathways. Barello et al,7 in their systematic review of eHealth for Patient Engagement, describe PPE as multidimensional with behavioural, cognitive and emotional components. The review concludes that the majority of approaches to PPE do not facilitate engagement at all three levels. However, SqS is able to provide a holistic and systematic approach that fulfils all three as described in the shared immersion model14 through the participant's role in the experience (emotional), evaluation (cognitive) and participation in the ongoing process of device development (behavioural). Furthermore, the nature of the shared event allows a degree of empathy between all stakeholders present, so that the outputs from the workshops can truly be underpinned in further research and device development.
In conclusion, SqS provides an effective methodology for active public and patient engagement and, to a limited degree, involvement in research towards the development of new POCT diagnostic devices and testing strategies. The outputs of these events provide rich data that can be of use to a wide range of stakeholders and could form a routine part of the evidence base, informing the adoption of new POCT devices.
Acknowledgments
The authors would like to thank Sheraz R Markar, Tom Wiggins, Stefan Antonowicz and Sophie Doran for presenting at the engagement workshops, as well as the Oesophageal Patient's Association for their assistance in recruiting participants for the first workshop.
References
Footnotes
Twitter Follow Jeremy Huddy at @JeremyHuddy
Contributors JRH conceived of the study and participated in its design and coordination, data collection and analysis and drafted the manuscript. S-MW and SR participated in the study design, data collection and analysis, and helped draft the manuscript. TP helped with interpretation of data and drafting the manuscript. GBH conceived of the study, participated in the design and coordination of the study, and helped draft the manuscript. RK conceived of the study, participated in the design of the study and helped draft the manuscript. FB conceived of the study, participated in the design of the study and helped draft the manuscript. All authors read and approved the final manuscript.
Funding This research was supported by the National Institute for Health Research (NIHR) Diagnostic Evidence Co-operative London at Imperial College Healthcare National Health Service (NHS) Trust. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests All authors have completed the International Committee of Medical Journal Editors (ICMJE) uniform disclosure form at http://www.icmje.org/coi_disclosure.pdf and declare: this research was supported and funded by the National Institute for Health Research (NIHR) Diagnostic Evidence Co-operative London at Imperial College Healthcare NHS Trust, JRH is funded by the National Institute for Health Research (NIHR) Diagnostic Evidence Co-operative, S-MW is funded by the Wellcome Trust, Health Education North West London, National Institute of Health Research, RK and FB are founding shareholders and FB is Executive Director (unpaid) of Convincis.
Ethics approval Imperial College Joint Research Compliance Office.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.