Article Text

Abstract
Objectives To determine optimum measurements for abdominal obesity and to assess the prevalence and determinants of metabolic syndrome in Qatar.
Design National health survey.
Setting Qatar National STEPwise Survey conducted by the Supreme Council of Health during 2012.
Participants 2496 Qatari citizens aged 18–64 representative of the general population.
Primary and secondary outcome measures Measure of obesity (body mass index, waist circumference or waist-to-height ratio) that best identified the presence of at least 2 other factors of metabolic syndrome; cut-off values of waist circumference; frequency of metabolic syndrome.
Results Waist circumference ≥102 for men and ≥94 cm for women was the best predictor of the presence of other determinants of metabolic syndrome (raised blood pressure, fasting blood glucose, triglycerides and reduced high-density lipoprotein cholesterol). Using these values, we identified 28% of Qataris with metabolic syndrome, which is considerably lower than the estimate of 37% calculated using the International Diabetes Federation (IDF) criteria. Restricting the analysis to participants without known elevated blood pressure, elevated blood sugar or diabetes 16.5% would be classified as having metabolic syndrome. In a multivariable logistic regression analysis, the prevalence of metabolic syndrome increased steadily with age (OR=3.40 (95% CI 2.02 to 5.74), OR=5.66 (3.65 to 8.78), OR=10.2 (5.98 to 17.6) and OR=18.2 (7.01 to 47.5) for those in the age group ‘30–39’, ‘40–49’, ‘50–59’, ‘60–64’ vs ‘18–29’; p<0.0001), decreased with increasing educational attainment (OR=0.61 (0.39 to 0.96) for those who attained ‘secondary school or more’ compared with ‘less than primary school’; p=0.03) and exercise (OR=0.60 (0.42 to 0.86) for those exercising ≥3000 vs <600 MET-min/week; p=0.006) but was not associated with smoking or diet.
Conclusions Waist circumference was the best measure of obesity to combine with other variables to construct a country-specific definition of metabolic syndrome in Qatar. Approximately 28% of adult Qatari citizens satisfy the criteria for metabolic syndrome, which increased significantly with age. Education and physical activity were inversely associated with this syndrome.
- Metabolic syndrome
- Waist circumference
- National health survey
- Qatar
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to establish optimal cut-off values for waist circumference for Qataris, which is a crucial criterion for a realistic estimation of the prevalence of metabolic syndrome in this population.
The study is based on a WHO STEPS survey, a well-established and tested method specifically for chronic non-communicable diseases (NCD) risk factor surveillance.
As for any population survey, the assumption is made that the sample of individuals interviewed is representative of the whole population.
Introduction
Metabolic syndrome is a combination of individual risk factors that are associated with several serious health conditions such as diabetes, cardiovascular disease or stroke. It is diagnosed by the presence of three or more of five risk factors: abdominal obesity, raised blood pressure (BP), raised fasting blood glucose, raised triglycerides and reduced high-density lipoprotein (HDL) cholesterol. The prevalence of metabolic syndrome is therefore highly dependent on the cut-off points used for the definition of each single component of metabolic syndrome, and particularly for the definition of abdominal obesity. Abdominal obesity is normally measured by waist circumference and broad ethnic-group suboptimal cut-off points have been proposed.1 ,2 Until more specific data are available for Middle East countries, the International Diabetes Federation (IDF) recommended using European cut-off points for all Eastern Mediterranean and Middle East (Arab) populations.1
The aims of this study were: first, to confirm results from a previous study3 showing that waist circumference was an appropriate measure of central obesity for the identification of metabolic syndrome among Qatari citizens; second, to assess optimal cut-off points for waist circumference in Qataris from data in a representative National Health Survey; third, to use these cut-off points to determine the prevalence and fourth, the determinants of metabolic syndrome among Qatari citizens.
Materials and methods
Survey instrument and sampling
Qatar had a total adult population of about 1.5 million inhabitants in 2010 comprising 240 000 Qatari Nationals (39% aged <15, 58% aged 15–64 and 3% aged 65 or more).4
We obtained survey data from a random sample of 2496 adult Qatari citizens aged 18–64 that were collected during the year 2012 by the trained Qatar Supreme Council of Health staff based on the WHO's established method for estimating non-communicable diseases prevalence and risk factors, as part of surveillance.
The same standardised questions and protocols have been used in many WHO member countries for monitoring within-country trends and for making comparisons across countries. General details on the survey are available at the WHO website,5 and country-specific details are available in a report from the Supreme Council of Health, Qatar.6 Briefly, a two-stage sample design was used, selecting primary sampling units (PSUs) at the first stage and a sample of households within each selected PSU at the second stage. A total of 96 PSUs were selected from the Qatari frame of PSUs. In the second stage, 30 households were selected from each selected PSU by simple systematic sampling. Interviewers visited each selected household and identified all survey-eligible individuals. A personal digital assistant device was used to generate a random number to select one individual, either male or female, from within the household. Only these selected individuals were administered the questionnaire at their household. Since biomedical tests require 12 hours of fasting, appointments were given based on the agreement between the interviewers and the respondents and were conducted at the household level on Saturdays. In total 2496 of the 2850 Qatari households selected were interviewed, corresponding to an overall response rate of 88%. An Arabic standardised version of the stepwise data collection form (Questionnaire) was used in the survey, gathering:
Demographic and behavioural risk factors: age, sex, years at school, tobacco and smokeless tobacco use, types of physical activity, sedentary behaviour, fruit and vegetable consumption, history of raised BP, history of diabetes and oral health;
Physical measurements: height and weight, waist circumference, hip circumference, BP;
Blood samples for biochemical measurements: fasting blood glucose, total cholesterol, HDL cholesterol, LDL-cholesterol and triglycerides.
All the Qatar national STEPwise questionnaires were tested for cultural applicability and sensitivity through word and pilot testing of the questionnaires.
This research proposal had been previously reviewed and approved by the Qatar Supreme Council of Health. The Office of Research Integrity at Weill Cornell Medical College in Qatar reviewed the proposal for secondary research analysis of those data by the authors and determined that such secondary analysis was exempt from Qatari and American human subject protection regulations and therefore did not require review by an institutional review board.
Definition of metabolic syndrome and physical activity assessment
Metabolic syndrome was defined according to the IDF criteria.1 It combines several individual risk factors including raised fasting blood glucose (≥100 mg/dL or taking diabetes medication), raised BP (systolic BP≥130 mm Hg or diastolic BP≥85 mm Hg, or taking anti-hypertensive medication), raised triglycerides (≥150 mg/dL), reduced HDL cholesterol (<40 in men or <50 mg/dL in women) and central obesity defined as waist circumference with ethnicity specific values (using Qatar-specific cut-offs estimated from this study: waist circumference ≥102 in men or ≥94 cm in women or body mass index (BMI)≥30 kg/m2). According to the IDF criteria,1 if BMI is >30 kg/m2, central obesity can be assumed and waist circumference does not need to be measured. If three or more of these risk factors are present, then metabolic syndrome is present.1
We calculated the total physical activity using the Global Physical Activity Questionnaire developed by the WHO.7 This instrument collects information on physical activity participation in three settings (activity at work, travel to and from places, recreational activities) and sedentary behaviour. Participants were categorised into low, moderate and high levels of activity based on the sum of their total metabolic equivalent (MET)-minutes of activity computed for each setting (1 MET being defined as 1 kcal/kg/hour and is equivalent to the energy cost of sitting quietly).
Data analysis
Demographic and health characteristics of the Qatari population were evaluated using data from a cross-sectional WHO STEPwise survey conducted in 2012. The STEPS tool was designed to cover three levels of risk factor assessment: step 1—demographic and behavioural risk factors information, step 2—physical measurements in household settings and step 3—biochemical measurements. The data were weighted using population weights to adjust for age and sex differences between the sample and the national population. Percentages, means and corresponding 95% CIs were then calculated using the weighted data. Comparison of percentages across groups of participants was assessed using the Rao-Scott χ2 test, which is a design-adjusted version of the Pearson χ2 test.
We evaluated the prevalence of each single component of metabolic syndrome in men and women by different age groups. We used the receiver operator characteristic (ROC) curve analysis to assess the performance of various measures of obesity (BMI, waist circumference, waist-to-height ratio) for the identification of those with at least two other components of metabolic syndrome and calculated the area under the curve (AUC) (or ‘c-statistic’) to assess the prediction ability of each parameter. Optimal waist circumference cut-off points that maximise total accuracy (sensitivity and specificity) were calculated by the intersection of the plots of sensitivity and specificity separately for men and for women and combined with other measurements to assess the prevalence of metabolic syndrome in Qatar.
Finally, we searched for lifestyle factors associated with metabolic syndrome using logistic regression, adjusting models for potential confounders such as age, gender or educational attainment level. When present, missing data were treated as a separate category and represented by dummy variables, allowing logistic regression models to be fitted on the whole population.
Data analysis was performed using the SURVEYFREQ, SURVEYMEANS, SURVEYREG and SURVEYLOGISTIC procedures of the SAS software (V.9.2, Cary, North Carolina, USA). All tests were two-sided and p values <0.05 considered statistically significant.
Results
The survey sample consisted of 1053 male and 1443 female Qataris. Table 1 contains sociodemographic characteristics of participants according to gender. Significant gender-related differences were observed for educational attainment, with significantly more women (14.6%) than men (5.4%) who had attained less than primary school, for marital status with more women than men being divorced or widowed (6.4% and 3.9%, respectively, for women and 2.2% and 0.2% for men) and for occupation with the majority of men (64.7%) being government employees, while homemakers were the largest group in women (38.8%) (p<0.0001). The age distribution (p=0.21) was similar in men and women.
Sociodemographic characteristics of participants according to gender
Best obesity measure that predicts metabolic syndrome
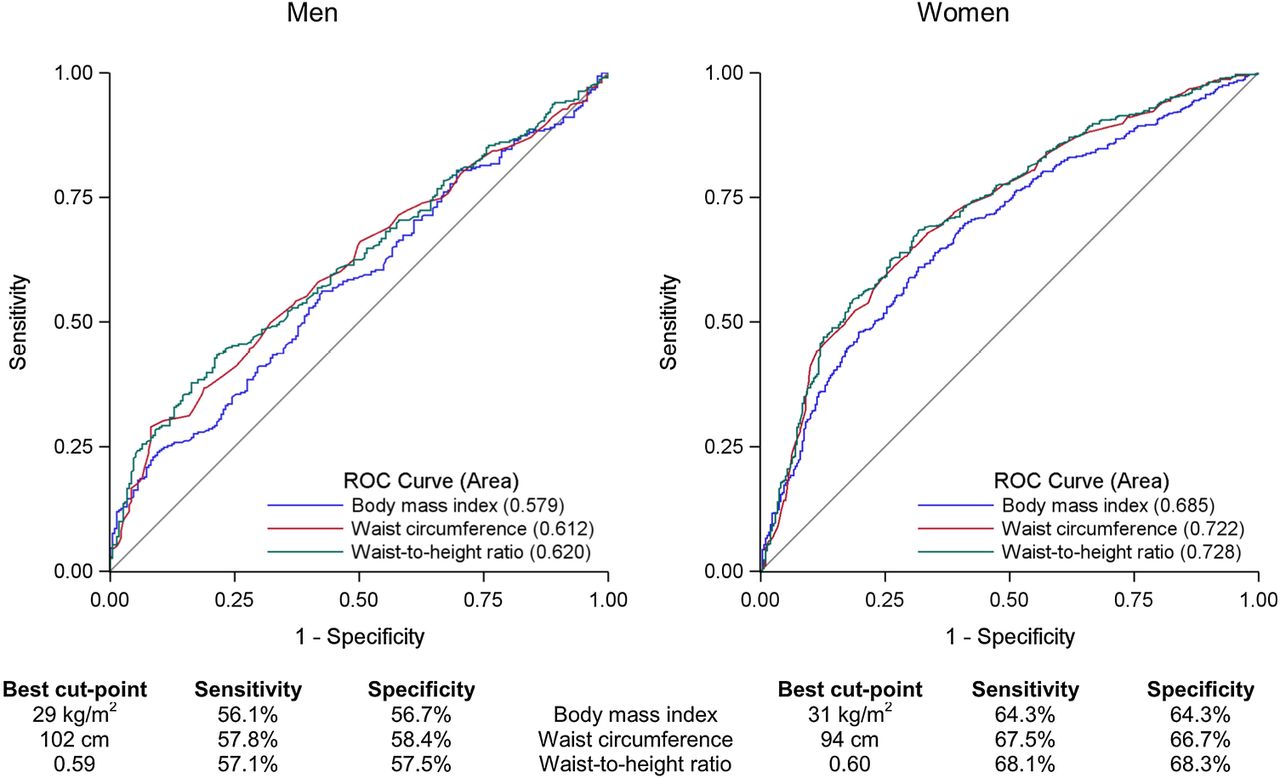
We performed ROC curve analysis to determine which obesity measure (BMI, waist circumference or waist-to-height ratio) and the corresponding cut-off points that best predict metabolic syndrome. For this analysis, we plotted the sensitivity versus 1-specificity for all possible values of the three obesity measures to predict the presence of at least two of the four remaining factors of metabolic syndrome (raised BP, raised fasting blood glucose, raised triglycerides or reduced HDL cholesterol) (figure 1). Waist circumference and waist-to-height ratio were better predictors of metabolic syndrome than BMI in men and women, yielding respective moderate AUC of 0.612, 0.620 and 0.579 in men and 0.722, 0.728 and 0.685 in women. The classifier performance of waist circumference is, however, only poor in men and fair in women.
{kind=link}
Receiver operator characteristic (ROC) curves for body mass index, waist circumference and waist-to-height ratio to predict the presence of at least two factors of metabolic syndrome (excluding abdominal obesity) in men and women in Qatar. Information on body mass index was available for 2384 participants, waist circumference for 2335 participants and waist-to-height ratio for 2333 participants.
We therefore confirmed that waist circumference (criteria used by the IDF), which has similar predictive value of metabolic syndrome than waist-to-height ratio and necessitates a single measurement with no calculation, is an appropriate measure of central obesity. The waist circumference cut-off points that maximised total accuracy (sensitivity and specificity) were 102 for men and 94 cm for women, respectively. The corresponding sensitivity and specificity for the detection of metabolic syndrome were 57.8% and 58.4% in men and 65.7% and 66.7% in women.
Waist circumference distribution
We assessed the waist circumference of Qatari men and women and the proportion of those with measures above cut-off points defined by the IDF in the absence of ethnic-specific values (≥94 for men and ≥80 cm for women), Adult Treatment Panel III (ATP-III) (≥102 for men and ≥88 cm for women) or obtained from the previous ROC curves analysis for Qatari citizens (≥102 for men and ≥94 cm for women) (table 2). Average waist circumference was 100 cm (95% CI 98 to 102) for men and 90 cm (95% CI 88 to 92) for women. Average waist circumference increased steadily with age in both sexes to reach 106 cm (95% CI 101 to 112) and 103 cm (95% CI 98 to 108), respectively, for men and women aged 60–64. Using the cut-off points proposed by the IDF (≥94 for men and ≥80 cm for women, ie, the same as those used for Europeans), 63.4% of men and 68.5% of women would be at risk, with the proportion as high as 77.1% in men and 92.4% in women aged 60 or more. Using the less-stringent ATP-III2 cut-off points (≥102 for men and ≥88 cm for women), the proportion of men and women with a waist circumference indicative of central obesity will diminish to 45.4% and 51.3%, respectively (for all age groups). Using Qatar-specific cut-off points identified by ROC curve analysis (≥102 for men and ≥94 cm for women), only 45.4% of men and 38.7% of women would be considered to have waist measurement indicative of central obesity.
Weighted prevalence of suboptimal waist circumference by sex and age group among Qataris using different cut-off points
Prevalence of metabolic syndrome
The prevalence of metabolic syndrome and its components is presented in table 3, stratified by gender and age group. This information was collected at different steps of the survey and was available for a variable number of participants (1470 for fasting blood glucose, 2342 for BP, 1518 for triglycerides level, 1526 for HDL cholesterol and 2356 for abdominal obesity). As a result, information on metabolic syndrome was available for 1373 (55%) participants.
Weighted prevalence of metabolic syndrome and its components by sex and age group among Qataris
Considering all age groups together, reduced HDL cholesterol (51.9%) and abdominal obesity (50.7%) were the most common single components of metabolic syndrome in men, while abdominal obesity (50.5%) and raised BP (43.3%) were the most common single components of metabolic syndrome in women.
Overall, the prevalence of metabolic syndrome in Qatar based on country-specific estimates of waist circumference was 27.7% (95% CI 24.5% to 30.9%) for both sexes combined, 28.7% (95% CI 23.6% to 33.7%) in men and 26.8% (95% CI 23.1% to 30.4%) in women. This prevalence increases with age from 9.3% (95% CI 6.0% to 12.7%) in those under the age of 30 to 70.2% (95% CI 54.1% to 86.3%) in those aged 60–64.
Determinants of metabolic syndrome
We used multivariable logistic regression to identify sociodemographic or lifestyle factors associated with metabolic syndrome (table 4). After adjustment for age and educational attainment level, gender was not associated with the risk of metabolic syndrome. The risk of metabolic syndrome, however, significantly increased with increasing age with OR=3.40 (95% CI 2.02 to 5.74); OR=5.66 (95% CI 3.65 to 8.78); OR=10.2 (95% CI 5.98 to 17.6) and OR=18.2 (95% CI 7.01 to 47.5) for those in the age group ‘30–39’, ‘40–49’, ‘50–59’, ‘60–64’ compared with those in the ‘18–29’ age group (p<0.0001), but decreased with increasing educational attainment with OR=0.61 (95% CI 0.39 to 0.96) for those who attained ‘secondary school or more’ compared with ‘less than primary school’ (p=0.03). No statistical significant association was observed for marital status or occupation. The particularly low but not statistically significant risk for students may be in part due to residual confounding from age, marital status and physical activity.
Characteristics associated with metabolic syndrome at multivariable analysis
Neither tobacco smoking nor any single component of the diet recorded at the survey (see online supplementary table) was associated with metabolic syndrome. After adjustment for age, gender and educational attainment, the risk of metabolic syndrome was reduced by 40% for those with high physical activity levels (at least 3000 MET-min/week) compared with those with low physical activity level (<600 MET-min/week) (OR=0.60; 95% CI 0.42 to 0.86) (p=0.006).
Supplementary table
Metabolic syndrome among ‘healthy’ individuals
The survey was conducted to be representative of the general population and therefore included a proportion of participants with previous diagnosis of diabetes or hypertension. Overall, 70% of the participants with available information about metabolic syndrome had never been previously told by a doctor or other health worker that they had either hypertension or diabetes. We reassessed the prevalence of metabolic syndrome and its components among these presumed ‘healthy participants’ (table 5). In this subset, the survey eventually found that 13.7% (95% CI 10.1% to 17.2%) had elevated fasting blood glucose, and 31.6% (95% CI 28.8% to 34.4%) had raised BP; metabolic syndrome was present in 16.5% (95% CI 13.5% to 19.5%).
Weighted prevalence of metabolic syndrome and its components by sex and age group among 1785 Qataris who reported not having been told by a doctor or other health worker that they had raised BP (or hypertension) or raised blood sugar (or diabetes)
Discussion
Health professionals depend on estimates of the frequency of metabolic syndrome to plan effective strategies for controlling several serious conditions within a given population. Thus, it is extremely important that the estimated prevalence of metabolic syndrome be reliable and based on information that is appropriate for the selected region or country.
The major organisations concerned with defining metabolic syndrome recognise that central adiposity—an important component of this syndrome—is most easily measured by waist circumference.1 ,2 Furthermore, the IDF has emphasised the need for determining country-specific estimates of cut-off points for waist circumference in calculating the prevalence of metabolic syndrome. In fact, there is good evidence that body composition varies among ethnic groups, Asians having lower cut-off points than Europeans, and African-Americans and Hispanics having similar cut-off points to Europeans. Differences between populations could relate to genetic differences that may affect body composition, environmental exposure and particularly nutritional differences such as early childhood nutrition exposures.8 A number of region-specific or population-specific estimates have been published, but there are only a few for Middle East countries and none for Qatar (table 6).
Ethnic specific values for waist circumference from selected Middle East countries
In previous publications, Bener et al3 ,9 suggested that previous criteria for estimating the risk of metabolic syndrome as recommended by the WHO, the IDF and ATP-III might be inappropriate for Qatar. In particular, he and his coauthors proposed BMI, waist-to-hip and waist-to-height ratio in alternative to waist circumference as a measure of central obesity.3 We used data from the 2012 Qatar National STEPwise Survey to calculate the current prevalence of metabolic syndrome in Qatar. We confirmed that waist circumference was an appropriate parameter for identifying other individual components of metabolic syndrome. For the entire Qatari adult population, using the best cut-off points for waist circumference, we estimate the prevalence of metabolic syndrome in adults to be 28%. This value resembles the previous overall estimate of 26% for this country obtained using the ATP-III criteria but considerably lower than the estimate of 37% derived from using the IDF criteria.9 For comparison, estimates of the age-standardised prevalence of metabolic syndrome in the USA are 23%.10
In a multivariable analysis, the risk of metabolic syndrome increased steadily with age: participants aged 60–64 were 18 times more likely to suffer from metabolic syndrome than those who were in the 18–30 age group. The frequency of metabolic syndrome was 39% lower among participants with the highest level of educational attainment than in the group with the least amount of education. Exercise of at least 3000 MET-min/week lowered the risk of metabolic syndrome by 40% compared with persons in the lowest exercise group. Neither diet nor smoking had any impact on the occurrence of metabolic syndrome in this survey. This could be due to the fact that only basic information was collected on diet and because smoking prevalence is relatively low in Qatar. This analysis, however, suggests that among the various lifestyle factors that might alter the prevalence of metabolic syndrome in Qatar, exercise is the most important and deserves emphasis in any disease prevention programme.
Of interest, about 70% of participants in the sample survey were unaware of pre-existing diabetes or hypertension. After evaluation, 16.5% in this group were eventually diagnosed with metabolic syndrome.
The availability of specific waist circumference cut-off points for Qataris will also allow a better identification of the metabolic syndrome at the individual level in this population. Using lower cut-off points for Europeans, which are recommended in the absence of ethnicity specific data, would markedly increase the number of individuals classified at risk of Mets.
The strength of this study is that the data came from a carefully selected random population sample and data collection followed well-defined WHO criteria. As in other surveys, there was a different response rate for each step, especially for the collection of biological material. Fifty-five per cent of participants in the Qatar National STEPwise Survey provided a blood sample, which is still a fair response rate. Many individuals who live in this region refuse to provide blood samples for a variety of cultural reasons in survey situations such as this one, but we have no reason to believe that the blood sugar values of study participants who provided blood samples are different from the values of those who did not. However, this might introduce an unknown bias into the estimate of the prevalence of metabolic syndrome. We also recognised that treating missing data as a category in the regression models, as any other method to handle missing data, such as dropping subjects or imputation, could again have introduced some bias.
Another study limitation pertains to the accuracy of self-reported dietary information. This information is an estimate, which may not be a true measure of past or present food consumption. This could lead to inappropriate conclusions that the diet has no significant impact on prevention of metabolic syndrome. Finally, as for any population survey, the assumption was made that the sample of individuals interviewed is representative of the whole population. Our careful sampling framework should guarantee this assumption.
In summary, using new ethnic-specific cut-off points (≥102 for men and ≥94 cm for women) derived from the ROC curve analysis of abdominal waist circumference, the prevalence of metabolic syndrome in adult Qataris is 28%. We believe the new cut-off points for waist measurement from this country could be suitable for estimating the prevalence of metabolic syndrome in similar populations from other Middle East countries where country-specific data for waist measurements are unavailable.
Acknowledgments
The authors would like to acknowledge the Supreme Council of Health staff for data collection.
References
Footnotes
Contributors All the authors have made substantive intellectual contributions to this study: MHA-T, AAMA-T, SC, JS, RM, ABL and PM designed the study. WFA-C, BAA, SAHK and AOHB conducted the study and collected the data. PM analysed the data. PM and ABL drafted the manuscript. RM, SC, JS and AAMA-T edited the manuscript. All the authors reviewed the manuscript and approved the final version.
Funding This work was funded by both the Supreme Council of Health and Qatar Foundation through the Weill Cornell Medical College in Qatar Biomedical Research Program.
Competing interests None declared.
Ethics approval Qatar Supreme Council of Health.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are from the Qatar National STEPwise Survey whose authors may be contacted at the Supreme Council of Health, Qatar (AAMA-T; Manager Health Promotion and Noncommunicable Diseases, email: aalthani@sch.gov.qa).