Article Text

Abstract
Objectives Diabetes requires continuous medical care including prevention of acute complications and risk reduction for long-term complications. Diabetic complications impose a substantial burden on public health and care delivery. We examined trends in regional differences in hospitalisations due to diabetes-related complications among the total diabetes population in Finland.
Research design A longitudinal register-based cohort study 1996−2011 among a total population with diabetes in Finland.
Participants All persons with diabetes identified from several administrative registers in Finland in 1964−2011 and alive on 1 January 1996.
Outcome measures We examined hospitalisations due to diabetes-related short-term and long-term complications, uncomplicated diabetes, myocardial infarction, stroke, lower extremity amputation and end-stage renal disease (ESRD). We calculated annual age-adjusted rates per 10 000 person years and the systematic component of variation. Multilevel models were used for studying time trends in regional variation.
Results There was a steep decline in complication-related hospitalisation rates during the study period. The decline was relatively small in ESRD (30%), whereas rates of hospitalisations for short-term and long-term complications as well as uncomplicated diabetes diminished by about 80%. The overall correlation between hospital district intercepts and slopes in time was −0.72 (p<0.001) among men and −0.99 (p<0.001) among women indicating diminishing variation. Diminishing variation was found in each of the complications studied. The variation was mainly distributed at the health centre level.
Conclusions Our study suggests that the prevention of complications among persons with diabetes has improved in Finland between 1996 and 2011. The results further suggest that the prevention of complications has become more uniform throughout the country.
- PRIMARY CARE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Our register-based data cover the total population with diabetes identified from different register sources in Finland over a 16-year follow-up.
We used two indicators of region of residence that are directly connected to the organisation of public healthcare for the residents, enabling us to disentangle the association of each organisational level with regional variations in complication rates.
Multilevel models enabled us to capture the hierarchical nature of the data (health centres nested in hospital districts), allowing us to analyse the association more efficiently.
Those with undiagnosed diabetes and diabetes treated only with diet are missing from our data.
Since we used hospitalisation data to study complications of diabetes, we cannot be sure to what extent our findings represent a true decrease in the number of complications or a partial shift of treatment to ambulatory care.
Introduction
The diabetic population is growing worldwide. An epidemic expansion of type 2 diabetes has been considered to be the main contributor to the increase in European countries including Finland.1 ,2 There has been a major increase in type 1 diabetes as well in Finland.2 ,3 As a complex chronic disease, diabetes requires continuous medical care including multifactorial risk reduction, supporting patient self-management, prevention of acute complications and reduction of the risk of long-term complications.4 The incidence of macrovascular complications (myocardial infarction (MI) and stroke) in the diabetic population is decreasing according to several studies.5 ,6 In microvascular complications like end-stage renal disease (ESRD), a decrease has also been reported in many countries among persons with diabetes.7 ,8 A similar decrease has been reported in lower extremity amputations (LEA) in many countries.9–11 However, the complications still generate a substantial burden on public health and the healthcare system.12
Hospitalisations due to ambulatory care sensitive conditions, that is, hospitalisations that could be prevented by timely and effective primary care interventions, have under recent years been increasingly used to evaluate access to and quality of primary care.13 ,14 Studies have used slightly different lists of conditions, but have usually examined three types of conditions: conditions that can be prevented by vaccination, acute conditions in which hospitalisation can be prevented by acute management and chronic conditions where primary care can prevent later admissions. The research evidence comes mainly from the USA,14–17 but some studies have focused on countries similar to Finland in terms of the healthcare system, such as Canada14 and the UK.18 There are also a few studies that have examined the quality of care among persons with diabetes by using the avoidable hospitalisations method. These studies have reported hospitalisations due to complications of diabetes from Taiwan among the adult population,19 from the USA among veterans20 and elderly Medicare recipients,21 ,22 from Canada among persons with intellectual and developmental disabilities,23 and among the First Nations population.24 However, these studies have mainly been based on survey or regional samples, or specific population groups and have typically had relatively short follow-up periods. The Organisation for Economic Cooperation and Development (OECD) currently evaluates the quality of diabetes care using four indicators based on hospital inpatient data, namely hospitalisations with uncomplicated diabetes, short-term and long-term complications of diabetes and LEA among persons with diabetes.25 We know of one earlier study examining time trends in regional differences in short-term complications of diabetes using register data.6 The Finnish context provides an excellent case for analysing avoidable hospitalisations, since the public healthcare system guarantees universal access to care to all residents according to need irrespective of region of residence or socioeconomic status. The system is mainly based on tax revenues and user fees are, in general, low.26
The aim of this register-based study was to examine hospitalisations due to diabetes-related complications among the total diabetes population in Finland from 1996 to 2011. We examined trends in diabetes-related short-term and long-term complications, uncomplicated diabetes and macrovascular and microvascular complications including MI, stroke, LEA and ESRD for men and women separately and with regional differences in them.
Methods
Population with diabetes
The Diabetes in Finland database was collected in a collaborative project by the National Institute for Health and Welfare (THL), the Social Insurance Institution (Kela) and the Finnish Diabetes Association. It covers all persons with diabetes identified from different register sources in Finland during 1964−2011 including the Hospital Discharge and Birth registers (THL), Causes of Death Register (Statistics Finland), Finnish Kidney Register and drug reimbursement registers (Kela). For these persons, data regarding the use of hospital services, both public and private (THL), and causes of death (Statistics Finland) between 1996 and 2011 were individually linked using the personal identification code unique to each individual. In the data, altogether 176 392 persons with diabetes contributed to 169 765 person years in 1996. In 2010, the numbers had increased and 385 281 persons contributed to 375 895 person years. We examined hospitalisations among persons alive with diabetes in the beginning of 1996 and followed them up until 31 December 2011 or earlier death. Persons with gestational diabetes only were excluded from the data. The linkages were performed by competent authorities and the research group received anonymised data.
Measurement
We examined hospitalisations due to diabetes complications using the diagnosis groups used by OECD in assessing quality of care including hospital admissions due to short-term complications (hypoglycaemic and hyperglycaemic coma), long-term complications (renal, ocular, neurological, microvascular and other complications) and uncomplicated diabetes as the main diagnosis, and LEA excluding cases associated with trauma.25 We further examined hospitalisations due to acute MI and stroke as the main diagnosis as well as the incidence of ESRD with onset of renal replacement therapy as registered in the Finnish Kidney Register as an indicator. Since we wanted to analyse hospital admissions due to complications among persons with diabetes, hospitalisations needed to occur after the diagnosis of diabetes or within 365 days preceding diabetes diagnosis due to a time lag between the diagnosis and registration of it in the drug reimbursement register. We considered hospital admissions due to the same complication with admission dates within 1 day of the discharge day of the preceding admission as a single admission. There were altogether 13 097 cases of hospitalisations due to any of these diabetes-related complications among men in 1996 and the numbers decreased steadily; in 2011, the number was 9861. Among women, the numbers were 14 596 and 7401, respectively.
We used two indicators of region of residence: first, health centre area (single municipality or cooperation area of municipalities) that is responsible for organising primary healthcare for the residents; and second, hospital district (owned by the federations of municipalities), which in Finland is responsible for organising the public specialist services for the residents. Publicly funded hospitals produce ca 95% of all specialised inpatient services in Finland.26 The municipality of residence was obtained from the Hospital Discharge Register for each individual at the time of hospital admission. Owing to the data protection regulations, patient data from municipalities with a population smaller than 5000 persons were merged with data from neighbouring municipalities with which they cooperated in some way in organising healthcare, for example, emergency services. The small hospital district of Åland was excluded from the analyses due to small numbers. Other variables included in the analyses were year, gender and age in 5-year age brackets.
Statistical methods
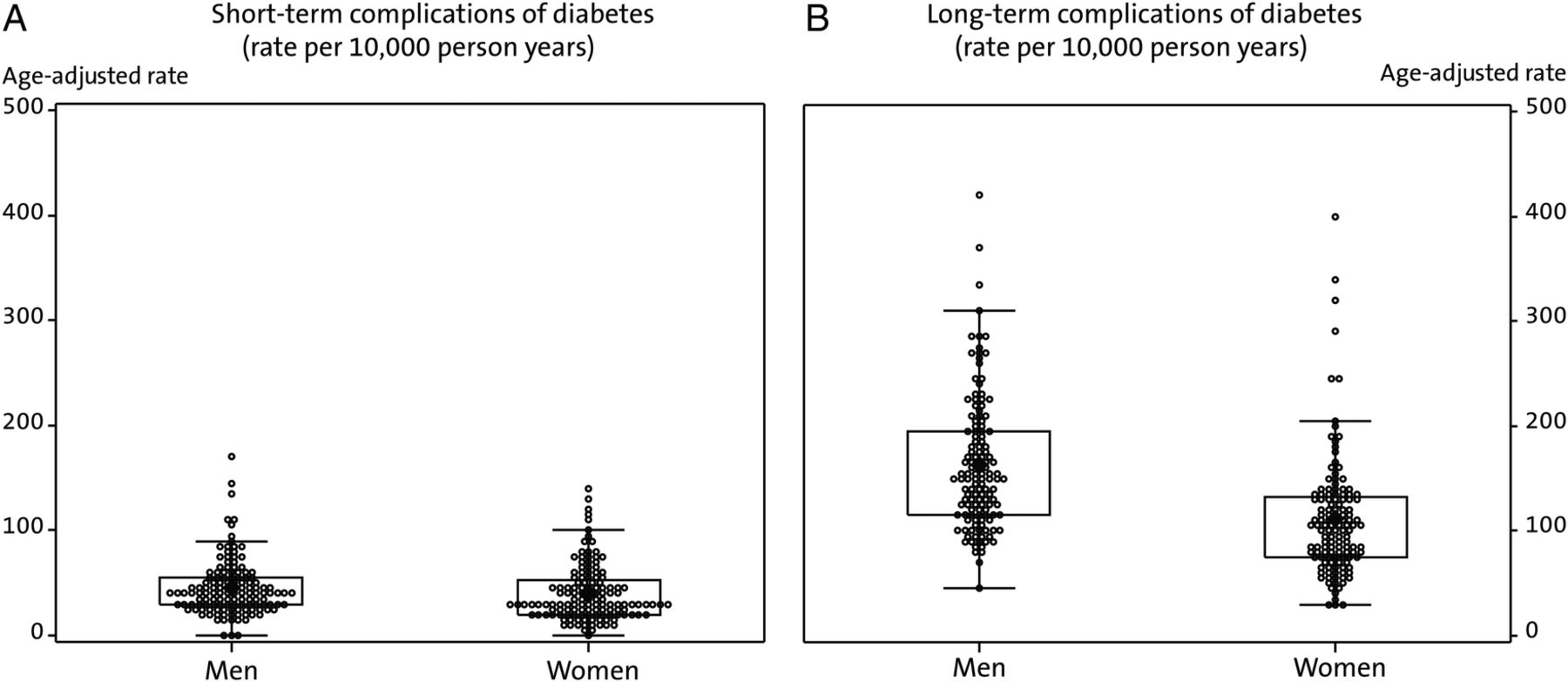
We calculated rates for avoidable hospitalisations per 10 000 person years adjusting for age using the direct method, and the total diabetes population of 2011 as the standard population. We further calculated the systematic component of variation (SCV) between hospital districts as a descriptive measure of annual variation in hospitalisation rates. It relates the number of observed hospitalisations to those expected in each hospital district, given the population structure in terms of year and age. It is a relative measure that indicates whether the variation is larger than could be expected by chance. Likewise, SCVs were calculated between the health centre areas. We illustrate the variation in regional dispersion of complications with the two scatter plots presenting age-adjusted hospitalisation rates among persons with diabetes per 10 000 person years by health centre with each dot representing hospitalisation rate at a single health centre area among men and women between 2007 and 2011.
Our data also allowed us to examine possible convergence of hospitalisation rates at the hospital district level. First, we calculated autocorrelations in each of the complications and hospital districts to study consistency in hospitalisation rates and their suitability for further analysis. Next, we performed two-level models for annual z-scores of the age-standardised hospitalisation rates in each hospital district and complications adjusted for polynomial function of time with normally distributed random intercept and slope terms at the hospital district level. Z-scores were used for hospitalisation rates to study the rates from different complications in a comparable scale. Multilevel models were applied to capture the hierarchical nature of the data and polynomial function of time to capture the general national trend in each complication. In these models, we examined the correlation between the random intercept and slope terms as an estimate of possible convergence in hospitalisation rates. A statistically significant negative correlation was interpreted as a decrease of regional variation with higher than average random intercepts linked with a larger than average decrease in random slopes and vice versa. A similar model was fitted to hospitalisation rates for all complications simultaneously where polynomial function of time was adjusted for each complication in order to calculate an estimate for possible general convergence of hospitalisation rates in diabetic complications.27 ,28 In a separate analysis, we examined whether variation between hospitalisation rates was mainly in the hospital district or health centre level using three-level Poisson regression models. In these models, year was controlled as a continuous variable and age group as a categorical variable with hospital districts and health centres nested within hospital districts as random variables. In order to assess possible changes in the levels of regional variation, we estimated models separately for the years 1996−2000 and 2007−2011. The likelihood ratio test was used to assess the statistical significance of random components in the models. In all the analyses, separate models were calculated for men and women and for each of the complications.
Results
Among both men and women, hospitalisation rates were largest for uncomplicated diabetes and long-term complications of diabetes (figure 1). The LEA rates, and especially ESRD rates, were relatively low. The rates among persons with diabetes (per 10 000 person years) for LEA were 82 among men and 41 among women in 1996, and for ESRD 11 among men and 6 among women in 1996. Hospitalisations due to the diabetes-related complications, both long-term and short-term, and uncomplicated diabetes decreased by ca 80% during the study period. Hospitalisations due to LEA, MI and stroke decreased by ca 50%, and hospitalisations due to ESRD decreased by ca 30% during the study period among both genders.

Age-adjusted rates of hospitalisations due to complications of diabetes (per 10 000 person years) among men and women with diabetes in 1996–2011 in Finland.
Table 1 shows per complication the hospitalisation rates for five complications in 1996, 2004 and 2011 and the SCV between hospital districts and between health centre areas. The SCV between hospital districts was, in general, small, and larger in hospitalisations due to short-term complications of diabetes, especially among women (0.06–0.13), while among men the variation was 0.02–0.06. In relative terms, the SCV diminished only in MI among women and in stroke among men, which would suggest that the hospital district rates for most of the complications would not converge.
Hospitalisation rate (per 10 000 person years in population at risk), and systematic component of variation between hospital districts (SCVHD) and health centre areas (SCVHC) in diabetes-related complications in 1996, 2004 and 2011 in Finland
The SCVs were, in general, much larger when examining health centre areas compared with hospital districts. The SCV was especially large in short-term complications of diabetes both among men (0.43–0.45) and among women (0.42–0.45), and it remained relatively stable throughout the study period. The SCV only diminished in stroke among both genders and in MI among men, suggesting that health centre area rates would not converge either.
We then inspected whether hospital districts were consistently above or below the national trend in each of the complications. Since the autocorrelations in hospitalisation rates due to LEA and ESRD were relatively small and, probably due to small numbers, varied between hospital districts suggesting non-consistency in time, they were excluded from further analyses. The rest of the hospital district autocorrelations averaged over the conditions varied between 0.24 and 0.71 with an average of 0.43 among men, and between 0.38 and 0.70 with an average of 0.54 among women. These results suggest that the regional patterns of hospitalisations were rather consistent in time. The average autocorrelation per condition varied between 0.30 (MI) and 0.63 (uncomplicated diabetes) among men and between 0.33 (stroke) and 0.72 (uncomplicated diabetes) among women.
In multilevel analysis, the overall correlation (including all complications) between hospital district intercepts and slopes in time was −0.72 (p=0.0003) among men and −0.99 (p<0.0001) among women, indicating that the overall hospital district variation in hospitalisations due to these five categories of complications diminished, suggesting convergence. When analysing each complication separately (table 2), the decline was significant in all the other groups (p<0.0001); it was only in the hospitalisations due to short-term complications of diabetes that the decline in hospital district variation was not statistically significant (p=0.397) among men. All the correlations were negative, strongly suggesting decreasing hospital district variation during the study period.
Multilevel model-based correlation between hospital district intercepts and slopes in time between 1996 and 2011
Figure 2 presents the health centre area distribution of hospitalisations due to short-term and long-term complications of diabetes in 2007−2011 as examples of large and small regional variation in complications. Each dot represents a health centre area. In the figure for short-term complications, most of the health centres are close to the mean among both men and women and there are few outliers. In hospitalisations due to long-term complications of diabetes, the variation was much larger, especially among men, and only some of the health centres were close to the mean. Additionally, the area covering 75% of the observations was larger among men compared with women.

{kind=link}
{kind=link}
Health centre area distribution of hospitalisations due to short-term and long-term complications of diabetes among men and women with diabetes in 2007–2011 in Finland, age-adjusted rates per 10 000 person years.
Finally, we examined on which regional level (health centre level vs hospital district level) the variation was mainly distributed in each of the five complications at the beginning (1996−2000) and end (2007−2011) of the study period. We examined these two periods due to the magnitude of change in complication rates during the study period (table 3). At the beginning of the study period, variance in all complications except MI among both men and women was predominantly distributed at the health centre level, suggesting relatively large differences between health centres in hospitalisation rates. However, hospital district-level variance was also statistically significant in all complications except short-term complications among men and stroke among women.
The distribution of variance in hospitalisations due to five diabetes-related complications to health centre (HC) and hospital district (HD) level in Finland in 1996–2000 and 2007–2011 (Poisson multilevel models controlling for year as continuous variable and age as categorical variable)
In MI, the variance was equally distributed among both regional levels, both of which were also statistically significant. In 2007–2011, while the variance estimates appeared to be somewhat lower compared with the beginning of the study period, the variance was still predominantly distributed at the health centre level except for MI among both genders.
Discussion
Overview of the main results
This study examined trends in the incidence of hospitalisations due to diabetes-related complications and regional differences in them from 1996 to 2011. In general, there was a steep decline in the incidence of hospitalisations due to diabetes-related complications among persons with diabetes during the study period. The decline was relatively small in ESRD. Instead, the rates of hospitalisations for short-term and long-term complications of diabetes as well as uncomplicated diabetes declined by about 80%. These results are in line with earlier evidence concerning specific complications from Finland9 and elsewhere.5 ,11 Several factors can explain the major change. Hypoglycaemia is treated more and more often in ambulatory care,29 whereas cardiovascular risk factors are treated more actively,30 and threatening symptoms are investigated and treated earlier before major complications appear.
We further found regional variation in each of the complications studied. These variations diminished during the study period. Earlier studies from other countries have also reported regional differences in complications of diabetes31 and diminishing of differences in time.6 Several potential reasons for the regional variation corresponding with the results of the current study have been suggested in earlier studies, including regional differences in the disease prevalence, sociodemographic characteristics of the patient population and access to and quality of primary care.6 ,32–34 Our data did not contain information about the socioeconomic position of the population with diabetes. Further studies are needed to examine the sociodemographic characteristics of the population with diabetes in order to find out whether these contribute to the differences.
Finally, we found that in most complications, the main part of the variance came from the health centre level. This suggests variation between health centres in the primary care of persons with diabetes and in prevention of complications. Some health centres had a shortage of general practitioners during the study period, which may have resulted in less active treatment of diabetes. As in all quality challenges, the attitudes of physicians and nurses also play a role when deciding how aggressive the treatment of risk factors is. While the variance between health centres appeared to decline during the study period, there were still differences between health centres at the end of the study period. The fact that there is no regular reporting system telling the health centre personnel how they are accomplishing in the risk reduction of diabetes complications, may have contributed to the large variation found in our study. Thus, a regular reporting system might influence the activity of risk reduction.
During the study period, Finland launched a national development programme for the prevention and care of diabetes (DEHKO 2000–2010) aiming to prevent type 2 diabetes and to improve the quality of diabetes care. It also focused on prevention of complications of diabetes. While the programme was national, part of the activities were launched at the hospital district level. Our study cannot directly examine whether the decline in complication prevalence was due to the prevention programme, but the results suggest that the development is in line with the goals of the programme, although in our study the decrease in hospitalisation rates started before the launch of the programme and was relatively stable during the whole study period, as suggested by the relatively high hospital district autocorrelations found in our study.
Methodological considerations
Our data and indicators of complications were based on several large administrative registers which have, in general, been estimated to have good-to-excellent validity.35 ,36 When interpreting the results, it needs to be taken into account that some of the indicators used in the study overlap. For example, long-term complications of diabetes include microvascular complications which overlap with amputations and ESRD. Since we used hospitalisation data, that is, complications observed in specialised care, we cannot be sure whether our findings represent a true decrease in the number of complications or part of their treatment just shifting outside hospitals during the study period. For example, milder complications are treated further in primary care, and short-term complications by first-aid personnel, decreasing the need for hospitalisations. A strength of the study is that we could examine preventable complications among the total diabetes population of the country during a 16-year period. However, those with diabetes treated only with diet (and not hospitalised or died during the study period), and undiagnosed cases are missing from the data. We examined persons with type 1 and type 2 diabetes together, since type 1 consists only of 10–15% of the total population with diabetes in Finland and could not be analysed separately due to small numbers. Additionally, diabetes type cannot unambiguously be defined using register data only. Since the focus of our study was diabetes-related avoidable hospitalisations and regional variations in them, we did not take into account factors related to disease history or the existence of multiple complications among persons with diabetes. The rate for multiple admissions was 851/10 000 person years among men in 1996 and 192/10 000 person years in 2011. Among women, the numbers were 632 and 115. Among both genders, approximately half of these were due to the same reason and half due to different reasons.
The Finnish diabetes population increased rapidly during the study period. This is likely to be partly due to an increase in overweight and sedentary lifestyle. Simultaneously, early detection and treatment of diabetes is likely to have improved, leading to a larger part of diabetes being diagnosed and at a milder stage towards the end of the study period. Further, survival rates have increased in many of the complications. To examine whether the decrease in the incidence of hospitalisations due to diabetes-related complications is mainly due to the increase in population with diabetes, we performed a sensitivity analysis examining national trends in the complications studied in the total Finnish population. These hospitalisation rates also showed a clear downward trend among the total population, but the trend was less steep compared with that within the diabetes population. For example, the decrease was ca 25% among both genders in stroke (vs 50% among the population with diabetes) and 10% among men (vs 50%) and 29% (vs 50%) among women in MI among the population during the study period. This suggests that part of the decrease has to do with the growing and ageing of the population with diabetes in addition to improvements in complication prevention.
Conclusions
Our study suggests that the prevention of complications among persons with diabetes has improved in Finland between 1996 and 2011. Our results concerning larger variation in the health centre area suggest that regional differences exist especially in primary care, which is mainly responsible for management of diabetes and prevention of complications in Finland. Both the convergence of hospital district variation and the apparent diminishing of health centre level variation suggest that the prevention of complications has become more uniform throughout the country.
Acknowledgments
The authors would like to thank the Finnish Diabetes Association and the Social Insurance Institution for collaboration in the forming of the data set.
References
Footnotes
Contributors KM contributed to the conception and design of the study, planning of analyses and drafted the manuscript. MA contributed to the conception and design of the study, performed the statistical analyses and took part in the revision of the manuscript for important intellectual content. SL contributed to the conception and design of the study, planning of analyses, drafting of the manuscript and took part in the revision of the manuscript for important intellectual content. KW and ML contributed to the conception of the study and interpretation of the results and took part in the revision of the manuscript for important intellectual content. IK contributed to the conception and design of the study, planning of analyses and took part in the revision of the manuscript for important intellectual content. All authors have read and approved the final manuscript.
Funding This work was supported by the Academy of Finland (project numbers 277 939 and 254 121).
Competing interests None declared.
Ethics approval Research Ethics Committee of the National Institute for Health and Welfare.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.