Article Text

Abstract
Objectives To identify factors predicting use, adherence and attrition with a nurse-moderated web-based group intervention designed to support mothers of infants aged 0–6 months.
Design 9-Month observational study.
Setting Community maternal and child health service.
Participants 240 mothers attending initial postnatal health checks at community clinics who were randomly assigned to the intervention arm of a pragmatic preference randomised trial (total randomised controlled trial, n=819; response rate=45%).
Intervention In the first week (phase I), mothers were assisted with their first website login by a research assistant. In weeks 2–7 (phase II), mothers participated in the web-based intervention with an expectation of weekly logins. The web-based intervention was comparable to traditional face-to-face new mothers’ groups. During weeks 8–26 (phase III), mothers participated in an extended programme at a frequency of their choosing.
Primary outcome measures Number of logins and posted messages. Standard self-report measures assessed maternal demographic and psychosocial characteristics.
Results In phase II, the median number of logins was 9 logins (IQR=1–25), and in phase III, it was 10 logins (IQR=0–39). Incident risk ratios from multivariable analyses indicated that compared to mothers with the lowest third of logins in phase I, those with the highest third had 6.43 times as many logins in phase II and 7.14 times in phase III. Fifty per cent of mothers logged-in at least once every 30 days for 147 days after phase I and 44% logged-in at least once in the last 30 days of the intervention. Frequency of logins during phase I was a stronger predictor of mothers’ level of engagement with the intervention than their demographic and psychosocial characteristics.
Conclusions Mothers’ early use of web-based interventions could be employed to customise engagement protocols to the circumstances of individual mothers with the aim of improving adherence and reducing attrition with web-based interventions.
Trial registration number ACTRN12613000204741; Results.
- PAEDIATRICS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Objective data on usage and attrition collected automatically during the course of mothers' use of a nurse-moderated web-based group intervention.
A web-based intervention delivered as part of routine community-based service delivery.
The pattern of results was similar for mothers randomly assigned to the intervention and those assigned to the intervention on the basis of their expressed preference, increasing the likelihood that results apply generally to mothers during the postnatal period.
A potential limitation is evidence that participating mothers in the study may have been from a somewhat more socially advantaged group.
Introduction
Increasing use of the internet by new parents to obtain information and support has encouraged the development of numerous websites and ‘phone apps’ by health services. However, this internet-based approach to service delivery has two limitations. First, there have been few evaluations assessing whether web-based information and support improves maternal and child outcomes.1 Second, achieving high levels of participant engagement with web-based programmes has proved difficult, with many studies reporting low rates of adherence and high rates of attrition.2–6 This is an important issue because a high level of engagement by participants is a key prerequisite for effective universal and targeted web-based programmes.7 ,8
Several different terms have been used to describe level of engagement with web-based interventions.2 ,9 ‘Actual usage’ refers to the amount of exposure that individuals have to a web-based intervention.9 This is typically assessed using number of logins, modules completed and messages posted.9 ‘Intended usage’ is assessed using similar behaviours but reflects the level of usage that individuals need to achieve to obtain maximum benefit.9 The term ‘adherence’ has been defined as the extent to which individuals experience the content of a web-based intervention2 and the percentage of participants who achieve the level of usage required to achieve maximum benefits.9 In this article, we use the latter definition when employing the term adherence.
Currently, very little is known about factors that influence mothers' level of engagement with web-based interventions as most investigations focus on general issues such as user satisfaction and improved user knowledge.10 In other areas of health, it has been reported that personally tailored advice focused on current health concerns,5 level of contact with clinicians2 ,5 ,9 and level of peer support4 may influence engagement with web-based health and lifestyle programmes. It has also been suggested that greater use should be made of information describing participants' use of web-based programmes immediately after enrolment to better predict subsequent levels of adherence and attrition.11
The results of the trial will be reported in a subsequent publication. The aim of the present study was to identify factors influencing mothers' level of usage, adherence and attrition with a novel 6-month nurse-moderated web-based group intervention that provided support for mothers after the birth of their infant.12 The format and content of the intervention was based on traditional face-to-face mothers' groups in Australia that provide a combination of professional and peer support for new mothers during the postnatal period. The groups are led by a nurse and include 10–12 new mothers who meet on a weekly basis for ∼6 weeks. The web-based format of the present intervention made it possible for mothers to participate in a nurse-led peer support group without leaving their home and for support to be provided over a longer period of time than is possible with face-to-face groups.12
In this article, we initially describe mothers' level of use of the intervention during the first week (phase I), during weeks 2–7 (phase II) and during the remainder of the intervention through to group closure at 26 weeks (phase III). Second, we describe mothers' level of adherence during phase II of the intervention based on an expectation of weekly logins during this time, comparable to that expected with traditional face-to-face parenting groups. Third, we describe the extent to which maternal demographic and psychosocial characteristics, and mothers' website activity during phase I predicted mothers': (1) actual usage and (2) level of attrition during phases II and III. Level of attrition was measured as time elapsed before mothers ceased to login and post messages.2 ,13 Finally, we describe the proportion of mothers who dropped out of the study by the time of the 9-month follow-up assessment.
Methods
Participants
Participants were mothers attending one of the six community child health clinics in Adelaide, South Australia, for their initial postnatal health check. During recruitment (March–December 2013), consecutive mothers attending the clinics were approached to participate in a pragmatic preference non-inferiority randomised trial.14
Full details about the trial's design are provided elsewhere.12 In brief, the trial is testing the non-inferiority of outcomes for mothers and infants across two study groups. Mothers in the intervention group received a clinic-based postnatal health check plus web-based support when infants were aged 0–6 months. Mothers in the standard care group received usual care, comprised a standard home-based health check plus advice about the availability of community-based resources. For the purpose of the preference trial, mothers' service preferences were elicited from them at the time that they were recruited to the trial.12 ,14 Mothers who expressed a ‘strong preference’ for a web-based intervention or for standard care were allocated to their preferred group. Mothers without strong preferences were randomised to intervention or standard care. All mothers in the trial were assessed at preintervention when infants were <2 months, and again when infants were aged 9, 15 and 21 months. Following data collection for each assessment, mothers in the intervention and comparison groups were mailed a children's book (value approximately $15). Provided that they completed the assessment, mothers in the intervention group received the book regardless of whether or not they were continuing their involvement with the intervention.
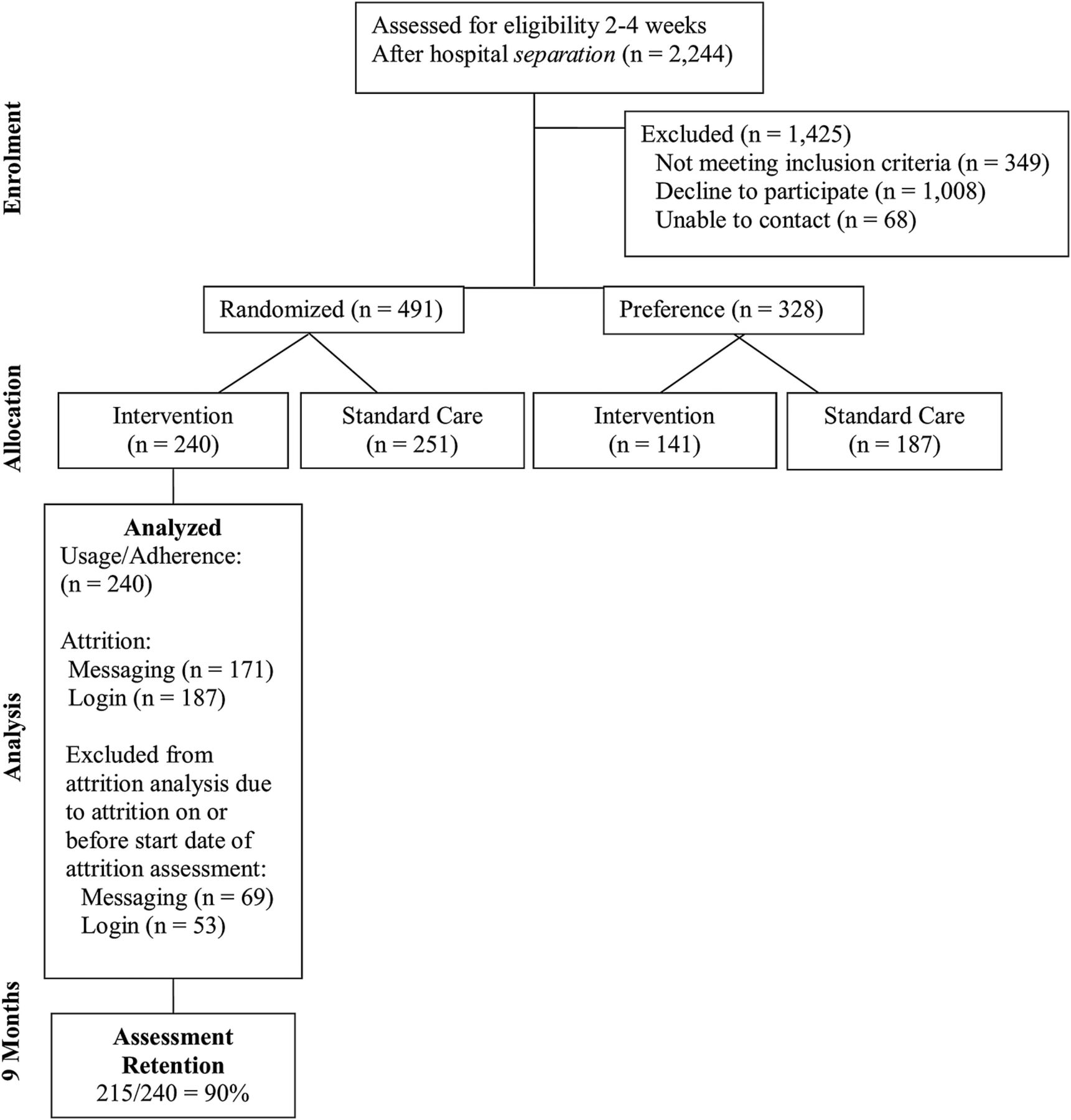
A total of 1827 eligible mothers were identified and 819 of these agreed to participate in the trial (response rate=44.8%). This response rate is consistent with that commonly reported for randomised controlled trials.15 In this article, we report observational data from mothers randomly assigned to receive the intervention (n=240) as there is less risk that unknown selection factors or biases may have influenced adherence and attrition than applied with mothers in the preference group (figure 1). Results for mothers in the preference group were very similar to those for the randomly assigned group and are available in online supplementary appendix A.
Supplementary Appendix

Flow of participants through each stage of the pragmatic preference randomised trial. We report usage, adherence, attrition and drop-out from the randomised intervention arm only.
Intervention
The intervention was comprised three phases. In the first week (phase I), mothers were visited in their home by a trained research assistant and shown how to login to the intervention website. In weeks 2–7 (phase II), the intervention followed a similar course to traditional 6-week face-to-face mothers' groups that meet weekly with a nurse during the postnatal period. During week 8 to group closure at 26 weeks (phase III), mothers could continue to participate in the extended web-based programme at a level of their own choosing.
The web-based intervention could be accessed by study participants only, via mobile phone, tablet or computer. Groups were moderated by one of seven experienced maternal and child health nurses who had completed a purpose-designed 3-day training programme for the web-based intervention.12 The same nurse moderated a group for the duration of the intervention except when on leave, in which case one of the other trained nurses would moderate the group during this time. Mothers used text-based messaging through the website to exchange information and mutual support, and to seek help from their nurse moderator when necessary. Nurses used the group format to (1) provide information directly to mothers, guided by a curriculum that mirrored information normally provided by the child health service and widely used in face-to-face parenting groups; (2) respond to questions asked by mothers; (3) correct misinformation arising during mothers' discussions and (4) direct mothers to additional information within the website and via hyperlinks to other service-approved websites. On average, each group contained 12 mothers (range=9–12).
The ‘mothers’ view of the website was comprised of four components accessed by browser tabs: (1) Home group—contained the chat room and displayed profile pictures of group members. Mothers' and nurses' posts and comments in the chat room were visible to all group members in a similar format to Facebook;16 (2) Milestones and reminders—provided an interactive list of child development milestones and health reminders that could be printed locally; (3) Resources—contained frequently asked questions grouped into topic areas that parallel the topics in the curriculum used by nurses. Nurses could direct mothers to relevant resources as required or mothers could find information themselves and (4) Contacts and assistance—contained useful contact numbers and a portal through which mothers could privately message their group's nurse.
The ‘nurses’ view’ of the website was comprised three main elements: (1) Group dashboard that displayed information about individual groups such as group activities, nursing notes maintained by nurses and responses to quizzes posted by nurses to check maternal knowledge and to stimulate discussion between mothers; (2) Parent dashboard that displayed information about individual mothers, including parent case notes, individual website login activities (eg, where mothers view material but do not post a message) and notifications that mothers have added information about children's milestones and (3) Nurse dashboard that provided nurses with access to their group's chat room and also contained resources that nurses used to support their group (eg, information inserted into the group chat room such as messages, reminders and short quizzes).
The intervention website was managed by system administrators. Any problems with the website were generally addressed on the same day that they were identified.
Measures
Maternal social support was assessed using the Spouse subscale (7 items; score range=7–35) and Isolation subscale (6 items; score range=6–30) from the Parenting Stress Index (PSI),17 the Interpersonal Support Evaluation List—Short Form (16 items; score range=0–48)18 and the Maternal Support Scale, which was adapted from the Diabetes Support Scale19 and was developed specifically for the present study (12 items; score range=12–84). Maternal self-competence was assessed using the PSI Competence subscale (excluding the last two items, 11 items; score range=11–55)17 and the Karitane Parenting Confidence Scale (15 items; score range=0–45).20 ,21 Maternal well-being was assessed using the PSI Role Restriction subscale (7 items; score range=7–35)17 and the Everyday Feelings Questionnaire (10 items; score range=0–40).22 All questionnaires were self-report and used Likert-type response options. Higher scores indicated higher levels of problems for the PSI subscales17 and the Everyday Feelings Questionnaire,22 and lower levels of problems for all other measures.
Demographic information was obtained about participating infants and their parents, including children's gender, parental age (years), education, housing and family characteristics (eg, single-parent or two-parent; number of dependent children).
Actual usage
The web-based system automatically recorded the time and date when mothers logged-in, posted messages and logged-out. If a mother was logged-in but was inactive for >2 hours, she was automatically logged-out to protect confidentiality. Number of logins and number of posted messages were used to assess actual usage. We also identified the number of days on which logins and messages occurred. We did this because it was possible that some mothers were automatically logged-out rather than intentionally using multiple logins on a single day. As well, this approach avoided the possibility that some mothers sent several messages on a single day and then none for several weeks. As there was little difference in the results from analyses using the total number of logins/messages and those obtained using login/message-days, only the former are reported.
Adherence
As noted, the format and content of the intervention was based on traditional face-to-face mothers' groups. Typically such groups are held weekly for 6–10 weeks during the immediate postnatal period. For the purpose of analyses, in this article, we assessed the level of adherence during phase II (weeks 2–7) of the intervention, based on an expectation that during this time mothers would login to the website once per week. It should be noted that we had no specific expectations about the frequency with which mothers should login during phase III (weeks 7–26). As such, we do not report adherence during this period of time.
Attrition
Rate of attrition was based on the number of days from the end of the first week to the day when no login or messaging activity had been recorded for the mother for >30 consecutive days.2 ,13
Drop-out
The percentage of drop-outs is the percentage of individuals enrolled at baseline who did not complete the 9-month follow-up assessment.
Missing data
All mothers had complete outcome data; however, 20 were missing one or more items from the demographic or psychosocial questionnaires. To reduce potential bias from missing data, we used multiple imputation by chained equations in Stata V.13 (Stata Statistical Software SE. Release 13.1. College Station, Texas: Stata Corp; 2014). We generated 20 data sets that were identical for complete data but could differ for imputed values.23 ,24 We used the method of chained equations, randomly sampling the imputed values from the posterior predictive distribution of the missing data.25 ,26 Subsequent analyses adjusted coefficients and variance estimates for variability between data sets according to Rubin's rules.27 Results from sensitivity analyses using complete and imputed data sets were similar. Here we report results using multiply imputed data. Multiple imputation has been widely recommended to reduce bias from missing data, including data collected for baseline assessments.28 ,29
Statistical analysis
Analyses were conducted separately for logins/login-days and messages/message-days. Predictor variables were mothers' demographic and psychosocial characteristics, and their number of logins and messages during phase I (their first week online). For completeness, results from bivariable and multivariable analyses are provided. However, interpretation of results is based on the multivariable results.
Negative binomial regression was used to examine the association between the predictor variables and adherence because the frequency of logins and messages followed an overdispersed Poisson distribution.30 We used standard negative binomial regression rather than zero-inflated models because all participants demonstrated their ability to access the website during the first week31 (results from the zero-inflated models were similar and are available on request). Kaplan-Meier survival estimates and Cox proportional hazards regression models were used to examine the association between the predictor variables and attrition.32
We initially modelled all the psychosocial predictors and early website activity as continuous variables in the multivariable analyses. Based on their tertiles, we then categorised predictor variables showing a statistically significant relationship with the outcome variable in these analyses. The categorised variables were then used in subsequent multivariable analyses. This allowed us to examine the linearity of the trend of the categories created with these variables and we report results of these latter models. All regression models used Stata's vce (cluster) option for estimating robust SEs to take into account possible clustering of outcomes because the intervention occurred in groups33 (Stata Reference Manual: Release 13. College Station, Texas: Stata Press; 2013).
Results from analyses identifying factors that predicted the extent to which mothers posted messages to their groups were similar to results for logins and are reported in online supplementary appendix B.
Supplementary Appendix
Results
The demographic and psychosocial characteristics of mothers are shown in table 1. The median (IQR) age of mothers was 31 years (IQR=28–34 years). The median score on all the psychosocial measures was in the ‘normal range’. Overall, it appears that mothers in the study were a somewhat socially advantaged group who showed a normal range of functioning at the time of their baseline assessment.
Mothers' demographic and psychosocial characteristics (n=240)
Level of actual usage and adherence
Phase I (week 1)
Twenty-two per cent (n=53) of mothers logged-in solely in phase I. The median number of logins during phase I was 3 (IQR=1–7) and the median number of messages posted was 1 (IQR=0–2). During this time, the median number of days during which mothers logged-in at least once was 2 days (IQR=1–4). The median number of days on which they posted at least one message was 1 day (IQR=0–2).
Phase II (weeks 2–7)
Twenty-four per cent of the mothers (n=57) did not login during phase II. The median number of logins during phase II was 9 (IQR=1–25) and the median number of messages was 2 (IQR=0–8). During this phase, the median number of days during which mothers logged-in at least once was 7 days (IQR=1–17). The median number of days on which they posted at least one message was 2 days (IQR=0–5).
In terms of adherence, 44.2% of mothers completed five or more weekly logins during the 6 weeks of phase II. The number of weekly logins by mothers during this phase of the intervention is shown in online supplementary appendix C.
Supplementary Appendix
Phase III (weeks 7–26)
Thirty-three per cent of mothers (n=79) did not login during phase III. The median number of logins during this phase was 10 (IQR=0–39) and the median number of messages was 1 (IQR=0–11). During this phase of the intervention, the median number of days during which mothers logged-in at least once was 9 days (IQR=0–28). The median number of days on which they posted at least one message was 1 day (IQR=0–7).
Factors influencing usage in phases II and III
Among the variables with continuous scores, number of logins in phase I and PSI Role Restriction score had a significant linear relationship with number of logins in phases II and III. When phase I logins were categorised into three groups comprised low, medium or high number of logins, it appeared that the number of logins in phases II and III increased substantially across the three phase I login groups (table 2). However, the number of logins in phases II and III across the three groups based on PSI Role Restriction scores appeared to plateau after an initial increase (table 2).
Median number of logins (IQR) during phase II and phase III of the intervention (n=240)
The multivariable relationship between mothers' demographic and psychosocial characteristics and logins during phase I, and the mothers' number of logins during phase II and phase III, respectively, are given in tables 3 and 4. Mothers with the highest third of logins in phase I had 6.43 times as many logins as those in the lowest third in phase II and 7.14 times as many logins in phase III. Mothers in the highest third of scores on the PSI Role Restriction score in phase I had 1.61 times as many logins as those in the lowest third in phase II and 1.94 times as many logins in phase III.
Bivariable and multivariable IRRs* (95% CI) for factors predicting number of logins during phase II of the intervention (n=240)
Bivariable and multivariable IRRs* (95% CI) predicting number of logins during phase III of the intervention (n=240)
Rate of attrition in phases II and III
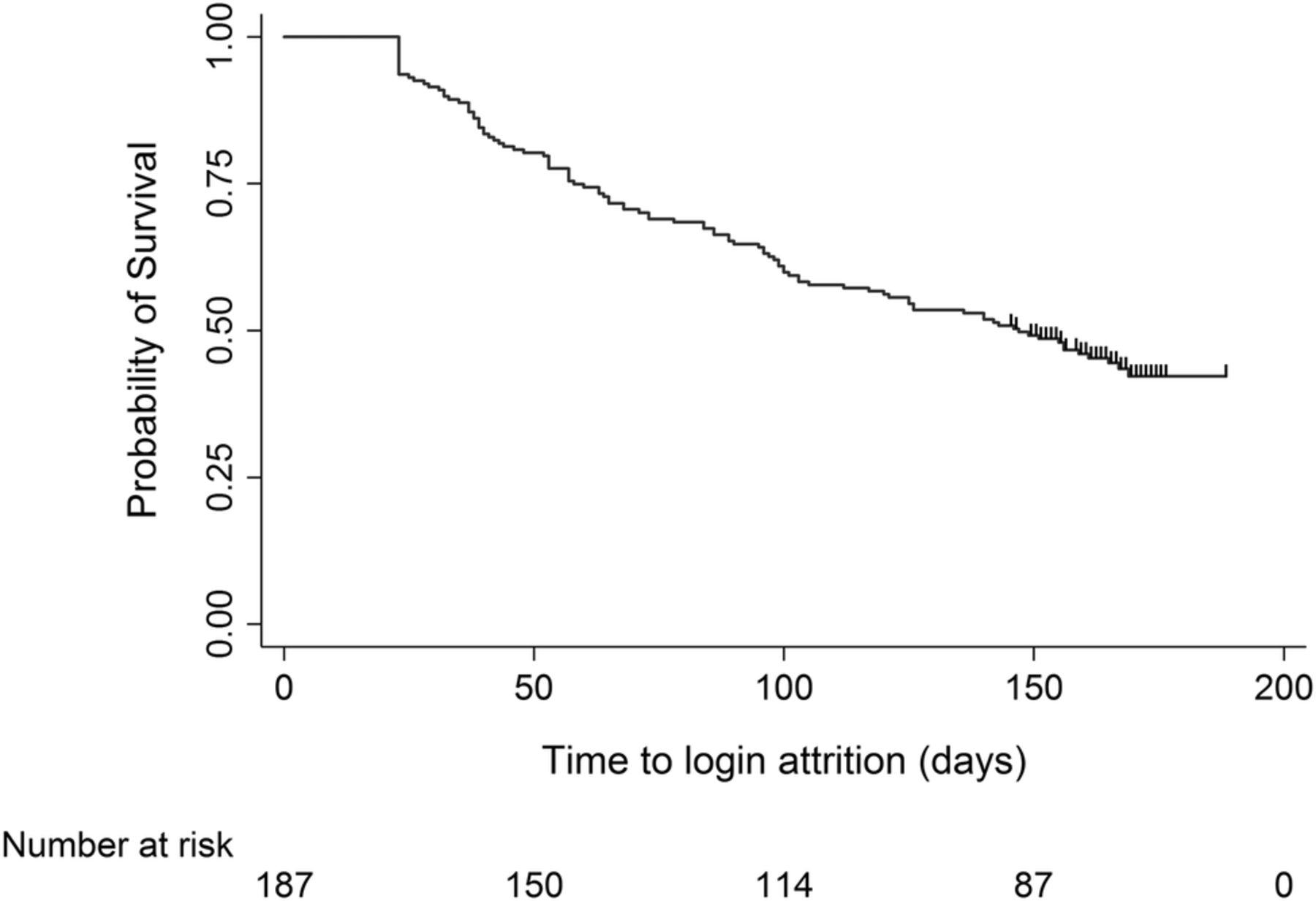
Only mothers with at least one login (n=187) after phase I were eligible for the analyses focusing on attrition. Among these mothers, 50% logged-in at least once every 30 days for 147 days after phase I and 44.4% logged-in at least once during the last 30 days of the intervention. Figure 2 shows the Kaplan-Meier survival curves for login attrition.
{kind=link}
{kind=link}
Kaplan-Meier survivor function indicating the probability of continuing to login after phase I. Mothers were considered to have ceased this activity if they did not login for >30 consecutive days. Time 0 is the first day of the second week for each mother. Only mothers with at least one login (n=187) after this time were included in the analysis. Censored events are shown by small vertical lines on the curve.
When modelling phase I logins and psychosocial predictors as continuous variables in initial multivariable analyses, there was a significant relationship between number of phase I logins, PSI Role Restriction score and PSI Spouse score, and 30 days of inactivity in phases II and III of the intervention. Subsequent analyses where number of phase I logins were categorised into one of three groups based on tertiles showed that mothers with the highest third of phase I logins were 0.18 times as likely as those in the lowest third to have 30 days of inactivity during phases II and III of the intervention. Mothers in the middle third of phase I logins were 0.51 times as likely to have 30 days of inactivity in phases II and III as mothers in the lowest third (table 5).
Bivariable and multivariable HRs* predicting mothers’ risk of attrition after phase I of the intervention (n=187)
Mothers with the highest third and middle third of PSI Role Restriction scores were 0.60 times as likely to have 30 days of inactivity during phases II and III as those in the lowest third of scores on this subscale (table 5). This suggests that mothers who were less comfortable with their parental role were more likely to continue logging-in to the website than other mothers. Mothers with the highest third of PSI Spouse scores were 1.27 times as likely to have 30 days of inactivity during this time as those with the lowest third of scores. Higher scores on the PSI Spouse subscale suggest that mothers perceive they are receiving less support from their spouses. As such, this result suggests that mothers perceiving less support from their spouse are less likely to continue logging-in than mothers perceiving more support.
Drop-outs
It is possible that attrition reflects the level to which participants are engaged with a research trial rather than their engagement with the web-based intervention being evaluated.2 In the present study, 89.6% of participants completed the 9-month follow-up assessment suggesting participants remained highly engaged with the research trial (demographic and psychosocial characteristics of mothers who dropped out are shown in online supplementary appendix D). This suggests that results from the Cox proportional regression analyses reflect the level of engagement with the intervention rather than the trial.
Supplementary Appendix
Discussion
To the best of our knowledge, this is the first study to investigate the extent to which first-time and multiparous mothers who do not have existing physical or mental health problems would engage with an online 6-month nurse-moderated group-based intervention designed to provide mothers with information and support during the postnatal period. This is an important issue because internet-based interventions have the potential to allow community nurses to support larger numbers of mothers during the postnatal period than is possible with face-to-face interventions. For mothers, internet-based interventions offer the added advantages that they do not have to attend meetings at fixed times at a location that may be some distance from where they live. This was noted in written comments by mothers in the present study who reported that they greatly valued the convenience of being able to access the website 24 hours per day from their home rather than having to attend clinic-based appointments at a specific time.
In the present study, during weeks 2–7 of the intervention, when key information and support was being provided in the early postnatal period, 44.2% of mothers logged-in weekly for at least 5 of the 6 weeks. In the later stage of the intervention (weeks 8–26), the median number of days during which mothers logged-in was 10 days (ie, approximately once every 13 days) with the median time to last login being 4.9 months. Judging the relative success of the present intervention to engage mothers is difficult due to lack of information about engagement levels with comparable interventions delivered at a population level. In the area of mental health, engagement with online interventions has been highly variable with attrition ranging from 1 to 50% depending on the type of intervention.2 In South Australia, ∼2000 mothers (10% of births per year) attend a face-to-face postnatal group.34 This is substantially lower than the uptake in the current trial where 45% of mothers approached agreed to participate in the trial. Of these, the majority (60.0%) were happy to be randomised to either the internet-based intervention or standard care, while 17.2% expressed a strong preference for the internet-based intervention. There are no data on attrition levels for postnatal face-to-face groups in South Australia, but informal advice from experienced nurses suggested that of the 12 mothers who are typically enrolled in each group, ∼10 mothers (84%) attend initial meetings and 8 mothers (67%) complete the 6-week programme. If these estimates are correct, it would suggest that the attrition rates in the present intervention may have been somewhat higher than traditional face-to-face groups.
An important finding from the study was that frequency of logins and messages during the first week were stronger predictors of mothers' level of engagement with the intervention than their demographic and psychosocial characteristics, with the possible exception of satisfaction with parental role. As noted by Van Gemert-Pijnen et al,35 web-based interventions are readily able to monitor participants' usage patterns. Results from the present study suggest that information about mothers' early use of a web-based intervention could be employed to customise engagement protocols so that they are better tailored to the circumstances of individual mothers. In the context of a web-based parent-support programme, for example, nurses could use the information to identify mothers who do not login during their first week. They could then directly contact these mothers to identify current problems and encourage the mothers to engage with the web-based programme. This approach has the potential to enable nurses to better target this additional support to those most likely to benefit from it, rather than using a ‘one size fits all’ approach.
It has also been noted that the vast majority of participants enrolled in web-based interventions login but do not contribute to group discussions.36 In this area, the level of participation of mothers with the present intervention was substantially better than that reported for web-based interventions focused on smoking cessation, problem drinking and mental health problems.36 In such interventions, it has been found that ∼1% of participants contribute the vast majority of content to the interventions, 9% of participants contribute sparingly and 90% of participants read content but do not contribute to the interventions.36 In contrast, in the present study, of those mothers who logged-in after phase I (n=187), the top 10.2% of mothers (comprised 19 mothers, each of whom sent 54 or more messages after phase I) generated ∼42.6% of the discussion content. Fifty-two per cent (n=98) of mothers who logged-in after phase I posted messages on at least 6 days (ie, on average, they posted one message per month) and only 8.6% of mothers read content but did not contribute to it. This is an important finding because although they may gain benefit themselves, individuals who read website content but contribute little to it add less value to a web-based intervention than those who participate actively in ongoing discussions.
There are three possible explanations for the higher level of contribution by mothers in the present intervention. First, nurses actively encouraged interaction between mothers in their groups and this may have led to greater participation by mothers. This is consistent with findings from previous studies demonstrating that increased opportunity for interaction with counsellors and more extensive dialogue support can improve engagement with web-based interventions.5 ,9 ,11 Second, the intervention was offered to women at a time when they experience a major role transition and it focused specifically on problems commonly experienced at this time. There is evidence from other studies that the latter is associated with level of engagement with web-based interventions.5 Third, the intervention provided easy access to ‘just-in-time’ information for new mothers and to professional and peer support during the postnatal period. To date, social support has been used infrequently by web-based interventions, despite substantial evidence of the value attached to it by individuals with health problems and its importance for achieving behaviour change.9
Finally, it is notable that 89.6% of mothers completed the 9-month follow-up assessment. This is higher than the percentage who were continuing to login to the website in the later stages of the intervention. A possible explanation is that at this stage of the intervention, mothers were using the support available at a level that fitted their needs, with most not requiring a large amount of support after the initial postnatal period. It is also possible that mothers using this approach did not consider that they had ‘dropped out’ of the trial, rather they simply did not have a need for additional information at the time. Some support is available for this suggestion in qualitative comments made by mothers such as ‘only logged on when I needed advice’, ‘wish I had more time for eMums’ and ‘it was a quick and easy way to get information and/or reassurance [when required]’. Alternatively, mothers may have preferred to obtain support from other sources because the intervention was no longer addressing their needs. However, this latter explanation seems less plausible and is also not consistent with the high follow-up response rate and the many positive written comments provided by mothers at the 9-month follow-up assessment.
Strengths and limitations
Strengths of the study are its use of objective data on adherence and attrition obtained during the course of an online intervention that was delivered as part of routine community-based service delivery in the health system. Furthermore, the pattern of results was similar for mothers randomly assigned to the intervention and those assigned to the intervention on the basis of their expressed preference. This similarity increases the likelihood that results would apply generally to mothers using a similar nurse-moderated web-based group intervention during the postnatal period. Potential limitations include evidence that participating mothers were from a somewhat more socially advantaged group. However, Organisation for Economic Co-operation and Development (OECD) data show that 44% of Australians aged 25–34 have tertiary qualifications compared with 50.7% of participants in this study, suggesting that participating mothers may not be greatly more advantaged than the general population.37
Conclusion
Nurse-moderated web-based group interventions have the potential to provide information and support to new mothers during the postnatal period. Information about mothers' early website activity with web-based interventions could be employed to customise engagement protocols so that they are better tailored to the circumstances of individual mothers, thus maximising the potential benefits for mothers and their infants.
References
Footnotes
Contributors MGS conceptualised and designed the study, analysed and interpreted results from the study, and drafted the manuscript. CER helped analyse and interpret results from the study and draft/revise the manuscript. KB and DJ helped conceptualise and design the study and draft/revise the manuscript. ACPS helped analyse and interpret results from the study and draft/revise the manuscript. CM-K, JDP, JJC and DM coordinated and supervised data collection, and helped draft/revise the manuscript. MNM helped analyse and interpret results from the study and draft/revise the manuscript. JWL helped conceptualise and design the study, analyse and interpret results from the study, and draft/revise the manuscript.
Funding This work was supported by a National Health and Medical Research Council of Australia—Partnership Project, grant number: 1016281. JWL is supported by an Australia Fellowship from the National Health and Medical Research Council of Australia, grant number: 570120. ACPS is also supported by funds from the Australia Fellowship awarded to JWL. These researchers are independent of the funding bodies. The other authors have no financial relationships relevant to this article.
Competing interests KB is the Director of Child and Family Health Services (CaFHS), and DJ is the Nursing Director of CaFHS. The authors have no other conflicts of interest to disclose.
Ethics approval The study protocol was approved by the Women's and Children's Hospital Human Research Ethics Committee (REC2368/4/17).
Provenance and peer review Not commissioned; externally peer reviewed.