Article Text

Abstract
Objectives To examine the basis of multidisciplinary teamwork. In real-world healthcare settings, clinicians often cluster in profession-based tribal silos, form hierarchies and exhibit stereotypical behaviours. It is not clear whether these social structures are more a product of inherent characteristics of the individuals or groups comprising the professions, or attributable to a greater extent to workplace factors.
Setting Controlled laboratory environment with well-appointed, quiet rooms and video and audio equipment.
Participants Clinical professionals (n=133) divided into 35 groups of doctors, nurses and allied health professions, or mixed professions.
Interventions Participants engaged in one of three team tasks, and their performance was video-recorded and assessed.
Primary and secondary measures Primary: teamwork performance. Secondary, pre-experimental: a bank of personality questionnaires designed to assess participants’ individual differences. Postexperimental: the 16-item Mayo High Performance Teamwork Scale (MHPTS) to measure teamwork skills; this was self-assessed by participants and also by external raters. In addition, external, arm's length blinded observations of the videotapes were conducted.
Results At baseline, there were few significant differences between the professions in collective orientation, most of the personality factors, Machiavellianism and conservatism. Teams generally functioned well, with effective relationships, and exhibited little by way of discernible tribal or hierarchical behaviours, and no obvious differences between groups (F (3, 31)=0.94, p=0.43).
Conclusions Once clinicians are taken out of the workplace and put in controlled settings, tribalism, hierarchical and stereotype behaviours largely dissolve. It is unwise therefore to attribute these factors to fundamental sociological or psychological differences between individuals in the professions, or aggregated group differences. Workplace cultures are more likely to be influential in shaping such behaviours. The results underscore the importance of culture and context in improvement activities. Future initiatives should factor in culture and context as well as individuals’ or professions’ characteristics as the basis for inducing more lateral teamwork or better interprofessional collaboration.
- patient safety
- teamwork
- quality improvement
- teams
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The first study in healthcare to examine clinicians’ professional differences in controlled laboratory settings.
Experimental novelty included asking groups outside of their normal healthcare settings to undertake three experimental tasks to test their interactions.
Participants were randomised to groups, but the overall inclusion of participants was purposive.
Participants were tested for their ideology, personality, propensity for power and team orientation using validated scales.
Some professionals (eg, allied health professionals) were not represented in some of the experimental tasks.
Background
Healthcare delivery systems ideally consist of well-functioning interprofessional teams working towards the common goal of caring for patients,1 applying the best evidence,2 and providing high quality, safe care within complex organisational contexts and cultures. However, research on teamwork in health settings indicates that professional groups can hold differing views, perspectives and attitudes, as illustrated by survey studies of O'Leary et al3 of 159 nurses and doctors, Wauben et al4 of 221 surgeons, nurses, anaesthesiologists and nurse anaesthesiologists and Gehring et al5 of 630 primary care physicians and nurses. Please refer to box 1 for the definitions of terms used throughout this paper.
Definitions
Hierarchy: A layered social structure which conceptualises superior and subordinate relationships transitively, in rank order; often depicted graphically, for example, in an organisational chart. In healthcare, the ‘clinical pecking order’ is one key example.
Interprofessional: The skills of the different professions overlap.6
Intraprofessional: Collaboration within a profession.6
Multiprofessional: Professionals work alongside each other, relatively independently.6
Organisational context: The setting in which practice takes place.7
Organisational culture: Recurring patterned behaviours, practices, attitudes and values describing settings infused with an ethos of ‘the way we do things around here’ contrasted with ‘the way they do things over there’.8
Stereotype: The pattern of characteristics that are attributed to a group external to one's own reference group; often, out-groups are assessed to be inferior, with negative characteristics, and one's own group to have superior, or positive characteristics.
Teamwork: The combined activities of a group of people working effectively towards common ends.9
Tribe: An in-group exhibiting strong bonds with tendencies towards inward social loyalty and conformity across the membership.
Studies have also shown10 ,11 that providing team training of various types (eg, modelling crew resource management (CRM), conducting simulation training, teaching communication skills and introducing ward rounding) is related to improvements in attitudes and knowledge, and that interprofessional collaboration can improve as a consequence.12–15 A systematic review found that 13 of 14 evaluation studies demonstrated an enhancement in teamwork as a result of team-based interventions16 and a Cochrane review of interprofessional collaboration showed that interprofessional rounds, meetings and an interprofessional audit can contribute to improved healthcare processes and outcomes in specific circumstances.17 ,18 Cohesive healthcare teams are linked to improved patient outcomes, and patient and staff satisfaction.1 ,19 In essence, effective teamwork involves cooperation and communication between professional groups, as well as an understanding and respect for the different roles the professions play within the broader team.20
However, despite the shared objective of patient well-being, there is a widespread view, notwithstanding normative hopes for better teamwork that clinical care is too often provided by tribes of relatively independent doctors, nurses and allied health professionals with low levels of interaction between the professional groups.9 ,21 Doctors, nurses and allied health professionals often work intraprofessionally, tending to seek out other members of their own profession when problem-solving, seeking professional advice or socialising.22 Yet poor interprofessional collaboration can adversely affect the quality of care delivered to patients,17 ,23 with the potential for patients to fall through the system's cracks.24 Substantial efforts to induce multidisciplinary teamwork,25 interprofessional collaboration12 and to traverse historical professional divides26 are strong indicators that there is a need to address this issue. Such divisions act as barriers to more inclusive teamwork27 and better care.28
It has proven difficult to create bridges across these profession-based silos and integrate activities of workplace groups.12 There are historical, cultural, behavioural and attitudinal reasons for the continuation of this state of affairs. Historically, gender divides existed within healthcare roles, with male doctors being hierarchically dominant compared with the traditionally submissive nature of female nurses.1 This resulted in a power imbalance and ongoing rivalries labelled ‘the doctor–nurse game’29 ,30 first noted almost 50 years ago. The emergence of a multiplicity of allied health professionals over the last 40 years increased the range of services to patients and also the potential for further fragmentation of teamwork based on professional distinctions and gender differences.
So, despite the breakdown of gender-restricted roles and other cultural typecasts across society as a whole, modern healthcare professionals still too often appear to function in discipline-specific groupings. Although doctors, nurses and allied health professionals share overall goals relating to the care of patients, they have differing histories, priorities, roles, expectations, education and training, which often exacerbates disconnections between them.20 Furthermore, organisational factors such as the physical layout of hospitals and differing staff shift schedules can limit the opportunities for interprofessional interactions,20 ,21 ultimately resulting in physical, social and psychological segregation of the professions from one another.
In-groups and out-groups in healthcare and elsewhere
Tajfel and Turner suggest that, beyond healthcare, poor group interactions can be explained by social identity theory.31 Individuals form groups based on compatible social factors such as class or race, or in the case discussed here, professional affiliation.32 Thus, ubiquitous group identification and a collective sense of belonging influence individuals’ self-concepts and manifest as in-group versus out-group rivalries,32 more colloquially known as the ‘us versus them’ attitude. This is tribalism: the clustering of people with shared tendencies in an in-group. People within the same group tend to agree with, and show favouritism towards, fellow members of their group, whereas people outside of that group are often judged less favourably even in instances where group membership has been arbitrarily allocated.33–35 Within healthcare settings, stereotypes about doctors, nurses and allied health professionals persist, for example, doctors can often be viewed by others as strong leaders with high academic ability, but having poor interpersonal skills compared with nurses and allied health professionals;36 nurses can be seen by others as hierarchical and rule oriented;37 ,38 and allied health staff can be considered by others as passive political players and relatively powerless in the face of medical and nursing political structures.39 We do not know the extent to which these stereotypes vary, or if the distinctions they represent hold under controlled conditions.
We do know that the attitude structures of the three main professional groups differ substantially, and this may be a core reason for poor levels of interprofessionalism when it manifests. In studies investigating their relative views on workplace issues such as interprofessional collaboration and teamwork structures, doctors tend to hold strong, certain and critical attitudes;13 ,40 nurses’ attitudes tend to be collective, intense and polarised;40 and allied health professionals tend to express the most positive attitudes but feel less certainty about the attitudes they express.40
It remains unclear to what extent the professionalised differences experienced anecdotally by participants in workplaces or measured on attitudinal scales are stereotypes of the three professional groups or actual manifestations of behavioural repertoires. If we are to encourage greater levels of teamwork and interprofessional practice in support of improved quality of care, we need to understand the underpinnings for poor teamwork based on professional differences. One way to do this is to examine the interactions of the main clinical professional groups in controlled settings, that is, by taking them out of the workplace cultures in which they are embedded, and to test their team orientations. These characteristics might be important in understanding the basis of in situ organisational silos, professional hierarchies and tribal behaviours40–44 which impede team-based care.
Aim
We aimed to characterise group behaviours of homogeneous groups of doctors, nurses and allied health professionals, and heterogeneous groups combining members of all these professions, to investigate differences and similarities in their interactions and problem-solving approaches, in an experimental setting. On the basis of the foregoing, we hypothesised that (H1) individual representatives of professional groups would show differences in their propensity for teamwork, attributable to their professional group characteristics, for example, in personality, collective orientation, conservatism and teamwork style; (H2) gender differences would be detectable among mixed gender teams and would be observed in tangible team role behaviours; (H3) homogenous groups of doctors, nurses and allied health professionals would differ from each other in their teamwork style; and (H4) heterogeneous groups would interact differently, and be less team orientated, when compared with homogeneous groups.
Method
Participants
Participants were 133 health professionals employed in the healthcare system in Australia. They comprised 24 doctors, 60 nurses, 39 allied health professionals and a smaller number (10) of other health professionals, such as scientific officers who were combined with the heterogeneous groups. To facilitate enrolment, the study was included as an optional professional development activity as part of the programme at two healthcare conferences in Australia in 2012 (the Annual Australasian Conference on Safety and Quality in Health Care in September 2012 and the Australian National Primary Health Care Conference in November 2012). In total, 84 participants were recruited in this way. A further 49 participants, all of whom had trained previously as doctors, nurses and allied health professionals, volunteered from a master's programme offered at the University of New South Wales in Sydney, Australia, in 2013. No inducements were offered to any participants to elicit their task performance, but a prize of an Apple iPad was offered at the primary health care conference to test whether this improved participation rates. Eligibility for the iPad prize was contingent on participation, but not linked in any way to performance of the group tasks.
Study design
The study purpose designed or modified and then applied three team-based experimental tasks to assess different aspects of intragroup interactions (health case study task, jigsaw puzzle task and healthcare budget allocation task; figure 1). We used a variety of tasks to reduce bias inherent in choosing only one type of task. Participants volunteered for scheduled session times and were then randomly assigned to one of the three tasks. Within these tasks participants were randomly allocated to either a homogeneous or heterogeneous professional group, creating 35 groups in total. Some direct allocations were made so that each group had sufficient members from the appropriate professional groups. Homogeneous groups consisted of members drawn from a single profession (ie, either all doctors or all nurses or all allied health professionals) while heterogeneous groups consisted of members from more than one profession within the same team (ie, a combination of doctors, nurses, allied health professionals and others). Each task required individual groups to have a maximum of n=6 members and a minimum of n=3 members; however, the jigsaw task required synchronous participation of three individual groups to run a session (with a minimum of n=9). Efforts were made to have an equal number of members from each profession in mixed groups, but this was not always possible due to some participants’ unavailability.

Study design.
Materials
Pre-experimental questionnaires
Four pretask personality questionnaires were used to assess individual differences between participants. These were as follows: a ten-item version of the Big Five Inventory, measuring five personality dimensions, viz openness, conscientiousness, agreeableness, neuroticism and extroversion;45 the 16-item Machiavellian Personality Scale, measuring Machiavellian tendencies such as distrust and manipulation of others;46 the 15-item Collective Orientation Scale, assessing participants for their propensity to work collaboratively in a team environment;47 and a 25-item modified version of the Henningham Social Conservatism Scale, measuring politically conservative values,48 from which two items were removed as they were not relevant to the current study. In addition, an in-house demographic questionnaire recorded each participant's gender, age group, profession, type of institution in which they worked, years of experience in their current position and years of postgraduate working experience. The 16-item Mayo High Performance Teamwork Scale (MHPTS), measuring the high performance teamwork skills49 shown to be important contributors to patient safety50 ,51 was used as a post-task questionnaire to assess participants’ views on how they had perceived their team's approach to the assigned task. Independent, trained raters were also given the MHPTS to assess group performance.
Experimental tasks
In addition to completing the rating scales described above, enrolees participated in one of the following team-based tasks.
Healthcare case study task: Each participant in a team was provided with a purpose-designed healthcare case study vignette that described a challenging healthcare management scenario. Each group was instructed to imagine they had been asked to resolve serious problems at a hospital. Participants were then asked to complete a structured response sheet detailing their group's proposed strategy to manage change in the problematic environment as well as an evaluation of their chosen strategy.
Jigsaw puzzle task: Three different 49-piece jigsaw puzzles were used in this task. Two pieces were removed from each jigsaw puzzle box and placed in the boxes of two of the other jigsaw puzzles (subsequently assigned to different teams), such that each jigsaw contained one piece from each of the other two puzzles. This jigsaw task was run among three groups simultaneously. Each group was provided with one of the three puzzles, disassembled and shuffled in a large envelope. Participants were asked to complete the jigsaw puzzle within 10 minutes. No information was given regarding the missing pieces. Further details of the task are available elsewhere.52
Healthcare budget allocation task: Each participant in each group was provided with (a) a synopsis of the Australian Federal Government's health budget for the previous financial year, and (b) the growth in health expenditure over the previous five years, in dollars and as a percentage increase. In addition, a single-page of typed text provided definitions for each item specified in the health budget. Participants were instructed to use a purpose-designed response sheet to allocate expenditure to a list of sectors (eg, aged-care, hospitals, research), as well as explain what they would do with the growth funding.
Settings and equipment
Each task was conducted in clean, well-appointed, quiet rooms equipped with tables and chairs as appropriate for each task. Since data collection occurred in situ at various locations, different rooms were used at different stages of the study. A video camera (Panasonic HDC-SD90 recording at 1920×1080i resolution) was mounted on a tall tripod and located to the front of each table of participants in order to maximise visibility of facial expressions, hand movements and spoken interactions. A microphone (Zoom H4n) was unobtrusively placed at the table, and connected by wire to the video camera, to capture clear audio of participants’ speech. In order to control for unintentional between-group differences in experimenter-participant interactions, the task instructions were recorded as a digital video file (‘talking head’) that was presented to participants using a digital projector prior to task commencement. The digital projector was also used to project the image of a countdown timer indicating the time remaining relevant to the specific task, which allowed participants to pace their task progress. Experimenters activated the instructional video at commencement of each task, and then left the room for the task duration.
Experimental study procedures
Prior to enrolling in the study, potential participants were informed (either as an announcement at one of the conferences, or by the lecturer in the master's course (JB)) that the task was an exercise to better understand interactions between individuals while working on a group task. At the conferences, participants were permitted to select the most convenient time from a number of available time slots during the day. For students from the master's course, the study was conducted during the usual class-time. The small number of class members who elected not to participate (n=2) were given a different class activity.
Participants were asked to read and sign information and consent forms before completing the battery of demographic and personality questionnaires. At this time they were also allocated a randomised numerical code number that would allow identification of individuals in the video recording and eventual linkage with their responses to the questionnaires, while not revealing their identity or professional background to other participants or the research team members co-ordinating the study task. Thus, research team members were blinded to participant identity and professional background and JB did not participate in the experiments. After completion of the pretask questionnaires, participants were brought into the task room, where each group of participants was seated at separate tables. No additional instructions were given as to how groups should operate or make decisions (eg, whether they should decide by consensus or majority). At the end of the allocated time, the ‘talking head’ video announced that the allocated time had expired and everybody should stop working on the task (if they had not already finished).
Post-experimental measures
Postexperimental task measures consisted of (1) self-assessed MHPTS, (2) rater-assessed MHPTS and (3) blinded observations. The MHPTS was administered immediately after the experimental tasks to all participants for later comparison with rater-assessed MHPTS scores. The MHPTS has been validated for self-assessment by novice healthcare team training participants,49 and assessment by independent observers.14 Once the research team collected all the task response sheets and post-task questionnaires, the participants were debriefed regarding the aims of the study and given the opportunity to ask questions.
The digital video files were transferred to DVDs in randomised order within groups, resulting in data of 35 groups performing tasks of 15–20 min duration each. The videos were analysed by three independent raters who were blinded to the professional composition of the group. Raters completed one-half day of training on how to use the MHPTS prior to rating the video behaviours, and achieved high agreement when rating two practice scenarios. As an additional measure of teamwork performance, blind observations were conducted by an independent observer. These semistructured observations consisted of viewing all video tapes and noting team interactions using a guideline based on CRM teamwork skills including; communication, leadership, decision-making, task management and situational awareness (see online supplementary file 1).53 The observation guideline was constructed by a researcher (RC-W) with extensive experience in CRM training and research in healthcare and other industries.
Supplementary file
Behavioural data procedures
Behavioural data were cleaned and entered into an SPSS statistics datasheet (V.22), missing values for questions 1–8 were allocated a ‘0’, and missing values for questions 9–16 were allocated a ‘1’ in accordance with published guidelines.27 For self-assessed data, participants’ ratings of the 16-behaviour statements for each scenario were summed, to give a participant team score for each scenario.
Ethics approval
Ethics approval for the study was obtained from the University of New South Wales’ (UNSW) Human Research Ethics Committee (UNSW HREC/HC12040). Active written consent was obtained from participants for all aspects of the research, including consent for audio–video recording of participant behaviours and later analysis.
Results
Participants
A total of 133 healthcare professionals participated in the study; the breakdown of participants by qualification, gender, age, experience and time in current position is shown in table 1. Participants worked in a large variety of healthcare settings, including public hospitals (n=53), private hospitals (n=8), community health services (n=13), general practice (n=11), academic organisations (n=4), health departments or other government agencies (n=19), consumer groups (n=1) and elsewhere in healthcare, or in more than one location or role (n=23).
Participant characteristics
There were 35 groups in total. For the healthcare case study task and healthcare budget allocation task, the smallest group size was n=3 and the largest was n=6 participants. For the jigsaw task, the smallest number of participants in each session was n=9 and the largest was n=18 participants.
Professional group differences
Analyses of covariance (ANCOVAs) were conducted for each of the scales comparing doctors, nurses and allied health professionals, while controlling for gender. Previous research54 suggested gender was the most important variable to control. The size of the sample precluded controlling for multiple variables in the analysis but post hoc examination of the data showed no significant differences among variables, for example, those associated with age or years since graduation. No significant differences were found between the professions in collective orientation, four of the five personality factors, Machiavellianism or conservatism. There was a significant difference between professions for one of the personality factors: agreeableness F(3, 124)=0.19, p=0.021, with allied health staff scoring as more agreeable (mean=4.1, SD=0.8) than ‘other’ (mean=3.3, SD=0.9).
Gender differences
There was a significant effect of gender on Machiavellianism Scale scores after controlling for the effect of profession, F(1, 124)=17.9, p<0.001, with females scoring as more Machiavellian (mean=3.33, SD=0.40) than males (mean=2.98, SD=0.49). Both males and females appear to become significantly more Machiavellian the longer they had spent in their profession. There was a significant difference between female Machiavellianism scores for those who had between 6 and 10 years’ experience (mean=3.15, SD=0.097) and those with over 20 years’ experience (mean=3.47, SD=0.06); mean difference=0.325, p=0.044, 95% CI (0.005 to 0.646). There was a significant difference between male Machiavellianism scores for those who had <5 years’ experience (mean=2.23, SD=0.21) and those with over 20 years’ experience (mean=3.20, SD=0.12); mean difference=0.968, p=0.006, 95% CI (0.209 to 1.726).
Homogenous teams of healthcare workers
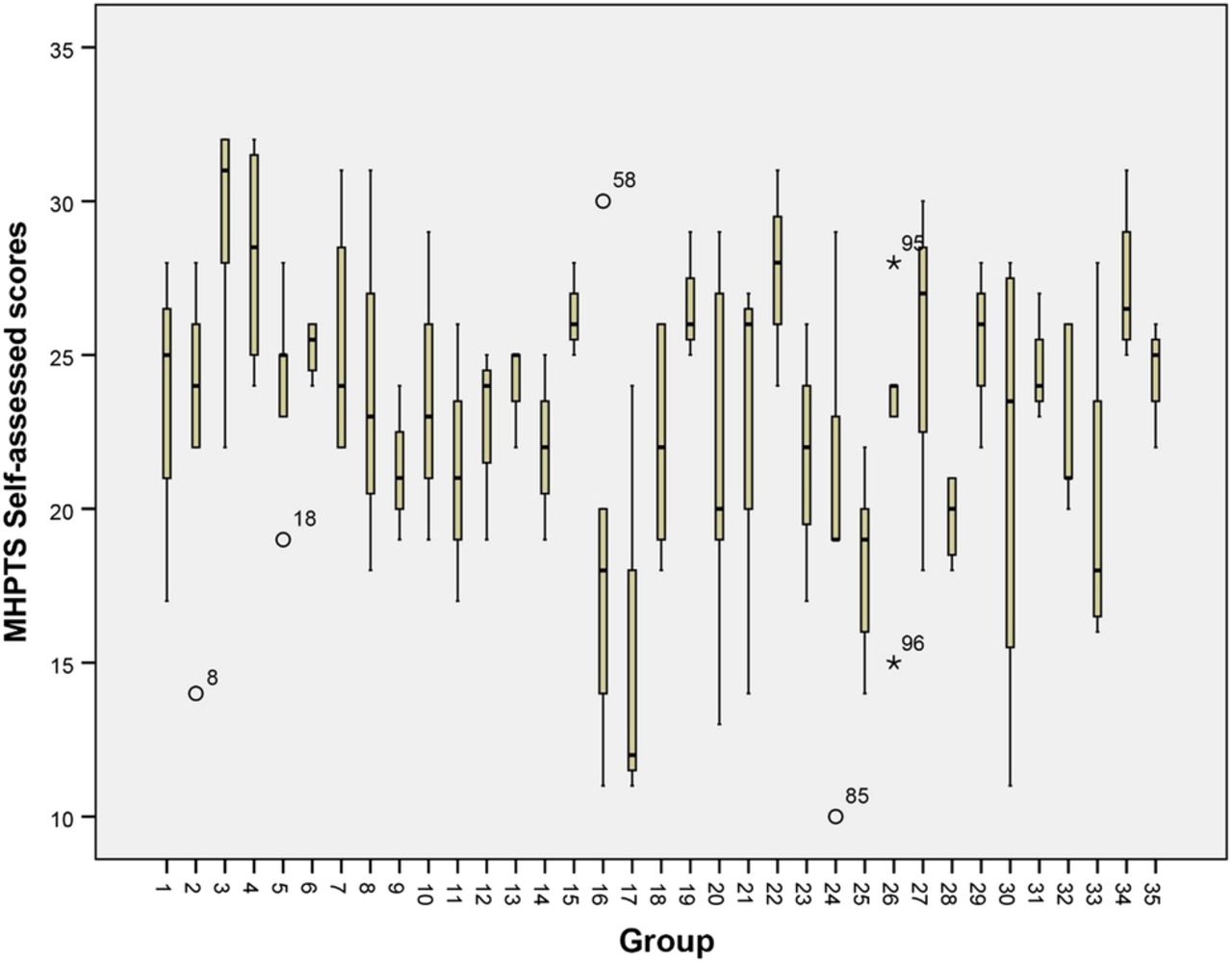
Participants’ self-assessed MHPTS scores were summed and averaged for each group to create a mean group score, with a maximum available score of 32, the highest possible teamwork score. For rater-assessed MHPTS data, scores on the 16 behaviour statements for each scenario were summed, to give each group a total score for each task. As is commonly found with the MHPTS instrument,49 self-assessed scores were higher than independent rater scores (M=23.1 and M=18.0, respectively); however, the self-assessed scores were not able to be used further due to the excessive variation of scores within groups (figure 2). In one healthcare budget allocation task, for example, self-assessed scores within one five-person team varied from 14 to 28.

Mayo High Performance Teamwork Scale (MHPTS) self-assessed scores.
As raters were blinded and did not observe the same teams as each other, scores were not able to be correlated. Despite this, raters’ scores had a high frequency distribution and similar distributions between raters (figure 3), which, in combination with high rater agreement shown when rating training scenarios, suggests a degree of consistency between raters’ scoring. ANCOVAs were calculated using rater scores comparing homogeneous teams of doctors, nurses, allied health professionals and combined teams, while controlling for gender. No significant differences were found between teams of different compositions, F(3, 31)=0.94, p=0.43.

{kind=link}
{kind=link}
{kind=link}
Frequency distribution of raters’ Mayo High Performance Teamwork Scale (MHPTS) scores. DM, Danielle Marks; EV, Elia Vecellio; RCW, Robyn Clay-Williams.
Interaction in heterogeneous groups
Observers in the blinded observations reported that teams performed well, interactions were relatively smooth and functional, and participants were observed to contribute effectively to group outcomes. Case study results, jigsaw completions and budget allocations were all attempted with due diligence. No obvious differences were apparent between homogenous and heterogeneous groups in problem-solving styles, teamwork orientation, tribalism, hierarchy or stereotypes.
No differences between groups’ behaviours were identified based on CRM teamwork skills, including communication, leadership, decision-making, task management and situational awareness. Groups chose a scribe in studies which required a scribe and males were disproportionately selected. In the seven teams where males and females were available to scribe, males were scribes for five teams. Nurses were more likely to be scribes in the mixed heterogeneous groups. In the eight mixed groups which contained nurses they were scribes for five teams. In heterogeneous teams, doctors were more prone to ask a question, direct the project or (in the jigsaw task) discover that a puzzle piece was missing. On the eight occasions when questions were asked in mixed groups four were asked by doctors. The questions asked by doctors were typically of a nature designed to progress the task (eg, ‘should we move on?’ or ‘have we finished (task)?’).
Discussion
This is the first study of its kind in healthcare, so far as we are aware. While well established in psychology and social psychology, conducting experimental work among healthcare teams in controlled settings is at an embryonic stage. In a laboratory-based setting, participants still ostensibly bear the hallmarks of their socialisation (they are still doctors, nurses and allied health professionals, after all) but they were not, while in our laboratory setting, infused with the immediacy of the cultural milieu of their home workplace setting.
Interprofessional teamwork is a cornerstone in delivering high-quality, safe care. When we took healthcare professionals out of their normal work environments and had them interact under different conditions to observe teamwork behaviours, we found few of the traditional, stereotypically patterned behavioural differences that have been attributed to the professional groups, that is, tribalism or hierarchical or stereotypical displays.9 ,21 When these styles manifest in modern healthcare settings, as they seem to do ubiquitously,9 ,12 ,17 ,21 ,22 ,24–26 then we can point to the workplace cultures as the genesis for the behaviours rather than intrinsically different characteristics of doctors, nurses and allied health professionals, or the individuals who make up the clinical professions.
In short, if you remove clinicians from their normal context, and put them in a laboratory environment, tribalism, stereotypes and hierarchically-laden behaviours dissipate to a considerable extent. Thus, while social identity theory offers a powerful explanation for professional group differences in healthcare settings, we did not detect such professional identity differences when we controlled for the setting by taking people out of it.
Profiles of participants
We found no major differences in demographic profiles, personality, Machiavellianism, conservatism or team orientation between professional groups at baseline. H1 was therefore not supported: on the strength of our data, contrary to expectations, there are few grounds for supposing a priori that aggregated individual differences are the key influence in determining the characteristics of the professional groups. In fact, observers could not tell from the behaviours of participants in the three tasks who was a doctor, nurse or allied health professional.
There have been few studies in healthcare examining the relationships between gender, personality and ideology. We identified no gender differences other than in one aspect—Machiavellianism, where females had higher scores than males: H2 was therefore rejected. For both genders, Machiavellianism increased with number of years of professional experience. In practice, this may mean that individual clinicians of both genders become more aware of their capacity to exercise power with age and experience.
Self and raters’ judgements of group performance
In regard to self-assessment of the teams’ performance, there was little agreement between participants’ judgements. Either participants have difficulty judging team orientation, or they have little agreement on what constitutes a good team. Independent raters judged that team performance in the main was smooth and functional and where team performance differed this could not be attributed to team composition.
Task performance
We found few discernible differences in team orientation or task performance between homogenous and heterogeneous groups. H3 was therefore rejected. In their laboratory task performance, the key problem-solving strategies of clinicians, in the team tasks we set them, was a kind of collegial collaboration. In heterogeneous teams, doctors were more likely to ask questions. Doctors were also more likely to direct progress in a task or point out if something was missing (eg, a jigsaw puzzle piece). Throughout the three tasks, scribes tended to be male. In the non-jigsaw activities, nurses were more likely to be scribes, self-selected, in the mixed heterogeneous groups. This provides modest supporting evidence for the view that the clinical pecking order replicates itself outside of the workplace.9 ,21 But, apart from these minor instances, few other traditional stereotypical or hierarchical behaviours were observed although there were many opportunities for these kinds of behaviour to manifest. H4 was therefore only partially confirmed.
Role behaviours
According to these results, if you invite clinical professionals to do teamwork under laboratory conditions, in situ workplace tribal and hierarchical behaviours are not readily replicated. Personal, rather than professional behaviour, dominates in the laboratory. There are grounds for believing, therefore, that stereotyping is an artefact of healthcare workplaces and history to a considerable degree.20 Put another way, in the workplace there are perceptions of marked behavioural patterns distinguishing doctors, nurses and allied health professionals.36–39 Our study suggests that these are not necessarily grounded in external reality, nor are they formed on the basis of demographic differences or personality; they simply do not manifest to any extent in controlled settings.
For an explanation, it might well be that when displaying a stethoscope or wearing a white coat, a nursing uniform, a physiotherapist's outfit or a technician's lab coat, this stimulates workplace participants to project stereotypic behaviours that they have assimilated through mechanisms such as workplace socialisation, professional education, or the perpetuation of role-anchored behaviours. It is important to remember that clinicians will tend to be more role oriented and profession centred (and even more Machiavellian and assertive) when in situ and their knowledge and status is involved. Take their artefacts away, and the context and culture might alter, often subtly, shifting towards more egalitarianism.
Implications for policy and practice
People in health workplaces treat the professions differently, and they behave according to established norms, tribal characteristics and in hierarchical and stereotypical ways. Indeed, ‘us’ and ‘them’ behaviours and attitudes pervade healthcare organisations. The results of this study suggest that for those wanting to promote greater levels of interprofessional teamwork in the real world, it is best not to reinforce these differences, but instead to attempt to inculcate a more equal, collaborative ethos and culture.
We are left with a view suggesting that hierarchical behaviours, tribalism and stereotypes may be a hangover from prior eras, rooted in past history when doctors were male and nurses and allied health professionals were female,29 ,30 or where historical in-group bonds were strongly based on group identification. Pronounced power disparities between the professions manifested from the earliest eras, and healthcare participants in situ seem to hold on to these despite large-scale shifts towards equality and horizontal responsibilities in society in recent years. Stereotypical, hierarchical and tribal behaviours, put simply, did not arise in our controlled conditions; they seem to be an artefact of workplaces rather than a manifestation of a priori personality or individual psychological differences. Strengthening interprofessional teamwork would, on the basis of this study, be enabled by paying more attention to the characteristics of the workforce context in which teams operate, and the encouraging of more egalitarian team activities, shared decision-making and mutual responsibilities.
Conclusion
Overall, traditionally patterned clinical workplace behaviours were rarely observed in a study with careful, triangulated measurements of team behaviours in external, controlled settings under a variety of tasks and conditions. It seems feasible to suggest that shaping workplace cultures by promoting interpersonal behaviours and taking steps to discourage professional tribalism are key to creating more heterogeneous teamwork, rather than looking for more deeply embedded sociological or psychological explanations rooted in the make-up of the individuals in these professions. Our data support the proposition that individual or group member characteristics are not the source of professional differences and cannot be used to predict subsequent poor cross-professional team orientation.
Strengths and limitations
Studies such as this cannot be completely randomised. Most psychology experiments enrol undergraduate students. A strength of this study was to include participants who held the actual in situ roles we sought to examine. Some people in the course or the conference from which the participants were drawn may have known each other, but we allocated people to groups randomly, so the effect is likely to be minimal. In addition, we used a teamwork rating scale that has been found to be effective for evaluating teamwork behaviours that improve patient safety. The populations from which participants were recruited were targeted towards people training to be leaders in healthcare, so the results might reflect their views rather than those of front-line staff, although, mitigating that, almost all were actually in front-line positions, either fully or partially. Nevertheless, we cannot rule out that stereotypes and in-group favouritism may have been more pervasive if participants were recruited from solely clinically focused roles. Owing to participants’ availability, some groups were not represented in some of the experimental tasks. Homogenous groups of doctors and allied health professionals in the healthcare budget allocation task, and homogeneous groups of doctors in the case study task, were less well represented. This meant that some comparisons could not be made across all professional groups for all tasks.
Acknowledgments
The authors give their thanks to Stephanie Dick (SD) and Jess Herkes (JH) for their support.
References
Footnotes
Contributors JB conceived of the study, did the initial design work and drafted the manuscript. RC-W, MW and JW worked the initial design in conjunction with JB into a final design. EV developed the laboratory and field materials. RC-W, DM, EV and TH (and SD) conducted the field work. BB reviewed and synthesised the digital video files. RC-W and MW executed various aspects of the statistical work. KL assisted with the analysis, literature reviews and the postdevelopmental editing of the manuscript. All authors read, commented on and approved the final version of the manuscript.
Funding No specific funding was allocated to this project. JB's work is supported by NHMRC Program Grant 1054146.
Competing interests None declared.
Ethics approval UNSW Human Research Ethics Committee (UNSW HREC/HC12040).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.