Article Text

Abstract
Introduction Adolescent idiopathic scoliosis (AIS) affects up to 3% of children around the world. There is limited knowledge of AIS aetiopathogenesis, and this evidence is needed to develop new management strategies. Paraspinal muscle in AIS demonstrates evidence of differential fibrosis based on curve sidedness. Fibrosis is the hallmark of macrophage-driven inflammation and tissue remodelling, yet the mechanisms of fibrosis in paraspinal muscle in AIS are poorly understood.
Objectives The primary objective of this study is to determine the influence of curve sidedness on paraspinal muscle inflammation. Secondary objectives include defining the mechanisms of macrophage homing to muscle, and determining muscle–macrophage crosstalk in muscle fibrosis in AIS.
Methods and analysis This is a cross-sectional study conducted in a tertiary paediatric centre in Hamilton, Ontario, Canada. We will recruit boys and girls, 10–17 years of age, who are having surgery to correct AIS. We will exclude children who have an active infection or are on immunosuppressive therapies within 2 weeks of surgery, smokers and pregnant girls. Paraspinal muscle biopsies will be obtained at the start of surgery. Also, blood and urine samples will be collected from participants, who will fill questionnaires about their lifestyle. Anthropometric measures will also be collected including height, weight, waist and hip circumferences.
Ethics and dissemination This study has received ethics authorisation by the institutional review board. This work will be published in peer-reviewed journals and will be presented in oral and poster formats at scientific meetings.
Discussion This study will explore the mechanisms of paraspinal muscle inflammation, remodelling and fibrosis in AIS. This will help identify pathways and molecules as potential therapeutic targets to treat and prevent AIS. It may also yield markers that predict scoliosis progression and response to treatment in these children.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to determine the mechanisms of inflammation and its effect of paraspinal muscle remodelling and fibrosis in AIS.
This study will also shed light on immune cell phenotype differences in paraspinal muscle on both sides of the scoliotic curve, and how this then drives immune–muscle crosstalk in AIS.
Owing to the cross-sectional nature of the study, it will not be possible to determine immune cell phenotype in muscle is a cause or effect of spinal curving.
As samples are collected at the maximal points of convexity and concavity, potential changes in other parts of the paraspinal muscle will not be studied.
Introduction
Idiopathic scoliosis is a three-dimensional deformity of the spine that occurs in up to 3% of children globally.1 Adolescent idiopathic scoliosis (AIS) is the most common form1 ,2 and in 80% of cases occurs in girls.3
AIS has potential implications for health across the lifespan, including pain, mobility problems, pulmonary hypertension and psychological health issues. While some of these complications have beens inconsistently reported, their occurrence places a heavy burden on the child, and some do not improve with treatment.4–6 It is a challenge to predict which child will develop AIS, and who is at risk of curve progression, which limits the development of precise therapies. The potential risk factors for progression of the scoliotic curve include curves with Cobb angle ≥30°, pubertal growth spurt, premenarchal girls, a right thoracic curve in girls and left lumbar curve in boys.1 ,7
Current treatment options depend on the severity of the scoliotic curve. In patients who are still growing with a Cobb angle <25°, observation is the mainstay of therapy. In cases with significant curvature (Cobb angle 25–40°) or with worsening of the curve, patients may require bracing to help control progression, but this does not reduce the severity of the curve.8–13 In those who have completed growth or are still growing with significant curves (Cobb angle 45° or higher), surgery is often undertaken to halt curve progression and induce partial correction.14–18 Bracing and surgical complications, although rare, are significant especially neurological complications in combined anterior and posterior surgical procedures.19 ,20
The mechanisms driving the initiation and propagation of the scoliotic curves are incompletely understood, and there is a paucity of models that can improve insights into the genesis of AIS. Animal models do not have the same spinal architecture of humans. Some models rely on chemical induction of scoliosis, so the faithful replication of aetiopathogenesis of AIS in these models is not possible.21 ,22 The prevalence of AIS, potential comorbidities, treatment-related complications, the lack of a unifying mechanism and the dearth of models to provide mechanistic insights into AIS occurrence make this disease a significant challenge to solve. Understanding the aetiopathogenesis of AIS continues to rely on studying humans as the best model of their disease.
Defining the mechanisms driving AIS will help the development of precise diagnostic, therapeutic and prevention strategies, which will likely improve outcomes.
Potential mechanisms driving AIS aetiopathogenesis: It is clear that AIS is a polygenic disease with genetic, epigenetic, nervous system, hormonal/metabolic, biochemical, musculoskeletal, environmental and possible lifestyle factors contributing to its genesis.23 ,24 Regardless of its cause, abnormalities of vertebral growth plates are a final destination for many proposed mechanisms that drive AIS. Still, there are many unanswered questions regarding the mechanisms involved in the development and progression of AIS.
Genetic factors: AIS is more common in families with a history of the disease, but there is no definite mode of inheritance. The main hurdles to identifying genes of AIS pathogenesis are the heterogeneity of genotypic and phenotypic definitions of cases, and relatively small sample sizes included in genetic studies.25
It is likely that many genes of minor effect contribute to the development of AIS. Twin studies have been inconsistent in showing increased concordance in monozygotic and dizygotic twins.26–30 This inconsistency suggests that other factors, including environmental and epigenetic elements, contribute to AIS with a given genetic background.
Gene linkage studies suggest that genetic factors influence the development of AIS, with loci so far on chromosomes 1, 3, 5, 6, 7, 8, 9, 11, 12, 16, 17, 18 and 19.25 ,29 ,31 ,32
Several candidate genes have been linked to AIS, but confirmation of these associations remains inconsistent and requires larger replication studies.33–42 A two-phase model for the development of AIS has been proposed. Under this model, a set of genetic factors initiate the development of the curve, while another set determines curve progression. These sets of genes may overlap in their effects and may be influenced by the environment.43
Importantly, genome-wide association studies (GWAS) have implicated new genes, with one study creating a list of markers that are predictive of curve progression.44
A recent GWAS reported the association of a gene expressed in the dorsal spinal cord, skeletal muscle and somatosensory neurons with AIS. Ladybird homeobox 1 (LBX1) is involved in muscle precursor and neuronal cell development and migration.45–47
A microduplication of the genomic region where LBX1 gene resides (10q24.31) was associated with scoliosis and myopathy.48 Further studies are needed to explore the mechanistic details of the role of LBX1 in AIS.
Epigenetics: Epigenetics refer to the phenomenon of production of different phenotypes due to changes in the expression of a gene rather than its sequence.49 Epigenetics is one of the mechanisms driving many non-communicable diseases due to exposure to an adverse intrauterine environment,50 but the role of epigenetics in AIS requires further study.23
Environmental and lifestyle factors: Sporadic reports link low body mass index (BMI) and diet (eg, calcium intake) with the prevalence of AIS. Inadequate calcium intake during the peripubertal period might result in poor bone mineralisation with accelerated bone growth.51–54
There is controversy as to whether girls with AIS have different body composition compared with girls with no AIS. Some studies have reported that BMI and fat mass are lower in AIS, but this has not been a consistent finding.52–54 The differences in BMI and adiposity may affect spinal development and skeletal maturation, and their role in AIS is unknown. Also, lower physical activity has been studied as an association of AIS, and the speculation is that this is related to a proprioception defect.51 Later age of menarche has been associated with more risk of AIS, and the risk is reduced for those who live closer to the equator.55 Systematic studies of the role of environmental factors in AIS are needed.
The nervous system: As patients with several neurological syndromes have scoliosis, there has been significant focus on defining neurological factors contributing to AIS.56–58 In addition, defects in central control and processing of information have been proposed to be associated with AIS, although their role in the development and propagation of AIS remains under investigation.
Anatomical abnormalities involving spine, midbrain, pons, medulla, vestibular and hindbrain regions have been reported in AIS.59–61 Differences in brain volume, internal capsule and corpus callosum were also reported.62–64 How these differences drive AIS is a mystery.
Neurophysiological mechanisms have also been reported in AIS, including abnormal proprioception, oculovestibular dysfunction, lateral gaze palsy, dynamic balance problems, postural imbalance and somatosensory disequilibrium.65–70 There have also been reports of enhanced electromyographic activity of the convex side of the spine.71
These phenomena led to the hypothesis that a combination of abnormal spinal growth patterns and neuromuscular and tissue remodelling is implicated in AIS.72 Posture is determined by sensory input from visual, vestibular and proprioception neural pathways, coupled with motor output. As a first step, postural disequilibrium due to defects in the neuromuscular system leads to the development of small spinal curves. With ongoing spinal growth, a second step involves biomechanical and neurological factors that drive the progression of the curve.72 With the establishment of scoliosis, secondary geometric and morphological changes emerge.73–75
Hormones and metabolic dysfunction: Studies have produced mixed results on the association of several biomarkers, their receptors and gene variants with AIS. Some of the data have suggested that growth hormone (GH),76 ,77 calmodulin,78 melatonin42 ,78–83 and leptin84 ,86 may have a role in AIS.
Melatonin deficiency, triggered by pinealectomy, was shown to cause scoliosis,87–89 and melatonin levels were reported to be reduced in patients with AIS.90 Both findings were not replicated in other studies that used pinealectomy or light stimulation to suppress melatonin in different models, including primates.83 ,91 ,92 One study suggested impairment in the melatonin signalling pathway in primary osteoblasts from patients with AIS.93 It has been proposed that initial spinal imbalance is sustained by biochemical, postural and melatonin signalling pathways that contribute to the development of scoliosis.94 Further research is needed to define the potential role of melatonin in AIS.
Calmodulin is a regulator of contractile properties of muscle, and its increased levels may lead to altered paraspinal muscle activity and progression of the scoliotic curve. This hypothesis is supported by the fact that calmodulin is asymmetrically distributed across the paraspinal muscles of patients with AIS.78
Leptin has also been implicated in the genesis of AIS.84 ,86 The ‘leptin-hypothalamic-sympathetic nervous system theory’ proposes that asymmetrical hypothalamic upregulation of leptin signalling leads to an asymmetrical activation of the sympathetic nervous system that may be associated with upregulation of GH/insulin-like growth factor 1 (IGF-1) axis.95
Since the sympathetic nervous system regulates the growth of the axial skeleton, the resulting asymmetrical vertebral growth plates may affect the progression of AIS, while the somatic nervous system may be involved in the initiation of the curve by the failure of mechanisms that maintain posture.95 ,98
Biomechanical factors: The human spine has natural kyphotic curves at thoracic and sacral regions, and lordotic curves at cervical and lumbar regions. One consistent anomaly in AIS is the shape abnormality in the sagittal plane.99 A large study that evaluated children for scoliosis demonstrated that lordosis was always present prior to the development of thoracic AIS.100 One potential hypothesis that may explain the progression of the spinal curve in AIS is that patients with AIS are taller than controls, and this is coupled with the fact that girls have more slender spines than boys.99 This makes the spine in girls more likely to buckle under force, and this is maximised during periods of rapid spinal growth including puberty. Increased compression force on the concave side may reduce spinal growth, while reduced loading on the convex side may accelerate growth.99 ,101 Another important study that evaluated cadaveric idiopathic scoliosis demonstrated that the primary abnormality is lordosis with anterior vertebral wedging. This leads to biomechanical instability, and compensatory rotation and scoliosis.102
Paraspinal muscle metabolism in AIS
The fibre composition of paraspinal muscle in AIS has been studied, and while the results are inconsistent, the prevailing view is that type I fibres are more prevalent on convex side of the curve. Type II fibres are increased or reduced on the concave side, but they were increased on the convex side in one study.103–109
Other abnormalities noted in muscle include increased intracellular calcium, reduced zinc,109 increased glucocorticoid receptors on the convex side,111 reduced RNA activity on the concave side and increased protein synthesis on the convex side.112 Muscle enzymes seem equal with minor exceptions.113
Skeletal muscle–immune crosstalk: a novel paradigm in potential pathogenesis of AIS
While the literature hints at muscle phenotype as a secondary phenomenon in scoliosis, it is a difficult conclusion to establish.
One important consideration is that the diagnosis of AIS is taken to be the time of presentation. However, scoliosis would have evolved over an undefined period before the diagnosis, making longitudinal studies starting at inception a challenge. Therefore, muscle phenotype may drive or be driven by scoliosis. In addition, it is not feasible to obtain repeated muscle biopsies to assess muscle changes in scoliosis, as this is an invasive procedure.
All studies that have examined muscle pathology in AIS have done so in a cross-sectional fashion due to these limitations.22 ,114 ,115 Animal models used to study this disease have relied on surgically or chemically induced scoliosis, which may not faithfully recapitulate the events in patients and requires specific expertise especially when using big animals (eg, chicken).114
Recent evidence suggests that while paraspinal muscle on both sides of the spinal curve has increased fibrosis, muscle on the concave side of the spine demonstrated more enhanced fibrosis and fatty involution compared with that on the concave side.115 These findings were taken to suggest a myopathic process based on finding central core lesions in muscle. Importantly, fibrosis is the hallmark of immune cell–tissue interaction to remodel tissues and restore homeostasis.116 ,117
Innate immunity and fibrosis in AIS
The innate immune system is the initial line of defence against environmental threats.118 Components of the innate immune system include cells (monocytes, neutrophils, basophils, eosinophils, natural killer cells, dendritic cells, and mast cells) and receptors including nucleotide-binding oligomerisation domain (NOD) proteins and Toll-like receptors (TLRs) and complement proteins.119–121 While acute activation in muscle injury results in a controlled remodelling response mediated by neutrophils and macrophages, chronic activation and low-grade inflammation can lead to dysregulation of tissue remodelling and fibrosis.116 ,122
Circulating monocytes are attracted to different tissues in response to chemokines. Monocytes sense the muscle microenvironment and, guided by tissue cues, differentiate to macrophages.123 There are two main types of macrophages. Inflammatory or M1 macrophages originate from bone marrow-derived monocytes that enter the injured tissue, and produce pro-inflammatory cytokines and are detected in muscle.124 Resident or M2 macrophages are present in tissues under physiological conditions and help with tissue homeostasis and remodelling.125 The imbalance between anti-inflammatory actions of M2 and inflammatory responses by M1 macrophages is a fundamental driver of the effects of inflammation on muscle phenotype. This M1 and M2 paradigm is a rather simplistic view of macrophage phenotype, and there are several intermediate phenotypes driven by tissue demands.126 ,127 One possibility is that in AIS, muscle inflammation is an acute-on-chronic process, whereby repeated cycles of tissue injury related to the progression of the scoliotic curve may lead to concomitant inflammation and fibrosis. This is supported by paraspinal muscles demonstration of simultaneous atrophy and hypertrophy, indicating that there is ongoing activity to remodel muscle.115 Muscle tissue injury may be the primary initiating event or the result of spinal curvature.
Recent evidence has strengthened the role of macrophages in muscle fibrosis in a chronic muscle disease, Duchenne muscular dystrophy.128 Acute muscle injury is characterised by three important responses: (1) expansion of satellite cells (muscle stem cells), (2) infiltration of inflammatory M1 macrophages and (3) expansion of resident mesenchymal cells (fibro/adipogenic progenitor cells, FAPs). The latter two mechanisms regulate myogenesis, whereby the expansion of FAPs in acute injury is followed by an apoptotic response to regulate FAP mass; tumour necrosis factor α (TNFα), a prototypical inflammatory cytokine, is secreted by infiltrating inflammatory macrophages and drives this response. This allows limited FAP expansion and regulates tissue remodelling to restore normal tissue function.128
On the other hand, chronic or repeated muscle injury (which may be a primary or secondary event in AIS) triggers a tissue repair response. This response is characterised by expansion of progeneration (M2) macrophages, activation of FAPs and the production by M2 macrophages of transforming growth factor β1 (TGFβ1), which inhibits TNFα and allows FAP expansion. This is associated with enhanced fibrosis and extracellular matrix deposition in muscle.128 Therefore, the shift from pro-myogenic to pro-fibrotic muscle response is driven by macrophage population differences; whether this translates to AIS is unclear.
In addition, other innate and adaptive immune cells are likely to play a role in muscle Immunometabolism, but limited data exist as to their role in AIS.
Immune cells and the chemokine(s) that attract them to paraspinal muscle in AIS have not been studied. However, they may contribute to the initiation or propagation (or both) of the spinal curve in AIS by influencing muscle remodelling. In addition, muscle–bone–cartilage–disc–immune crosstalk at the interphase of these tissues is critically important to tissue metabolism and health129 but has not been studied in AIS. Understanding the role of the immune system in muscle inflammation, metabolism and fibrosis in AIS is the objective of the proposed study.
The role of skeletal muscle inflammation and fibrosis in the causation of AIS is not completely understood. It is imperative to delineate the role of immune cells in muscle in AIS, as this may help define targeted therapies to muscle immune cells, and define biomarkers of scoliosis initiation, progression and response to therapy.
The Immunometabolic CONnections to Scoliosis (ICONS) study was designed to investigate paraspinal muscle–immune crosstalk in AIS, and is focused primarily on understanding the role of the macrophage in AIS.
Research question
In adolescents with AIS, does paraspinal muscle on the concave side of the scoliotic curve, compared with paraspinal muscle on the convex side, have enhanced anti-inflammatory macrophage infiltration? If so, is this associated with FAP expansion and fibrosis?
Objectives
Primary: To quantify macrophages and muscle inflammation in paraspinal muscle from concave and convex sides of the scoliotic curve.
Secondary:
Profile chemokines in paraspinal muscle from concave and convex sides of the scoliotic curve.
Assess the role of FAP in muscle fibrosis in AIS.
Hypothesis: In adolescents with AIS, enhanced anti-inflammatory macrophage infiltration of paraspinal muscle on the concave side, compared with the convex side of the curve, drives FAP expansion and differential fibrosis.
Methods and study procedures
Study design
This is a cross-sectional study. The participants will be recruited from Pediatric Orthopedic clinical services at McMaster Children's Hospital, a tertiary paediatric care centre in Hamilton, Ontario, Canada. The study procedures are described in figure 1.
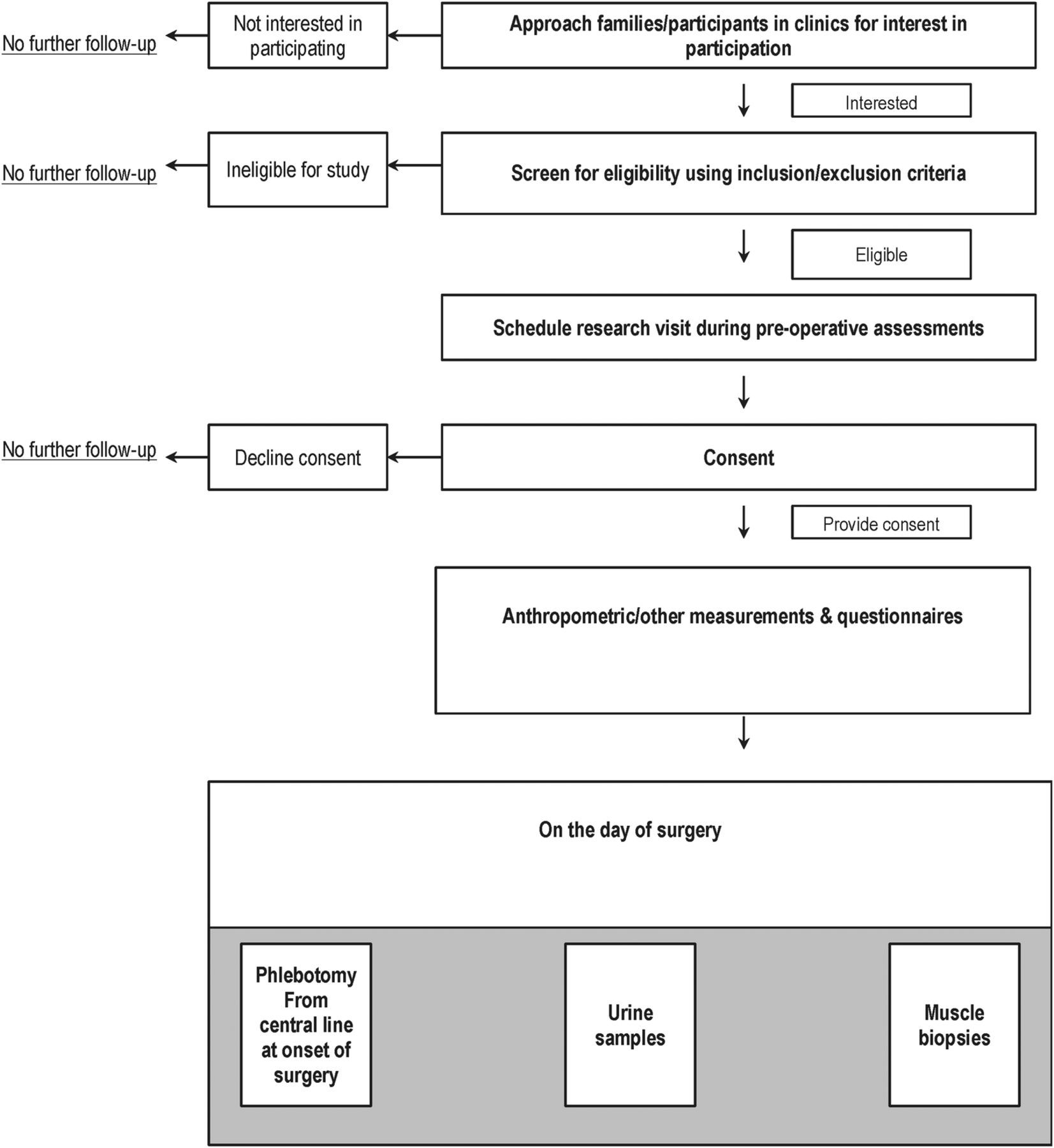
ICONS study flow diagram. ICONS, Immunometabolic CONnections to Scoliosis study.
Cohort characteristics
Inclusion criteria: We will include boys and girls, 10–17 years of age with a diagnosis of AIS confirmed on clinical and radiological grounds, and who have been informed by their team that they require and have agreed to undergo spinal surgery. We will include lean (BMI centile below 85th) and overweight/obese (BMI centile ≥85th) who are free from infection for 15 days before sample collection.
Exclusion criteria: We will exclude patients with scoliosis related to other causes, including congenital scoliosis, neuromuscular disorders, metabolic disorders, skeletal dysplasia and syndromes. We will also exclude those on certain medications used within 15 days prior to sample collection (including high-dose steroids, immunosuppressive therapy and anti-thrombotic medications). We will also exclude those with active bacterial, viral or fungal infections, and chronic inflammatory diseases including autoimmune disease (systemic lupus erythematosus, juvenile idiopathic arthritis, dermatomyositis). We will also exclude smokers, pregnant girls and those who are unable or unwilling to provide consent.
Recruitment and consents
The ICONS study will recruit patients who have been deemed eligible for scoliosis surgery. The healthcare provider will ask permission from potential participants to be approached by the study team. If patients and parents agree, the study team will meet the participants on the day of their preoperative evaluation to introduce the study and answer questions.
If the family and participant agree to participate, consent forms will be signed. The consent forms include those for parents and assent forms for children aged between 10 and 15 years. For those aged 16 years or older, the participants will sign their consents. Separate consent forms for genetic (DNA) testing are completed. The participants are assigned unique identifying numbers to protect confidentiality and data are anonymised shortly after collection.
Questionnaires
After consent procedures are completed, study questionnaires are provided to the participants and their families.
The study will collect sociodemographic and clinical data including age, gender, grade in school, parental education, religion, ethnicity, history of medical or surgical problems, birth history, family income, social history and family history of medical problems.
Regarding dietary information, the intake of different food items will be documented using a dietary questionnaire modified from the Adolescent Food Frequency Questionnaire.130 ,132 Reported physical activity will be measured using the Habitual Activity Estimation Scale (HAES) Questionnaire.133 Sleep will be measured using the Chevrin Sleep Questionnaire.134 We will also enquire about mental health by asking participants or parents to fill a questionnaire reporting mental health problems.135 Neighbourhood walkability will be determined using the Neighborhood Environment Walkability Scale (NEWS) Questionnaire.136
Anthropometric and clinical measurements
The participants will have their height measured closest to 0.1 cm using a stadiometer, weight to closest 0.1 kg using weighing scale, and BMI in kg/m2 will be calculated from height and weight and BMI centile determined from Centers for Disease Control (CDC) growth charts. The waist circumference and hip circumference will be measured using a spring-loaded measuring tape closest to 0.1 cm. Puberty will be assessed using drawings describing Tanner staging for girls 8 years or older, and external genitalia for boys 9 years and older.137
Sitting systolic and diastolic blood pressure (BP) will be measured using automated BP monitor, and pulse rate is measured using the same device. Body fat percentage is measured using Tanita body fat monitor for children (Tanita Corporation, Illinois, USA), and grip strength will be tested using a dynamometer.
Biological samples
All samples will be obtained on the day of surgery after an overnight fast of 8–10 hours.
Blood
Blood samples are obtained after patients are anaesthetised and central lines are in place to permit blood sampling. We will be collecting serum and plasma samples as well as buffy coat for DNA studies. PAX RNA whole blood samples are also collected for RNA studies. Samples will be aliquoted to cryovials and stored at −80°C until further use.
Urine
Urine samples will be obtained using 90 mL urine containers after urinary catheterisation for the surgical procedure. Urine is aliquoted to cryovials and stored at −80°C until further use.
Tissue sampling and processing
Paraspinal muscle (erector spinae) samples will be collected shortly after starting the surgical procedure for correction of scoliosis. The points of sampling include samples from the apex (maximal area of convexity) of the spinal curve, matched with a biopsy from the area of maximal concavity on the opposite side of the spinal curve.
Two important procedures are applied during sample collection that will ensure fidelity of immune cell phenotype. First, we will collect the samples before epinephrine injections, used to control bleeding during surgery, as it is known that adrenergic stimuli may change macrophage responses. We will also avoid cauterised areas for tissue sampling.
The muscle samples will be cleaned from blood by drying with gauze, and connective tissue is separated from samples. Tissue samples are then divided into five pieces, and four pieces will be snap frozen immediately in liquid nitrogen and transferred to −80°C freezer for storage. One piece will be formalin fixed and paraffin embedded until further processing.
Experimental work details
Primary objective: determine the influence of curve sidedness on paraspinal muscle inflammation
Muscle macrophage content will be profiled using CD68 quantitative real-time PCR (qRT-PCR), western blot and immunohistochemistry (IHC).124 ,138
For qRT-PCR, muscle tissue (25–50 mg) will be chipped and powdered, and then added to Trizol reagent. The tissue will be homogenised, and RNA isolation will take place using RNeasy Mini Kit (Qiagen).
In total, 1 μg of RNA will be used to generate complementary DNA (cDNA) using SuperScript III Reverse Transcriptase Kit (Invitrogen, Carlsbad, California, USA). qRT-PCR will be completed using TaqMan assay primer/probe mixes (Applied Biosystems) as we previously described.124 ,139 Western blot and IHC will be performed as described previously by our group.124 ,138 ,139
The full characterisation of macrophage phenotype will be determined by testing markers of inflammatory macrophages, including cluster of differentiation-11c (CD11c), arginase II and C-C chemokine receptor 2 (CCR2). Anti-inflammatory macrophages will be detected by using CD206, TGFβ1 and CD301 using qRT-PCR, western blot and IHC co-staining methods.140 We will use Nikon Eclipse 90i microscope for imaging, and analyse images to determine macrophage content using NIS Elements 64 bit 3.22.11 software (Nikon Inc, Melville, NY, USA).138 ,141
To profile muscle inflammation, we will perform qRT-PCR using TaqMan assay primer/probe mixes (Applied Biosystems) on cDNA synthesised from RNA from muscle.
We will test the gene expression of pro-inflammatory cytokines including TNFα, interleukin 1β (IL-1β), IL-6 and interferon γ (IFNγ). Anti-inflammatory cytokines measured include IL-10 and IL-1 receptor antagonist (IL-1Ra).
We will also measure cytokines in lysates from muscle (TNFα, IL-1β, IL-6, IFNγ, IL-10, IL-1Ra) using Bio-Plex assays (Bio-Rad) as we previously reported.138
Activation of inflammatory pathways responsible for cytokine and chemokine production will be tested using western blot, including c-Jun-N-terminal kinase (JNK), extracellular signal-regulated kinase (ERK), p38 mitogen-activated protein kinase (p38MAPK) and nuclear factor κB (NFκB) pathways (cell signalling).139
Total and phosphorylated (activated) versions of the molecules will be quantified and reported as a ratio of phosphorylated/total protein. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) will be used as a loading control.139
Secondary objectives
Profile chemokines in paraspinal muscle from concave and convex sides of the scoliotic curve
As chemokines drive macrophage migration to muscle, there is a need to determine the chemokines driving macrophage infiltration to muscle in AIS. We will assess the gene expression of CCL2, CCL3, CCL5, macrophage colony-stimulating factor (M-CSF), granulocyte–monocyte colony-stimulating factor (GM-CSF), and chemokine (C-C) ligand 20 (CCL20), which accounts for most muscle chemokinetic activity.
Chemokine protein content (CCL2, CCL3, CCL5, MCSF, GM-CSF, CCL20) will be assessed using Bio-Plex assays (Bio-Rad) as we previously reported.138
Assess the role of FAP in muscle fibrosis in AIS
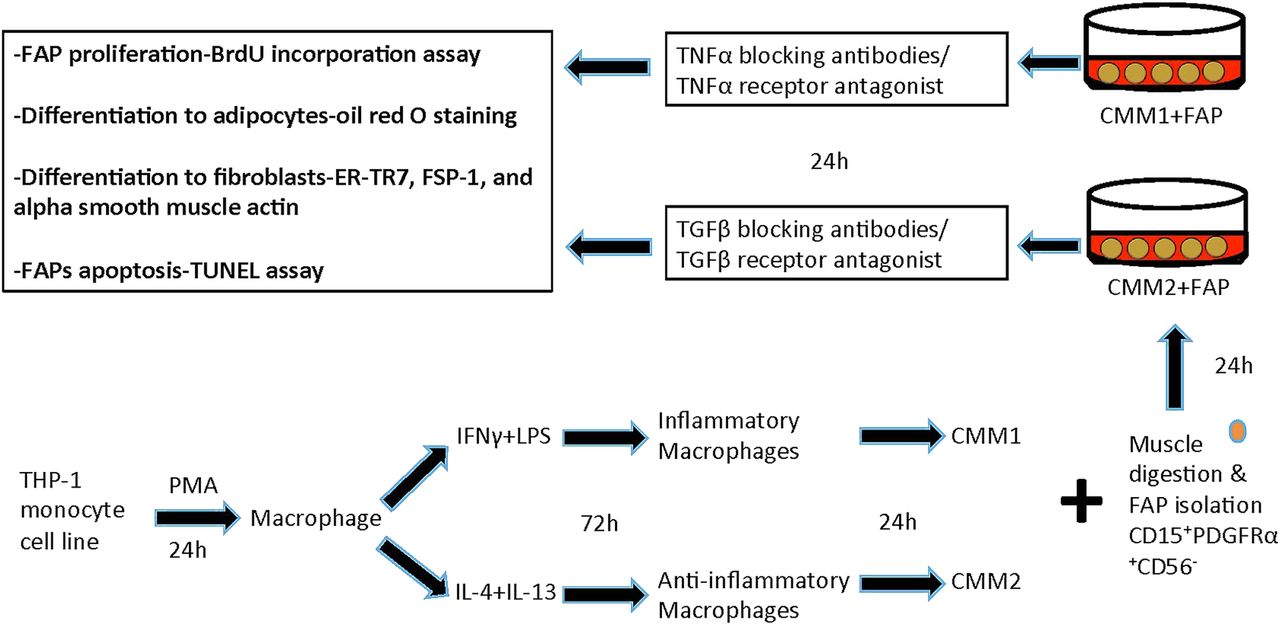
The experimental design of this part is described in figure 2. We will generate macrophages and evaluate inflammatory (M1) and anti-inflammatory (M2) effects on FAPs. We will isolate FAPs from paraspinal muscle using CD15+PDGFRα+CD56− markers after collagenase digestion by flow cytometry.142
{kind=link}
{kind=link}
Testing macrophage–muscle crosstalk in adolescent idiopathic scoliosis (AIS). THP-1 monocyte cell line is treated with 150 nM phorbol 12-myristate 13-acetate (PMA) for 24 hours to generate macrophages. Macrophages are treated with 20 ng/mL interferon γ (IFNγ)+10 pg/mL lipopolysaccharide (LPS) to generate inflammatory macrophages, and 20 ng/mL interleukin 4 (IL-4)+20 ng/mL IL-13 to generate anti-inflammatory macrophages. The medium the cells are growing in is called conditioned medium (CM) for inflammatory (CMM1) and anti-inflammatory (CMM2) macrophages. To generate fibro/adipogenic progenitors (FAPs), muscle will be digested with collagenase, and FAPs will be plated into 12 well plates. We will then add CMM1 and CMM2 to FAPs, and then test FAP proliferation, differentiation to adipocytes and fibroblasts, and apoptosis. BrdU, bromodeoxyuridine; FSP-1, fibroblast-specific protein 1; TGFβ, transforming growth factor β; TNFα, tumour necrosis factor α; TUNEL, terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick-end labelling.
To generate macrophages, we will differentiate THP-1 human monocyte cell line to macrophages (24-hour incubation with 150 nM phorbol 12-myristate 13-acetate (PMA), followed by 24-hour incubation in Roswell Park Memorial Institute (RPMI) medium). Macrophages will then be polarised to M1 macrophages (20 ng/mL IFNγ+10 pg/mL lipopolysaccharide (LPS)). Polarisation to M2 will be done by incubating cells in 20 ng/mL IL-4+20 ng/mL IL-13).143 We will collect the medium in which M1 and M2 cells are growing in. This conditioned medium from M1 (CMM1) and M2 (CMM2) will be used in this set of experiments. To determine if inflammatory (M1) macrophages produce factors that reduce FAP proliferation and differentiation, we will treat FAPs with CMM1 for 24 hours. We will then measure FAP proliferation with bromodeoxyuridine (BrdU) incorporation assay, differentiation to adipocytes using oil red O staining and differentiation to fibroblasts using gene expression and western blot of ER-TR7, fibroblast-specific protein 1 (FSP-1) and α smooth muscle actin. We will also test FAPs for apoptosis by performing terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick-end labeling (TUNEL) assay using TiterTACS in situ kits (R&D Systems). We will then measure CMM1 cytokines including TNFα using ELISA, and use TNFα neutraliser adalimumab, and repeat the FAP treatment.144 In addition, we will treat FAPs with TNFα receptor antagonist (R-7050; Santa Cruz)145 and repeat the experiments.
To determine if anti-inflammatory (M2) macrophages produce factors that enhance FAP proliferation and differentiation, we will treat FAPs with CMM2 for 24 hours. We will then measure FAP proliferation with BrdU incorporation assay, differentiation to adipocytes using oil red O staining and differentiation to fibroblasts using gene expression and western blot of ER-TR7, FSP-1 and α smooth muscle actin, and apoptosis by performing TUNEL assay. We will then measure CMM2 cytokines including TGFβ, and then use TGFβ neutralising antibodies and test FAP proliferation and differentiation. We will also treat FAPs with TGFβ receptor antagonist (LY2157299; Eli Lilly),146 and repeat the FAP treatment with CMM2.
Statistical analysis
Outcome variables will be summarised using descriptive summary measures expressed as mean (SD) or median (minimum–maximum) for continuous variables, and number (%) for categorical variables. Data will be checked for normality using Kolmogorov-Smirnov test, and log transformed if not normally distributed. We will test differences in sociodemographic and clinical data between groups using χ2 tests for categorical variables and t-test or Kruskal-Wallis tests for continuous variables depending on the distribution. Statistical analysis of qRT-PCR experiments will be done using ΔΔCT.124 For ELISA, standard curves will be generated and cytokines normalised to total protein content of the sample and reported as pg/μL/μg protein.138 For western blots, we will measure the total and phosphorylated protein and generate a ratio of total/phosphoprotein for comparisons.139
For IHC, macrophages will be counted manually at ×400 magnification, and the number of macrophages is normalised to the section area. The researcher counting the cells will be blinded to the experimental group allocations as we previously reported.138
For human samples, all analyses will be performed using regression analyses to pool and compare the groups adjusted for age, sex, BMI, ethnicity and fitness. For in vitro studies, data will be analysed using t-test.
The results will be reported as estimates of the difference, corresponding 95% CIs and associated p values. Alpha is set at 0.05, adjusted using Bonferroni approach for multiple analyses. All analyses will be performed using SAS 9.2 (Cary, North Carolina, USA).
Sample size: For sample size calculations for the full study, as macrophage phenotype evaluation in paraspinal muscle has not been done in AIS before, power calculation is difficult. We aim to recruit 120 patients based on sample size calculations according to Norman and Streiner,147 whereby 10 patients are needed per marker studied. We plan to approach 200 patients, and assuming 80% recruitment rate, and 20% attrition, with one patient being evaluated weekly for surgery and 40 scoliosis surgeries per year at our institution, we plan to complete patient recruitment over 60 months for the full study.
Discussion
Previous research has demonstrated the presence of fibrosis in paraspinal muscle in AIS.115 The immune system is one of the major players in muscle tissue remodelling via inflammation, yet this has not been fully studied in AIS.
This work will focus on understanding the mechanisms driving immune–muscle crosstalk in AIS, and the contribution of FAPs to muscle fibrosis. This work will aid the development of anti-inflammatory and antifibrotic therapies to help retain muscle strength, reduce pain and delay or prevent the development of the scoliotic curve. This study may also reveal muscle-specific biomarkers that predict initiation and progression of the scoliotic curve, response to therapy or the development of complications.
References
Footnotes
Contributors MCS conceived the study question. MCS, PM and DP designed the study objectives and developed the study procedures. LT provided methodological and statistical support. MCS drafted the first version of the manuscript; and all authors read, provided comments and approved the final draft.
Competing interests None declared.
Ethics approval Hamilton Integrated Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.