Article Text

Abstract
Introduction Sleepiness is a cardinal symptom in obstructive sleep apnoea (OSA) but most patients have unspecific symptoms. Arterial stiffness, evaluated by pulse wave velocity (PWV), is related to atherosclerosis and cardiovascular (CV) risk. Arterial stiffness was reported to be higher in patients with OSA, improving after treatment with continuous positive airway pressure (CPAP). This study aims to assess whether the same effect occurs in patients with OSA and without sleepiness.
Methods and analysis This observational study assesses the CV effect of CPAP therapy on a cohort of patients with moderate-to-severe OSA; the effect on the subcohorts of sleepy and non-sleepy patients will be compared. A systematic and consecutive sample of patients advised CPAP therapy will be recruited from a single outpatient sleep clinic (Centro Hospitalar de Lisboa Central—CHLC, Portugal). Eligible patients are male, younger than 65 years, with confirmed moderate-to-severe OSA and apnoea–hypopnea index (AHI) above 15/hour. Other sleep disorders, diabetes or any CV disease other than hypertension are exclusion criteria. Clinical evaluation at baseline includes Epworth Sleepiness Scale (ESS), and sleepiness is defined as ESS above 10. OSA will be confirmed by polygraphic study (cardiorespiratory, level 3). Participants are advised to undertake an assessment of carotid-femoral PWV (cf-PWV) and 24 hours evaluation of ambulatory blood pressure monitoring (ABPM), at baseline and after 4 months of CPAP therapy. Compliance and effectiveness of CPAP will be assessed. The main outcome is the variation of cf-PWV over time.
Ethics and dissemination This protocol was approved by the Ethics Committees of CHLC (reference number 84/2012) and NOVA Medical School (number36/2014/CEFCM), Lisbon. Informed, written consent will be obtained. Its results will be presented at conferences and published in peer-reviewed journals.
Trial registration number NCT02273089; Pre-results.
- Obstructive sleep apnea
- Sleepiness
- Pulse wave velocity
- Arterial stiffness
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study allows us to obtain new evidence on the effectiveness of continuous positive airway pressure (CPAP) in decreasing cardiovascular risk in sleepy and non-sleepy male patients with obstructive sleep apnoea (OSA).
The strengths of this protocol are a controlled and clinic-based setting, the use of standardised instruments to characterise OSA and sleepiness and the use of standardised quantitative early indicators of cardiovascular risk (carotid-femoral pulse wave velocity, cf-PWV).
This observational study has the limitations of convenience, non-randomised sample and the exclusion of patients with mild OSA or older patients.
Background
Obstructive sleep apnoea (OSA), if left untreated, is associated with high cardiovascular (CV) morbidity and mortality.1–3
The diagnosis of OSA syndrome is based on the presence of symptoms suggestive of the disorder, with confirmation by polygraphic sleep study.4 ,5 The Epworth Sleepiness Scale (ESS) is a validated questionnaire that evaluates the presence of excessive daytime somnolence.6 Other symptoms besides sleepiness are non-specific (decreased concentration, irritability),4 ,5 hampering diagnosis.
Continuous positive airway pressure (CPAP) is the standard therapy for patients with symptomatic OSA, but CPAP therapy for asymptomatic patients is consensual only when the apnoea–hypopnea index (AHI) is above 30/hour.7
In some studies, greater severity in polysomnographic parameters has been reported in sleepy patients in comparison with those who are not sleepy.8 ,9
Considering the relationship between OSA and CV disease, namely arterial hypertension or CV risk, it is less evident in patients with fewer symptoms. The effect of CPAP in lowering the blood pressure (BP) levels seems greater in patients with more severe OSA and sleepiness than in those without it.10
Changes in arterial stiffness are measurable and are one of the earliest manifestations of functional and structural damage to the vessel wall in the process of atherosclerosis. Arterial stiffness, evaluated by pulse wave velocity (PWV), is used as an early marker of organ damage in patients with hypertension.11 It predicts CV events, beyond classical CV risk factors, and can be considered as an intermediate end point for CV events.12 Carotid-femoral PWV (cf-PWV), that is, the speed of the pulse as it travels from the heart to the carotid and the femoral artery, is the most commonly used non-invasive method to assess arterial stiffness and is considered to be the gold standard.12 ,13
Increased arterial stiffness depends on various conditions, of which BP and ageing prevail, but also depends on other CV risk factors.
cf-PWV value is augmented in patients with OSA, and even in those without high BP.14 ,15 It is increased even in the less symptomatic, severe patients. However, there is an improvement after treatment with CPAP,16 but the effect in patients without sleepiness is less well known and still controversial.17
This research protocol aims to assess the variation of arterial stiffness in two cohorts of patients with OSA, either sleepy or non-sleepy, while undergoing treatment with CPAP. We hypothesise that a measurable improvement on cf-PWV can be detected over time, independent of sleepiness.
Methods and analysis
Study design
This project involves the prospective and observational study of a systematic, consecutive and non-randomised sample of adult male patients diagnosed with OSA and advised CPAP therapy, recruited from a single outpatient sleep clinic (Centro Hospitalar de Lisboa Central—CHLC, Lisbon, Portugal).
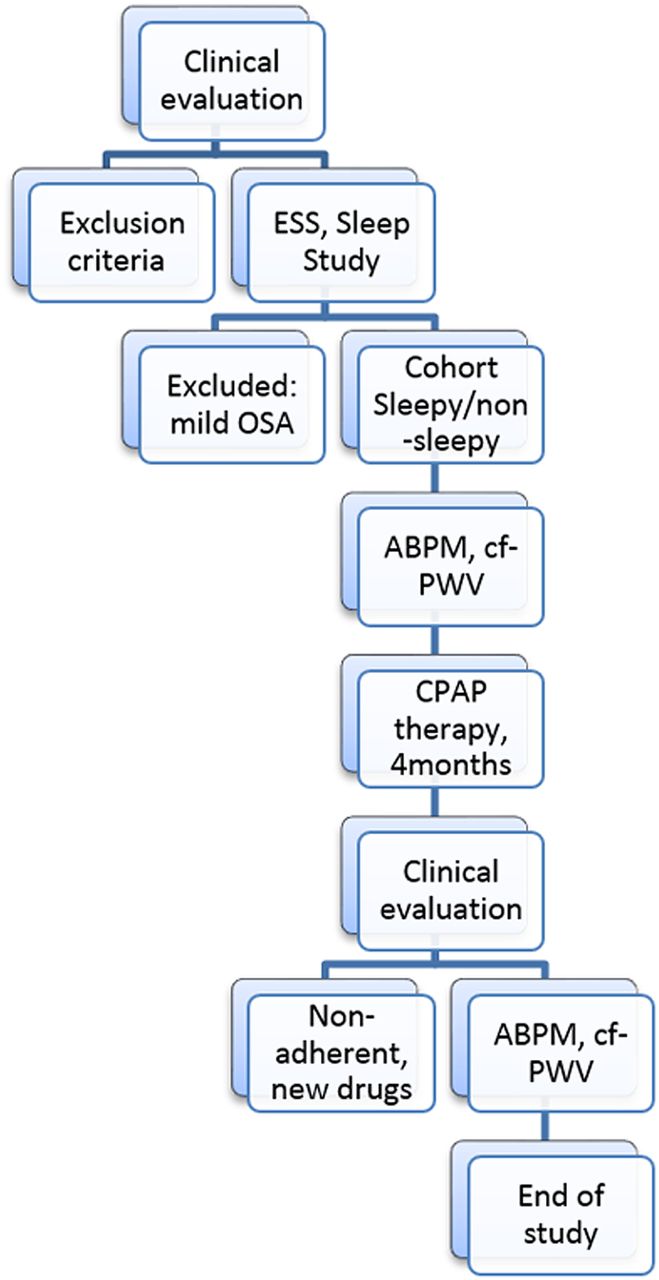
The sample is divided into two cohorts according to the ESS and the effect of CPAP therapy on sleepy (ESS>10) and non-sleepy (ESS≤10) patients will be compared (figure 1).

{kind=link}
Study design. ABPM, ambulatory blood pressure monitoring; CF-PWV, carotid-femoral pulse wave velocity; CPAP, continuous positive airway pressure; ESS, Epworth Sleepiness Scale; OSA, obstructive sleep apnoea.
The primary outcome is the variation of cf-PWV after therapy with CPAP. The effect of a 4-month trial of CPAP therapy is assessed. For ethical reasons, each patient will act as its own control.
Obesity and metabolic syndrome are common findings in OSA, and possible changes of metabolic parameters after CPAP are relevant.18
Secondary outcomes are ambulatory blood pressure monitoring (ABPM) variations and metabolic changes after treatment with CPAP.
The study is exploratory in nature and is based on a convenient sample, limited by the number of eligible patients consenting to participate. The effective sample size estimated for the primary outcome was 70 patients in order to demonstrate a reduction on cf-PWV from 12 to 11 m/s (from baseline to 4 months on CPAP), with 95% CI and power 80%. Based on the previous assessment of the institutional experience on compliance with CPAP and with outpatient clinic consultations, the recruited sample was increased in 15% to obtain a final sample of 80 patients.
Recruitment started on October 2012 and data collection is expected to end by June 2016.
Inclusion criteria
Patients referred to the Outpatient Sleep Clinic of the Pneumology Department, CHLC, Lisbon, because of snoring or other symptoms suggestive of OSA, were eligible for the study if they met the following criteria: males, younger than 65 years old, living in Greater Lisbon and with confirmed moderate-to-severe OSA (AHI>15/hour). To confirm this, on the first consultation, data on anamnesis and clinical examination were collected and the Epworth questionnaire was used.
Exclusion criteria
Patients are excluded if they have a history of CV events, established heart disease (beyond arterial hypertension) and peripheral vascular disease. Patients who are smoking (over 10 units pack/year) or consuming alcohol (>80 g/day) are not accepted. Other severe chronic diseases (assessed by chronic use of medication), chronic ingestion of hypnotics or other sleep disorders (clinically identified) are among the exclusion criteria.
Patients with diabetes are excluded, as they might have vascular involvement.
However, patients with some comorbidities namely hypertension and metabolic syndrome are allowed. Patients with antihypertensive medication and undergoing treatment of dyslipidemia are allowed as well.
Baseline evaluation
The Outpatient Sleep Clinic protocol for patients referred due to snoring or other symptoms suggestive of OSA require clinical evaluation, blood test, ECG and sleep study.
ESS will be applied by the principal investigator, and the presence of comorbidities and pharmacotherapy in progress is evaluated.
The collection of data regarding duration of comorbidity or pharmacotherapy has not been considered since including these two factors as liable intervening factors would greatly increase the sample size.
Anthropometric data regarding adiposity and vital signs are collected. Body mass index (BMI) is calculated as weight (kg) divided by height (m) squared.
BP will be measured while the patient is in a quiet room, using a semiautomatic device (Omron HEM-907XL, Omron Healthcare, Bannockburn, Illinois, USA) with an appropriate cuff. The patient should not have taken stimulants 3 hours prior to BP measurement. Two measurements are taken with a minimum of 3 min interval and the average is considered. When large differences existed among the measurements, additional measurements were performed.
The analytical screening evaluation includes glycated haemoglobin, fasting glucose, total cholesterol, high-density lipoprotein, low-density lipoprotein and triglycerides; for in patients with high levels of fasting glucose, an oral glucose tolerance test will be performed. Dyslipidaemia, glucose intolerance and metabolic syndrome are diagnosed according to current guidelines.19
An ECG (Page Writer TC 30, Philips, Eindhoven, Netherlands) will be performed by the same technicians, as per institutional protocol.
Sleep study
To confirm the diagnosis of OSA, patients will submit to a polygraphic cardiorespiratory sleep study type 3 (Embletta system, Broomfield, USA), a portable equipment that performs continuous recording from a nasal cannula (pressure and flow), thoracic–abdominal motion, pulse oximetry, ECG and a body position sensor. Results from the sleep studies are analysed by two trained technicians using standard criteria.20
Ambulatory blood pressure monitoring
All participants will undergo 24 hours BP monitoring using an ABPM device—Spacelabs model 90207 (Issaquah, Washington, USA), according to the current guidelines. Patients are classified as normotensive if the average systolic and diastolic BP values obtained by the ABPM are within normal limits and are classified as hypertensive if already on antihypertensive medication or if the average BP values obtained from the ABPM are above ≥130 mm Hg for systolic and/or ≥80 mm Hg for diastolic.11
Pulse wave velocity
Non-invasive assessment of cf-PWV (Complior, Colson, Paris, France) will be performed by the same operator. For this, the investigators followed the recently published expert consensus document.21 In a few words, the measurement is done at the right common carotid and the right common femoral artery after 10 min rest in supine position. Two pressure waveforms were transcutaneously recorded at the base of the neck for the right common carotid artery and over the right femoral artery. The pulse transit time was determined as the average of 10 consecutive beats. The straight line distance between the measurement sites is obtained by surface measurement, with the patient in the supine position. cf-PWV is calculated as the ratio of distance to transit time. In order to normalise cf-PWV values according to the arterial pathway, the threshold of 10 m/s for cf-PWV evaluated by the full direct carotid-to-femoral distance was considered.21
Standard CPAP intervention
According to the current clinical recommendations,4 patients with moderate or severe OSA are offered therapy with non-invasive ventilation by CPAP. Additionally, patients receive counselling on sleep hygiene.
An auto-CPAP device (ResMed S9 AutoSet, California, USA) is used. CPAP will be titrated for 3 nights. The definitive value of CPAP is the amount of pressure that eliminates events in ∼95% of the total sleep time (95th centile), once confirmed that there is no significant leakage the nasal mask is used.22
Patients will be assessed monthly for compliance and effectiveness of the intervention. Compliance to the CPAP is measured using the data from the CPAP card; a patient is considered to be in compliance when using CPAP at least 4 hours/day (average) in at least 70% of nights. CPAP is considered effective if the AHI falls below 5/hour.23
The presence of nasal symptoms or changes on the equipment will be taken into account.
Follow-up assessments
After 4 months of standard CPAP intervention, patients will undergo a clinical evaluation, including ESS and analytical evaluation, similar to the one on baseline. BMI, ABPM and cf-PWV will be assessed, as well as compliance to CPAP and the effectiveness of CPAP therapy.
At any point of the study, patients will be excluded from follow-up if do not comply with CPAP, if significant weight loss (>10%) occurs,4 if new drugs are prescribed or if new diseases are diagnosed.
Statistical analyses
The primary outcome measure (cf-PWV) is compared before and after the therapy with CPAP for 4 months. Analysis is performed as per intention to treat.
Continuous variables are described with median and IQR (25th–75th centile) or extreme values, as previous evaluations have evidenced that a normal distribution of values was not to be expected. Data of sleepy and non-sleepy patients at each evaluation are compared using the Mann-Whitney test. Categorical variables are described as percentage and are compared with Pearson's χ2 test or Fisher's exact test; stratified Mantel-Haenszel analysis is performed as appropriate.
The categorised outcome measure (using the threshold of 10 m/s for cf-PWV21) is used to estimate the incidence rates of the outcomes and relative risk estimates, both with 95% CIs.
Measurements on the cohort before and after 4 months of CPAP therapy are analysed using generalised linear mixed-effects models for repeated longitudinal data, to explore associations between outcomes and exposures, in order to assess factors influencing the success of the intervention.
Discussion
The results of this study will disclose differences in the CV risk and the response to CPAP therapy among patients with and without daytime sleepiness. In the subgroup of less-symptomatic patients, the benefits of CPAP have yet to be identified.
This observational study protocol has the limitations of convenience, non-randomised sample, and the exclusion of patients with mild OSA or older patients. The strengths of this protocol are the controlled clinic-based setting, the use of standardised instruments to characterise OSA and sleepiness, and the use of standardised quantitative early indicators of CV risk (cf-PWV), a useful indicator of subclinical CV disease.
Dissemination
The study has been registered as STIFFSLEEP at ClinicalTrials.gov (ID: NCT02273089). Informed, written consent will be obtained. Results will be presented at conferences and published in peer-reviewed journals.
References
Footnotes
Contributors MAM developed the conceptual clinical background of the protocol. PMdS provided clinical background and methodological input for the cardiovascular risk assessment. MA and DV contributed to the epidemiological design, causal framework and proposed epidemiological and statistical analyses. MJMG and JC provided scientific overview. All the authors provided intellectual input to the editing of the manuscript and preparation for publication.
Funding This work was supported by the Pneumology Department, CHLC, Lisbon, and by a gracious grant from Vitalaire SA (Lisbon).
Competing interests None declared.
Patient consent Obtained.
Ethics approval This protocol was approved by the Ethics Committees of CHLC (reference number 84/2012), NOVA Medical School, Lisbon (number 36/2014/CEFCM) and the Portuguese Data Protection Authority.
Provenance and peer review Not commissioned; externally peer reviewed.