Article Text

Abstract
Introduction The number of major joint replacement procedures continues to increase in Australia. The primary aim of this study is to determine the incidence of falls in the first 12 months after discharge from hospital in a cohort of older patients who undergo elective total hip or total knee replacement.
Methods and analyses A prospective longitudinal observational cohort study starting in July 2015, enrolling patients aged ≥60 years who are admitted for elective major joint replacement (n=267 total hip replacement, n=267 total knee replacement) and are to be discharged to the community. Participants are followed up for 12 months after hospital discharge. The primary outcome measure is the rate of falls per thousand patient-days. Falls data will be collected by 2 methods: issuing a falls diary to each participant and telephoning participants monthly after discharge. Secondary outcomes include the rate of injurious falls and health-related quality of life. Patient-rated outcomes will be measured using the Oxford Hip or Oxford Knee score. Generalised linear mixed modelling will be used to examine the falls outcomes in the 12 months after discharge and to examine patient and clinical characteristics predictive of falls. An economic evaluation will be conducted to describe the nature of healthcare costs in the first 12 months after elective joint replacement and estimate costs directly attributable to fall events.
Ethics and dissemination The results will be disseminated through local site networks and will inform future services to support older people undergoing hip or knee joint replacement and also through peer-reviewed publications and medical conferences. This study has been approved by The University of Notre Dame Australia and local hospital human research ethics committees.
Trial registration number ACTRN12615000653561; Pre-results.
- PREVENTIVE MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The study will be conducted in a large tertiary hospital where multiple surgeons perform elective joint replacement procedures.
Comprehensive falls data collection methods will adhere to guidelines for falls research.
Economic evaluation of the cost of falls after hospital discharge will aid in understanding healthcare costs in this population.
The study population comes from one tertiary hospital; therefore, results may not be generalisable to differing healthcare settings.
The follow-up period of 12 months in an older population may result in patients dropping out of the study.
Background
Hip and knee replacements are increasingly common procedures undergone by older people, with over 97 000 hip and knee replacement procedures being performed in Australia in 2014.1 The number of hip replacement procedures performed has increased by over 58% since 2003, with the number of knee replacement procedures increasing by over 88% during the same period.1 There is uncertainty about the incidence of falls in the discharge period after total hip replacement (THR) or total knee replacement (TKR). Studies conducted in medical, rehabilitation and acute care populations have documented that the incidence of falls in postdischarge populations is higher than in the general community population.2–4 These findings include an increased rate of hip fracture.5 However, these studies were not conducted among older patients who had undergone major joint replacement surgery. Additionally while most patients report high levels of satisfaction following their joint replacement surgery,6–9 evidence suggests that between 7% and 30% of patients are dissatisfied with the outcome including reporting limited or no improvement, reduced functional ability and health-related quality of life.7 ,8 ,10–12 Functional decline and reduced health-related quality of life have been shown to be associated with falls.13 ,14
Older patients who have undergone THR or TKR have been found to have some increased risk of falls, but high-quality evidence is sparse and the size and scope of this problem remains uncertain. Older adults who undergo joint replacement surgery may have reduced proprioception, as well as a short-term increase in pain and reduction in muscle strength following surgery.15–17 These deficits as well as the hospital admission itself may affect older adults who have less physical reserve and ability to compensate for these deficits than younger adults. Studies conducted in post-TKR populations have found that between 24% and 45% of patients report they have fallen;17–21 however, these studies had methodological limitations including not being prospective, not using recommended methods for collecting falls data (such as identifying falls events using monthly reporting) or having a small sample size. Two large retrospective cohort studies also found that the risk of hip fracture is increased in the 12 months after TKR, suggesting that falls rates in this population may be higher than those among broader community populations.22 ,23 Both studies demonstrated that the incidence of hip fracture was >50% higher than the general community incidence rate, only returning to normal rates 3 years after surgery. Despite other data which found that over 90% of hip fractures can be attributed to falls,24 these studies were not able to retrospectively collect falls data so were unable to calculate the falls rates for this population. The studies were also unable to evaluate the psychological consequences of falls, minor physical injuries or other more serious injuries resulting from falls such as head injuries. In Australia, falls resulting in head injuries have increased by ∼7% each year from 1999–2000 to 2010–2011.25 Given the poor outcomes associated with traumatic brain injury among older people,26 ,27 head injury is an important outcome to measure when investigating the consequences of falls among older people.
A recent large longitudinal study (n=5154) among patients who had a 3-day admission for THR or TKR examined hospital admission data for 90 days postdischarge and found that 1.6% of patients were readmitted for a fall-related injury.28 The study did not report falls rates or the incidence of injuries which did not result in presentation to hospital, and recommended methods of gathering falls data were not adhered to. A cross-sectional survey of 214 older people after THR reported that 36% of patients fell in the year following their THR, which was high considering the mean age of the sample was 66 years, but this study also did not use recommended methods of gathering falls data and no falls rates were reported.29
Falls are the leading cause of injury-related hospital admissions in older people in Australia requiring ∼1.3 million patient bed days in 2009–2010.30 Despite this, other older postdischarge populations have been found to have low levels of knowledge about falls prevention after discharge and engagement in exercise.31 ,32 Addressing this gap in knowledge by clarifying what older people undergoing THR or TKR understand about falls prevention may inform the design of postdischarge falls prevention information for these patients. Additionally while the estimated direct hospital costs alone for falls-related hospitalisations for 2007–2008 in Australia was over $645 million,33 there are no published studies that specifically examine the healthcare costs of falls among a postdischarge older population.
The primary aim of the study is to investigate the incidence of falls in the first 12 months after discharge from hospital, among a cohort of older patients who undergo elective THR or TKR. The secondary aims are to investigate the incidence of injurious falls, identify risk factors independently predictive of falls and examine health-related quality of life in fallers and non-fallers in the 12 months after hospital discharge. An economic evaluation will also describe the nature of healthcare costs in the 12 months before and 12 months after elective THR or TKR and estimate costs directly attributable to fall events.
Methods
Design
A prospective, single-centre, longitudinal, observational, cohort study will be undertaken and reported according to Strengthening the Reporting of Observational Studies in Epidemiology guidelines34 (see figure 1).
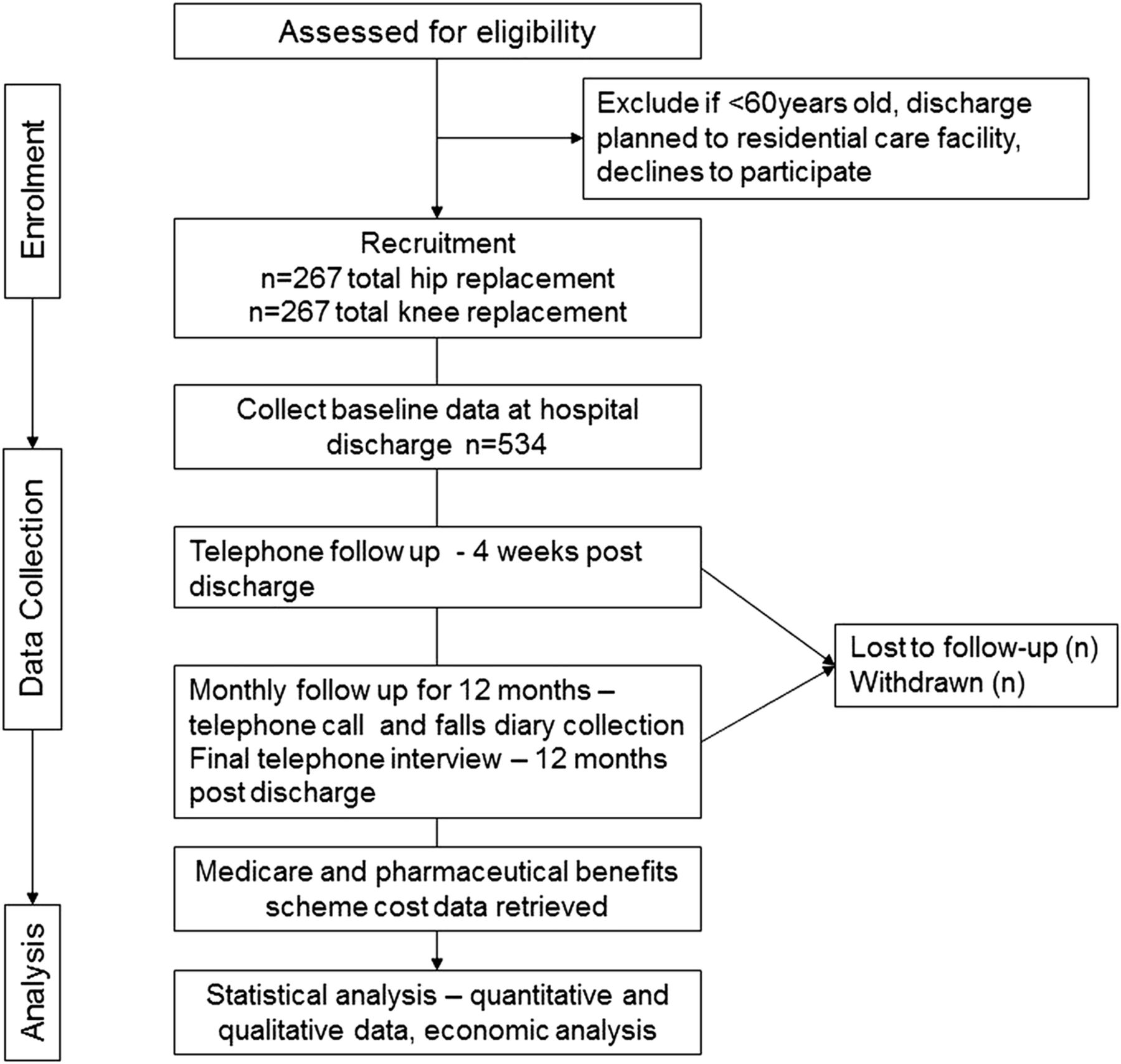
{kind=link}
Participant flow through study.
Ethical considerations
The study has received ethics approval from University and local hospital human research ethics committees. Patients will be required to provide written consent to participate in the study or have next of kin provide written agreement for the patient to participate if the patient's Short Portable Mental Status Questionnaire score is below 8/10 (indicating an impaired level of cognition).35 Patients are also asked to provide additional consent for access to their pharmaceutical and medical benefits data, required as part of the economic evaluation of the study.
Setting and study population
The setting is the orthopaedic wards of a large private tertiary hospital in Perth, Western Australia. The hospital performed ∼1450 TKR and THR procedures in 2013–2014 by 15 orthopaedic surgeons. Patients admitted to the wards will be eligible for inclusion in the trial if they are aged ≥60 years, have undergone elective THR or TKR (including primary joint replacements and revisions) within the week prior to recruitment, are to be discharged to the community and are able to read and understand English. Exclusion criteria are undergoing emergency THR following fractured neck of femur, not being able to read or understand English or planned discharge to a residential aged care facility, such as a nursing home.
Recruitment
Eligible patients admitted to the participating wards from July 2015, who are to undergo THR or TKR, will be identified through operating lists at the hospital and approached consecutively in order of admission by the research assistant (RA), who will be provided with training in conducting interviews and administering assessment tools. Recruitment occurs postoperatively and prior to hospital discharge. Those who provide written consent will be enrolled in the trial in order of recruitment. Patients who are screened as having an impaired level of cognition will not be automatically excluded, but agreement will be sought from the patient and the patient's next of kin, who will also be the point of contact for the monthly follow-up telephone calls. A specific participant information sheet and consent form for patients with cognitive impairment and their families will be used in these circumstances.
Outcome measures
The primary outcome measure is patient falls in the 12 months following discharge, expressed as the rate of falls (number of falls per 1000 patient-days). Secondary outcome measures include the number of injurious falls expressed as the rate of injurious falls per 1000 patient-days and the proportion of patients who experience one or more falls. Falls will be defined as ‘an event which results in a person coming to rest inadvertently on the ground or floor or other lower level’.36 A faller will be defined as a participant who has sustained one or more falls during the observation period. A fall injury will be defined as any physical harm resulting from a fall reported by study participants during the observation period. Falls injuries will be classified as mild (pain, bruising or abrasion), moderate (wound requiring sutures, laceration or sprains) or serious (dislocation, fracture or head injury).37 To permit accurate calculation of rates of falls, the period of time each patient remains in the trial (length of stay in trial) will be recorded. Patients will remain in the study until their observation period (12 months) is completed, or until death, withdrawal or loss to follow-up.
Falls will be measured in two ways. First, a falls diary will be issued to participants prior to discharge from hospital. The RA will explain the definition of a fall as described above and ask participants to record any fall details in their diary. Participants will be asked to return their diary monthly page at the end of each month. Second, the RA will call each participant monthly after discharge and ask about falls events using the recommended questioning method: ‘In the past month, have you had any fall including a slip or trip in which you lost your balance and landed on the floor or ground or lower level?’. At this time, participants will also be asked to check their diary and to recall any events in the past month, as monthly recall has been shown to improve accuracy of recall of falls events by older people.38 For those participants who have an impaired level of cognition or a sensory impairment such as decreased vision, their nominated next of kin or family will be permitted to assist them to keep their diary and respond to telephone calls. All falls events will be coded using the following descriptors: date of fall, time of day, location, injury or no injury, type of injury if any, medical or no medical attention, including whether a visit to a health professional was undertaken and what type of visit such as visiting a doctor, having X-rays or nursing attention, use of an ambulance, any medications prescribed for the resulting injury, hospital admission and the amount of medical attention.
The other secondary outcomes are as follows:
Health-related quality of life, which will be measured using EQ-5D-5L.39 This questionnaire is a quality-of-life instrument which comprises five dimensions (mobility, self-care, usual activities, pain/discomfort and anxiety/depression) and a visual analogue scale for respondents to self-rate their health state. This instrument can be reliably administered over the telephone.40
Participants' perceptions of the causes and consequences of falls which occur in the 12 months after hospital discharge; their awareness and knowledge about falls and falls prevention strategies; and their motivation to engage in falls prevention behaviours. These outcomes will be measured at 12 months using a semistructured interview.
Economic outcome measures
Healthcare costs will be calculated for each participant for the 12 months before and the 12 months after elective joint replacement, including government, insurer and out-of-pocket costs from Medicare (Australia) items and Pharmaceutical Benefits Scheme (PBS) prescriptions. This will enable healthcare costs to be calculated for each patient presurgery and postsurgery and then to be compared for patients who do and do not fall following surgery. Cost estimates to address the economic outcome measure will be generated using data from three sources: Medicare and PBS data, inpatient medical records and monthly patient telephone interviews. The participating hospital's administrative records will be used to capture information about readmissions to the same facility. Monthly telephone follow-up will identify admissions to other hospital facilities, as well as the reasons for admission, length of stay and any other health costs incurred by the participant as a result of a fall.
Data collection and procedure
Baseline demographic data will be collected prior to the patient's discharge from hospital including age, date of operation, type of replacement (hip, knee, unilateral, bilateral and revision), length of stay in hospital, comorbidities, cognition, falls in the preceding 12 months prior to surgery, presence of any visual impairment, number and type of medications taken, and use of any home care services. Other data collected at baseline and at intervals after discharge will be functional ability, measured using the Katz Index of Independence in Activities of Daily Living (ADL)41 and the Lawton Instrumental Activities of Daily Living Scale,42 fear of falls (measured using Falls Efficacy Scale-International)43 and mobility level, including the use of walking aids. Patient-reported outcomes after the hip or knee surgery will be measured using the Oxford Hip or Oxford Knee score.44–46 These joint specific questionnaires ask patients a series of questions which allow them to rate their level of pain and aspects of functional ability following surgery. The procedure to measure these covariates at baseline and subsequent time points is shown in table 1.
Study procedure
Monthly follow-up phone calls will start 4 weeks after discharge from hospital as outlined in table 1. Participants will be asked during each phone call to recall details of any falls events since discharge or their last telephone contact with the RA. Participants will also be asked to return their monthly falls diary by post. On completion of the 12-month telephone call, participants will be asked whether they would like to participate in a further final recorded telephone interview, which seeks to explore older participants' perceptions of the causes and consequences of falls and their confidence and motivation to engage in falls prevention programmes.
Statistical analysis
The primary outcome measures (rates of falls) and secondary outcome measure of rates of injurious falls will be expressed using an incident rate per 1000 days. The number of fallers will be expressed as a percentage. Generalised linear mixed modelling will be used to examine the falls outcomes (falls and injurious falls rates and the proportion of patients who fell) in the 12 months after discharge. The analyses for this study will be conducted under a mixed modelling framework whereby parameterisation during the modelling process will be influenced by the nature of the data in order to return the most appropriate model fit (after accounting for penalty for complex parameterisation to avoid overfitting the model using an appropriate information criterion, eg, the Akaike information criterion). Generalised linear mixed modelling will also be conducted to examine patient and clinical characteristics predictive of falls in the 12 months after discharge. Unadjusted univariable analysis will be undertaken, followed by generalised linear mixed modelling, including such variables as age, male gender, presence or absence of cognitive impairment, whether or not assistance is required with ADLs, history of falls in the 6 months prior to admission, visual impairment, use of walking aids, Oxford Hip or Oxford Knee score and whether or not a fall occurred in hospital, along with adjustment for length of stay in the study. These variables include those that have been shown to be predictive of falls in other postdischarge populations.2 ,3 Proportional hazard models will be used to examine factors associated with the risk of first fall. Factors associated with multiple falls will be examined using an extension of the Cox Proportional Hazard model (frailty model),47 which can estimate the risk of subsequent falls conditional on previous falls.
Participants' health-related quality of life over the first 12 months following discharge from hospital will be examined among fallers and non-fallers using adjusted and unadjusted generalised linear modelling. Generalised linear mixed modelling will be conducted to identify patient and clinical characteristics (including falls outcomes) predictive of patient's health-related quality of life. Participants' awareness of the risk of falls, awareness and knowledge about falls and falls prevention, and motivation to engage in falls prevention strategies will be summarised using descriptive statistics. Comparison between fallers and non-fallers outcomes will be conducted using Wilcoxon rank sum tests, and generalised linear mixed modelling will be used to examine patient characteristics predictive of these outcomes. Data from items in semistructured interviews that require verbatim responses will be treated as qualitative data and coded, categorised and thematically analysed.48 Telephone interviews will be digitally recorded, transcribed verbatim into individual word files (with all patient names de-identified) and analysed using content analysis.49
Sample size
In a previous study conducted in a large and broad diagnostic postdischarge population, the annual incidence rate for falls after hospital discharge in an older population was reported to be 4.5 falls/1000 person-days (or 1.23 falls/person-year).2 The proposed sample size for the present study is 267 patients in each of the THR and TKR cohorts, which would lead to ∼328 falls observed if the present study was consistent with the previous report of 1.23 falls/person-year.2 It is likely that fall count data will approximate a Poisson distribution. Therefore, the present study is powered to estimate the Poisson parameter to within 11% of its true value using a 5% significance level (at 4.5/1000 person-days or 328 falls observed in each of the THR or TKR cohorts, 95% CI interval of 293 to 365 falls representing a total width of 22%).
Economic analysis
Analyses of costs from the perspective of the health service provider (including Medicare and PBS items) for the 12 months prior to and 12 months following joint replacement will be undertaken for fallers and non-fallers. We will examine the types of services and number of service providers accessed (and repeated use of the same providers), the costs associated with these services (including government and out-of-pocket payments for concession and non-concession holders), in-hospital and out-of-hospital costs and an estimate of healthcare costs directly attributable to falling in the postoperative period. Owing to potential uncertainty of distribution for some data, bootstrap resampling (2000 replications of original sample size) will be conducted as necessary to generate 95% CIs and indicate potential variance in cost data. Sensitivity analyses will be conducted where necessary to investigate the potential influence of any variation in assumptions used during the evaluation of economic data.
A significance level of p<0.05 will be used for all analyses. Statistical tests will be conducted using Stata V.13 software (StataCorp, College Station, Texas, USA).
Discussion
The transition period between hospital and home is a time of high risk for older adults. Older people are an important subgroup within the posthospital discharge population; between 2013 and 2014, Australians aged ≥65 years used 48% of all hospital bed days.50 Falls and related injuries are increased in this population resulting in significant physical, psychological and socioeconomic costs to the patient and the healthcare system.2–4 Despite this, the magnitude of this problem among patients who are discharged after undergoing THR or TKR and the true economic cost of falls in this population are unknown. However, age standardised rates of hospital admissions due to injurious falls have increased by 2% per year between 1999 and 2013,25 and falls are known to form a substantial economic burden worldwide.33 ,51–53
This cohort is being recruited from the private hospital sector which undertakes the majority of hip and knee replacement procedures in Australia (59% for hip surgery and 70% for knee surgery in 2013).1 Therefore, results may not be able to be generalised to THR or TKR populations in public health settings. Strengths of the study include the prospective design and robust data collection by use of recommended methods to capture falls data, with monthly phone calls and falls diaries. Personal monthly telephone contact with participants will also facilitate comprehensive collection of injurious falls data. The study is also adequately powered to determine the falls rates and compare this rate with previous studies conducted in postdischarge populations. The 12-month observation period may lead to older patients dropping out, resulting in missing observations. Other limitations of the study are that it is being conducted at one site only and participants are recruited postoperatively which means that the first measurement of the Oxford scores will ask participants to recall their usual level of functioning over the past 4 weeks prior to admission. Physical characteristics of strength and balance are also known to be associated with falls, but the study will not collect these data to minimise participant burden and retain participants in the study. However, participants' health-related quality of life, patient self-reported outcomes and functional ability outcomes will be measured.
Conclusion
These findings will provide rigorous evidence about the rate of falls in the 12 months after discharge in a large joint replacement cohort and the cost of falls in this population. The findings will also assist in identifying whether falls in this population affect health-related quality of life after joint replacement. Findings will inform the development of falls prevention strategies and interventions, which can be evaluated for their effect on optimising functional recovery and reducing falls in this population.
References
Footnotes
Contributors A-MH was awarded a grant which was used to fund the trial. A-MH, SMM, GR-A and LM conceptualised the trial design and resultant research protocol with ongoing expertise and support from MB, CE-B, GH and SJP. A-MH and SMM provide expertise for the falls data collection, management and analyses and GR-A manages the project at the hospital site with support from GH, A-MH and LM. All investigators provide ongoing expertise regarding recruitment, data collection at the site and management of data in preparation for analyses. SMM provides economic expertise to direct the healthcare cost analyses for the trial. A-MH led the drafting of all sections of the manuscript in consultation with SMM, GR-A, MB and CE-B. All authors critically revised the manuscript for important intellectual content and gave final approval of the version of the manuscript to be published.
Funding The study was funded by a grant awarded to A-MH from the Department of Health, Government of Western Australia. The funder has no role in design, conduct of the study, data analyses or dissemination of results. SMM is supported by a National Health and Medical Council of Australia career development fellowship.
Competing interests None declared.
Ethics approval The University of Notre Dame Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.