Article Text

Abstract
Objectives To describe older adults' perceptions of evaluating and comparing pharmacies based on the Consumer Experience with Pharmacy Services Survey (CEPSS), describe older adults' perceived importance of the CEPSS and its specific domains, and explore older adults' perceptions of the influence of specific CEPSS domains in choosing/switching pharmacies.
Design Focus group methodology was combined with the administration of a questionnaire. The focus groups explored participants' perceived importance of the CEPSS and their perception of using the CEPSS to choose and/or switch pharmacies. Then, using the questionnaire, participants rated their perceived importance of each CEPSS domain in evaluating a pharmacy, and the likelihood of using CEPSS to switch pharmacies if their current pharmacy had low ratings. Descriptive and thematic analyses were done.
Setting 6 semistructured focus groups were conducted in a private meeting room in a Mid-Western state in the USA.
Participants 60 English-speaking adults who were at least 65 years, and had filled a prescription at a retail pharmacy within 90 days.
Results During the focus groups, the older adults perceived the CEPSS to have advantages and disadvantages in evaluating and comparing pharmacies. Older adults thought the CEPSS was important in choosing the best pharmacies and avoiding the worst pharmacies. The perceived influence of the CEPSS in switching pharmacies varied depending on the older adult's personal experience or trust of other consumers' experience. Questionnaire results showed that participants perceived health/medication-focused communication as very important or extremely important (n=47, 82.5%) in evaluating pharmacies and would be extremely likely (n=21, 36.8%) to switch pharmacies if their pharmacy had low ratings in this domain.
Conclusions The older adults in this study are interested in using patient experiences as a quality metric for avoiding the worst pharmacies. Pharmacists' communication about health and medicines is perceived important and likely to influence older adults' pharmacy selection.
- Older adults
- Pharmacy
- Quality in healthcare
- Quality measures
- Patient experience survey
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
For the first time, research examines older adults' perceptions of pharmacy patient experience measures, which is important as pharmacy quality organisations aim to include patient experiences as part of a pharmacy's quality metrics.
This is the only study to examine whether older adults perceive patient experience measures (that may be publicised in pharmacy quality reports) as important or useful in their healthcare provider selection.
This study is significant in improving the quality of care provided by pharmacy providers as the pharmacy profession moves towards the development of quality ratings that can be understood and used by patients to inform their pharmacy selection.
Limited geographical area.
Convenience sample.
Background
Public reporting of quality of care information has been suggested as a means for patients to actively choose best performing providers that deliver quality and efficient care.1 With access to provider performance data, it is assumed that patients are aware of the differences in quality of care and can make an informed decision based on this information.2 It is expected that when patients become selective of their healthcare providers based on publicly available performance information, providers will be forced to improve quality of care, so that they can maintain their reputation and stay competitive.3
Although work has been done to encourage patients to utilise provider performance information to choose their healthcare providers, it is disconcerting to know that available public reports are not commonly used by patients, and the public reports do not have a substantial effect on patients' decision-making.2 ,4 This is due to a myriad of factors, including a lack of awareness of available provider performance information and low perceived usefulness of the information.3 ,5–7 In addition, it is reported that patients do not have an interest in using provider performance information because the information presented is irrelevant and contains provider performance measures that are not understandable.8 ,9
As it relates to pharmacy choice, our previous studies showed that patients do not understand the meaning and interpretation of pharmacy performance measures and few individuals are likely to use them to make an informed pharmacy choice.8 ,10 ,11 It has been suggested that one way to get patients to use quality information in guiding their provider choice is to consider the features of quality that patients care about and that patients believe are relevant to their choice.12 ,13
Patient care experience measures are increasingly used in public reporting to highlight the patient's perspective of their care.14 Standardised patient surveys such as the Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey is a mechanism through which the information and experiences that patients gain while using health services can be captured and summarised.15 Although data describing patients' healthcare experiences might be used by consumers to choose better performing providers (eg, hospitals) as well as hold them accountable,16 no one facilitated the development of patient care experience surveys for the care provided in ambulatory (outpatient) pharmacies until recently. A standardised survey, the Consumer Experience with Pharmacy Services Survey (CEPSS), has been developed for patients' evaluation of pharmacy services received in an ambulatory care setting.15 ,17
The CEPSS was developed as a mechanism for benchmarking the quality of pharmacy services provided by pharmacists nationwide. Most patients use a pharmacy for ambulatory care services such as filling a prescription medication, obtaining medication information about an overcounter drug, or getting advice about disease self-management.15 With the CEPSS, the information relevant to pharmacy quality based on patients' interactions with pharmacists can be captured from survey responses. Based on the CAHPS initiative, the CEPSS is a reliable and valid survey to capture patient perceptions of pharmacy quality. There are four measures of pharmacy quality within the CEPSS: pharmacy staff communication, health-focused and medication-focused communication, pharmacy care, and clarity of written information about medicines (table 1). Similar to the CAHPS survey, the rationale for the CEPSS is that it can be used by healthcare organisations, insurers, and patients as a quality metric in evaluating and comparing a pharmacy's performance and ultimately motivate patients to choose high-quality pharmacies.15 ,17
The Consumer Experience with Pharmacy Services Survey (CEPSS)* quality domains
Previous studies have reported mixed results related to the usefulness of the CAHPS survey in patients' evaluations of hospitals and health plans,1 ,2 ,18–22 and the importance of the CAHPS measures in patient decision-making.1 ,23 ,24 Since the development of the CEPSS, no research has examined whether patient experience information might be useful to patients' evaluations of pharmacies and if the CEPSS is important in patients' decision-making concerning their pharmacy. Also, we do not know if patients' perceptions of the usefulness of the CEPSS are similar to reported usefulness of the CAHPS survey. In our previous study, patients with chronic illnesses who discussed the usefulness of clinical pharmacy quality measures also wanted to see consumer experience quality metrics.11 It is assumed that the CEPSS will be important to pharmacy consumers for several reasons. For example, a pharmacist may ensure the accuracy of a prescription medication, check the appropriate labelling of a prescription medication, and ensure the safe administration of the medicine by checking for drug interaction. Based on clinical quality metrics, this pharmacy may be ranked as ‘high technical quality’. However, the pharmacist may not give the patient the amount of time and attention needed, answer their questions appropriately, or offer private counselling spaces during the discussion of sensitive health issues. These aspects of pharmacy quality can only be evaluated based on patient input and experience.15 Hence, the CEPSS can be important as a quality metric in facilitating patients' pharmacy choice.
This study focuses on older adults' perceptions of using the CEPSS to evaluate and compare pharmacies, their perceived importance of the survey, and the perceived influence of the survey in their pharmacy selection. The research is significant to older adults because they use a lot of medicines, are more likely to have a chronic condition and are at risk for preventable adverse drug events.25 Owing to these reasons, they are more likely to talk to the pharmacist about their prescription medicines and use pharmacies for medication reviews, disease management and other pharmacy services.26 Exploring older adults' perceptions of the CEPSS will allow this information to be used in the development of public reports that will help them identify better performing pharmacies.
According to Hibbard et al's24 theoretical consumer choice model, a psychological process takes place in a patient's mind before they proceed with a behaviour (ie, provider decision-making using quality information). Specifically, the model proposes that patients need to be aware of the availability of quality information, trust the information and perceive the information as useful to them (the psychological processes) before it can be used in their decision-making (the behaviour).2 ,5 ,24 This study explores, in part, these psychological processes among older adults who could potentially use pharmacy quality information.
Objectives
The objectives of the study are to (1): describe older adults' perceptions of evaluating and comparing pharmacies based on the CEPSS; (2) describe older adults' perceived importance of the CEPSS and its specific domains and (3) explore older adults' perceptions of the influence of specific CEPSS domains in choosing/switching pharmacies.
Methods
Sample
The convenience sample for this study consisted of English-speaking individuals who had filled a prescription at a retail pharmacy within 90 days of recruitment and who were at least 65 years of age. The authors partnered with staff at senior apartment facilities and community centres to recruit participants by means of email announcements, word of mouth and flyers. Participants were informed of the study's eligibility criteria, objectives and compensation for participating ($50 cash). Recruiters enlisted the participation of men and women who had the capacity and ability to provide consent. Based on the number of participants who responded to the recruitment efforts, 60 people were recruited to six focus groups. There were no drop-outs or refusals to participate.
Study design and data collection
Using a phenomenology approach, focus groups were chosen as the data collection method because the ways in which older adults think about and might use pharmacy patient experience measures are insufficiently understood. Focus groups allowed for gathering and exploring a wide range of perspectives on pharmacy quality. A semistructured questioning route was developed by the authors and used at all six groups. The focus group guide was not pilot-tested prior to the start of the study. The participants were informed of the reasons for conducting the research and the reason for the investigators' interest in the research topic. One of the authors (KDC), a trained male focus group moderator and a PhD-trained cultural anthropologist, who has 20+ years of experience conducting qualitative research, facilitated the groups. All groups were attended by the study's principal investigator (OOS). Field notes were taken by OOS during the focus groups and discussed with the moderator. Senior apartment facilities and community centres in Madison, Wisconsin, USA, served as venues for the groups. The groups took place from May to July 2014 and lasted ∼90 min each. Participants were not given any information about CEPSS before completing the focus groups.
To explore the triangulation of results, a brief 10 min, 12-item questionnaire was self-administered at the end of the focus groups. The questionnaire asked participants to rate the importance of each specific CEPSS domain in evaluating pharmacies (on a five-point Likert scale, response options were ‘not at all important’ to ‘extremely important’. Also, on a five-point Likert scale, participants indicated their likelihood of changing pharmacies if a pharmacy rated low in a specific domain (response options were ‘not at all likely’ to ‘extremely likely’). Participants' demographic information was also collected.
Analysis
The analysis in this article focuses on the following questions, which are a subset of questions administered at the focus groups:
I will ask you to imagine that you had access to a report that compares pharmacies based on all the aspects of pharmacy quality that we have been talking about (the following measures of pharmacy quality, including their definitions, which had been discussed individually, were displayed on a flipchart to facilitate participant discussion of the present question: health and medication-related communication, pharmacy staff communication, pharmacy care, clarity of written information provided with medications; see table 1 for descriptions). Imagine that the report would tell you which pharmacies do better and which do worse on these aspects of pharmacy quality. What would you think about pharmacies being evaluated and compared on these aspects?
What would you do if you read such a report and saw low-quality ratings for your pharmacy?
Which aspect of pharmacy quality, if you found it rated low in a report, would prompt you to change your pharmacy? What is important to you about this factor?
What are your thoughts on how to distribute a report on pharmacy quality to pharmacy customers?
The focus groups were audio recorded, transcribed verbatim by a certified transcriptionist, and independently coded by two of the authors (OOS and KDC). NVivo V.10 (QSR International, Burlington, Massachusetts, USA) was used to organise the data and to categorise the themes. Data saturation was discussed by OOS and KDC. Transcripts were not returned to participants for comments or corrections. The authors used descriptive coding, which is a method of coding qualitative data whereby words or short phrases are assigned to segments of text to capture their essential ideas, and to enable comparison of similar ideas across the entire qualitative data set (in our case, across all transcripts).27 The authors coded all transcripts independently and discussed coding divergences. They reached agreement on the application of all codes. All themes were derived from the data and were not identified in advance. The participants did not provide feedback on the findings.
Descriptive statistics were used to examine participant responses to the questionnaire including questions on perceived importance of each CEPSS quality domain and participants' likelihood of changing pharmacies if their pharmacy rated low in a specific CEPSS domain. The questionnaire responses were analysed using SPSS V. 21.0.
Results
There were 60 older adults in this study. Participants' ages ranged from 65 to 88 years old. At least 8 participants with a maximum number of 12 participants were included in each focus group. The composition of each focus group is published elsewhere.13 The highest proportion of older adults were female, white, had a graduate degree and self-reported having good health (table 2). Based on the study objectives, four major themes emerged from the focus group.
Descriptive statistics of the study population (n=57)*
First, older adults' perceived the CEPSS to have certain advantages and disadvantages in evaluating and comparing pharmacies. Second, older adults thought the CEPSS was important in choosing the best pharmacies and avoiding the worst pharmacies. Third, older adults perceived the CEPSS would be influential in their decision to choose a pharmacy. Fourth, older adults' perception of the CEPSS influence in switching pharmacies varies depending on the individual's personal experience or trust of other consumers' experience. Additional themes are also described.
The study's overall findings are grouped based on the objectives of the study.
Objective 1: The objective was to describe older adults' perceptions of evaluating and comparing pharmacies based on the CEPSS.
Major theme 1: Older adults perceived the CEPSS to have certain advantages and disadvantages in evaluating and comparing pharmacies. Some older adults supported the use of CEPSS to evaluate and compare pharmacies because many health services are compared in the market place and the evaluation would have a salutary effect on pharmacies that were initially rated as low quality (table 3).
I think it's very useful. They rate hospitals nationwide. You can go and look up how your hospital rates. I think you should be able to do that for your pharmacy.
Everybody would get better or do the job better knowing somebody is watching over them. I think they would do a better job if they know somebody out there is watching over them and grading them.
Older adults' perception of evaluating and comparing pharmacies based on the Consumer Experience with Pharmacy Services Survey (CEPSS)
On the other hand, some older adults were not supportive of using the quality domains to evaluate pharmacies because it was not based on quantifiable clinical indicators of quality but based on subjective information.If you're real unhappy cause you have to wait [in line], go to a different pharmacy! But the only important thing to get out of a pharmacy is the proper medication and the cost and those are the only two things that are life and death, just as in a hospital. The service you get, whether you're going to get an infection, whether you're going to get a pharmacist who has a poor record…those are the important things, whether they make errors and whether their cost is prohibitive.
Additional minor themes were identified:
Credibility of the quality information was an important consideration in the use of CEPSS as a quality metric for pharmacies. Older adults stated that their trust (credibility) of the quality information would depend on the information source, timeliness of the information, and whether the quality information was based on the CEPSS or other objective quantifiable data. Verbatim statements included:
Credibility of the information
Who's doing the judging…? Because you get all kinds of commercial interests involved, and public interests involved, and government interests involved.
If they're going to be rated, then we have to look at who's doing the rating. If it's the customer that would be one thing, if it's some outside source that knows what they're looking for but may not have a direct relationship, that's another thing.
Timeliness of the information
How are you going to have it be accurate by the time it would get in the hands [of patients], because any self-respecting pharmacist is going to try and fix whatever the problem is.
CEPSS versus objective data
Subjective information, that's a problem. However, there are certain factual things [that could be included in a quality report]. I had a pediatrician when my children were little…He said, ‘I have called every pharmacy in [town name] with the ten prescriptions I most often prescribe. And, they’re cheaper here, they’re more expensive there.’…The idea that a doctor actually took the time to find out what his patients were having to pay for the same medication from place to place, that was really a fine thing that he did. That's the kind of research that's factual.
Older adults also suggested that a valid and transparent report on pharmacy quality would need to say:Who's doing the evaluating, what are the actual criteria on which they're being evaluated…It would help you determine whether this report is valid.
What's the standard [used for evaluating]? What does selection mean or what does attention [to customers by pharmacy staff] mean?
Other minor themes: Dissemination of a quality report containing CEPSS information was important to older adults in using the survey domains.
Older adults volunteered some thoughts on how often the quality report should be compiled, including how to structure the report, and means and locations for wide dissemination including the internet, pharmacies, doctors' offices and American Association of Retired Persons (AARP) magazines. Verbatim statements included:
Compilation of quality report
You would have to do this [report] fairly often [because lower-ranking pharmacies would improve right away].
Structure of quality report
I think there’s two different ways it could be done. You can rate the individual stores or you could rate (Chain Pharmacy A) versus (Chain Pharmacy B), like the whole corporation and I think it would have greater value rating the individual stores but that would be harder to do.
Dissemination location for quality report
If you can go by the internet and see—at the pharmacy that I go to, for example, I can enter in the webpage and see if they have a good evaluation.
I think a report should be included with your prescription. When you go there to pick it up, the pharmacist should say, ‘Here is a report’.
I would love to have my doctors know which pharmacies are really doing well so that when…I’m in the office [and]…they’re going to prescribe a new medication, they could say, ‘We know that the following three pharmacies not only routinely stock this but are charging a reasonable price for it.’ Now, that doesn’t say that's where you have to go. But, I’m not having to get to my pharmacy, which is a small one, and suddenly find out that we’re going to have to wait a few hours for them to get it to me.
I think, since everybody here gets AARP, that would be a real good way, because everybody usually goes through the magazine here or the book that you get and knowing that they’re behind this 100%, which they should be, since they are doing more representation of the older population.
One other way you could get it around is to have in newspapers and on TV that it is available and here is who you contact to get it. If you don’t have a computer you can do that by mail and if you do you can request it on the Internet.
Objective 2: The objective was to describe older adults' perceived importance of the CEPSS and its specific domains.
Major theme 2: Older adults thought the CEPSS was important in choosing the best pharmacies and avoiding the worst pharmacies (table 4).
It rules out the worst case scenarios for you. If you’ve got eight to pick from, I would go with the top three…I wouldn’t do the one that has poor, poor, poor, on the categories so that way at least you can narrow the field down.
Older adults’ perceived importance of the Consumer Experience with Pharmacy Services Survey (CEPSS)
While all the CEPSS domains were important, some older adults strongly supported specific domains compared to others—that is, health and medication-focused communication and pharmacy staff communication were both perceived as the most important quality domains. These results are further confirmed in our questionnaire results.I think medication-related communication is the most important and as [participant name] says it's the main purpose of the pharmacy…Anything else is extra.
I don’t count on the pharmacist as the expert about my health. And, if I have a medication-related communication, I might ask the pharmacist but I’m more likely to look it up online or go through My Chart (a secure online service that allows a patient to communicate with their healthcare provider) with my general practitioner. But, being treated with respect by the pharmacy staff is very important.
Objective 3: The objective was to explore older adults' perceptions of the influence of specific CEPSS domains in choosing/switching pharmacies.
Major theme 3: Older adults perceived the CEPSS would be influential in their decision to choose a pharmacy (table 5).
The first one [pharmacy] that I was going to, to get my prescriptions, it was because of convenience. But then the staff wasn’t as friendly and they didn’t ask you questions, and then somebody recommended someplace else but it was inconvenient. But it turned out…it was worth the inconvenience, because the staff there was really concerned and I wasn’t afraid to ask them questions.
Older adults’ perceptions of the influence of the Consumer Experience with Pharmacy Services Survey (CEPSS) in choosing/switching pharmacies
However, some older adults would rather use price and pharmacy medication safety information to choose pharmacies instead of the CEPSS.As long as they can give me the right medication I don’t give a hoot. I go where the price is right and I don’t care actually if they have the best price if the pharmacist frowns at me every time…I don’t care if they say hurry up and get out of here. I don’t care as long as their price is right…as long as they are competent…no errors. None of these [CEPSS domains] are related to the pharmacy giving you the wrong darn pill.
Major theme 4: Older adults' perception of the CEPSS influence in switching pharmacies varies depending on the individual's personal experience or trust of other consumers' experience (table 5).
Some older adults would switch pharmacies because CEPSS information is based on other consumers' experiences. Other older adults would place greater importance on their own personal pharmacy experiences than other consumers' experiences.I don’t think I would change pharmacies if my own personal experience were good in all those areas…and others might’ve had a bad experience.
When the older adults discussed what specific CEPSS domain would cause them to switch pharmacies if their pharmacy rated low, health and medication-focused communication and pharmacy staff communication were more frequently described as the quality domains that would cause them to switch their pharmacies.I take 17 different prescriptions. And, if I couldn’t depend on them (the pharmacy) to have accurate… information or the actual medication part of it, if I couldn’t trust that, then, I guess, I would have to consider changing.
You can ask about anything you want to if you have a good communication with staff. If you don't have a good communication with the staff, I feel like you're lost, absolutely lost. So… If I was missing that, I'd go someplace else.
Questionnaire results—importance of the specific CEPSS domains and its use in choosing/switching pharmacies
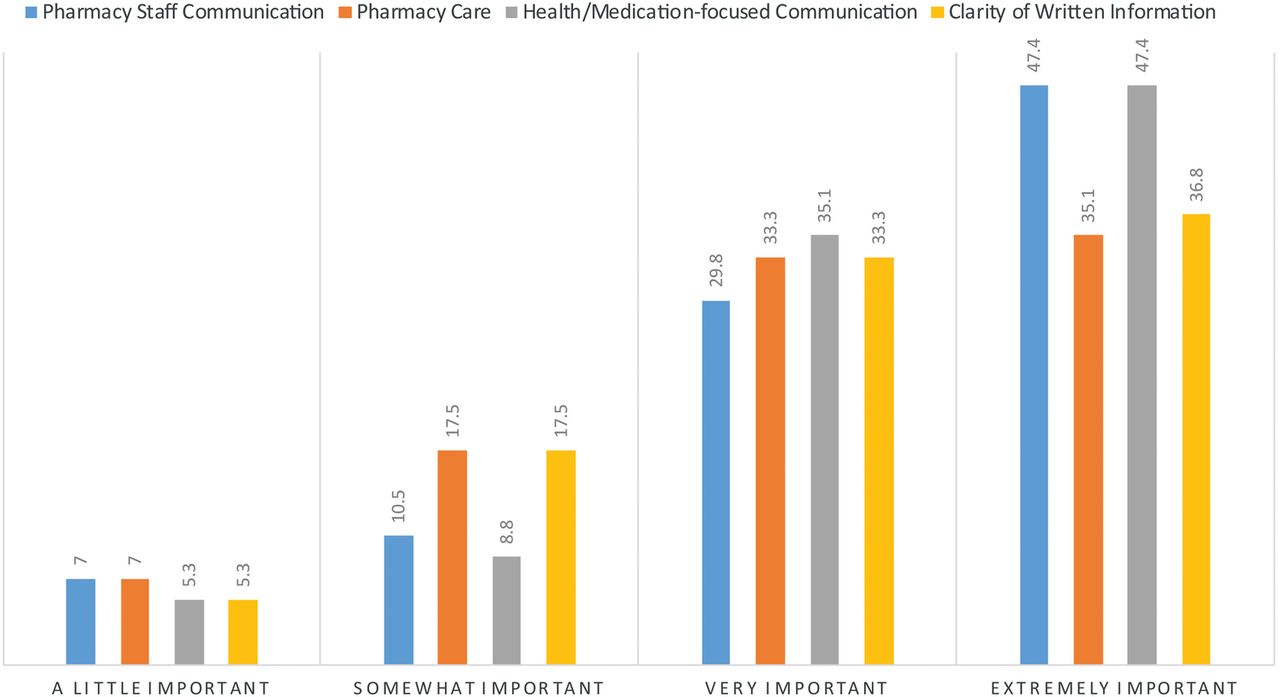
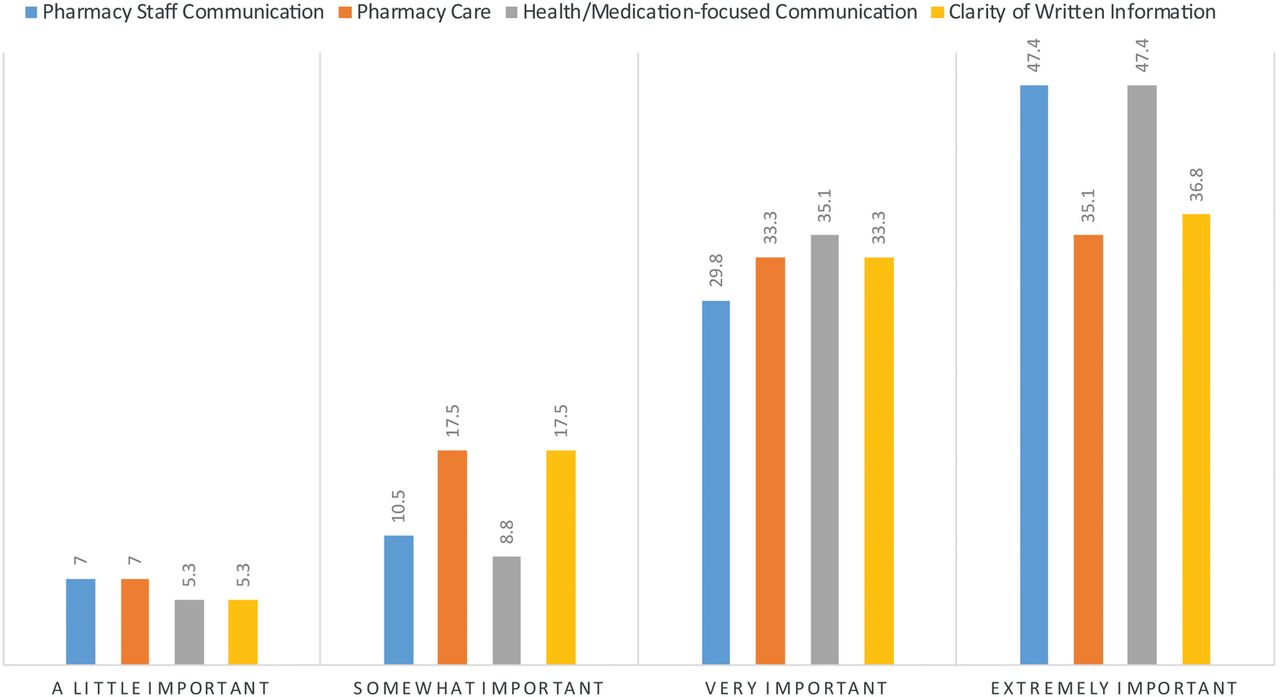
Fifty-seven participants completed a questionnaire. Three participants had missing data. Patients reported that all the CEPSS domains were extremely important in evaluating and comparing pharmacies. The largest percentage of older adults thought pharmacy staff communication (n=27, 47.4%) and health/medication-focused communication (n=27, 47.4%) were extremely important in evaluating and comparing pharmacies. None of the older adults chose the ‘not at all important’ response option for any CEPSS domain (figure 1).

Older adults likelihood of changing pharmacies if pharmacy had low rating in Consumer Experience with Pharmacy Services Survey (CEPSS) quality domain (N=57).
Overall, low ratings in all the CEPSS domains were likely to lead to a change in pharmacy. Twenty-one participants (36.8%) reported being extremely likely to change their pharmacy if it had low ratings in health/medication-focused communication. The lowest percentage of older adults (n=12, 21.1%) would be extremely likely to change their pharmacy if their pharmacy reported low ratings in pharmacy staff communication (figure 2).
{kind=link}
{kind=link}
Older adults perceived importance of Consumer Experience with Pharmacy Services Survey (CEPSS) quality domains in evaluating and comparing pharmacies (N=57).
Discussion
This study showed that older adults perceive the CEPSS as important in evaluating and comparing pharmacies. Pharmacy quality information based on the CEPSS is likely to influence older adults' pharmacy selection in varied circumstances. The pharmacist's communication about medicines and health is perceived as the most important domain within the CEPSS. Low ratings in this domain are also likely to influence older adults' pharmacy choice and to lead to a possible switch in pharmacy.
Older adults thought that the use of the CEPSS to evaluate and compare pharmacies had certain advantages and disadvantages. This result is consistent with research showing how patients use data from the CAHPS survey in evaluating health plans and hospitals.23 ,24 In the current study, some older adults supported the CEPSS because many health services were already compared in the market place and they perceived that an evaluation would have a beneficial effect on initially low-rated pharmacies. Hibbard et al,28 showed that publicising hospital performance information led to higher quality among hospitals whose performance were initially low. Currently, there is no conclusive evidence of the effect of quality reports on improved quality of healthcare services. Schauffler and Mordavsky,29 reported that the public reporting of provider performance information did not affect patients' decision-making, or lead to provider competition and improved quality care. This result might vary by the type of healthcare service being received. For example, in a systematic review, it was concluded that public reporting stimulates quality improvements in hospitals.18 However, in the same review, it was reported that its effect in stimulating quality among health plans is mixed.18 Future research needs to examine whether publicly available pharmacy quality information stimulates quality improvement in ambulatory care pharmacies.
Some older adults were not supportive of using the CEPSS to evaluate pharmacies because the CEPSS is not based on quantifiable objective indicators of quality but rather on subjective information compiled from patients. Patients have been reported neither to understand30 nor to use objective quality metrics, in their healthcare decision-making.9 ,31 Also, no comparative pharmacy information based on objective quality metrics are presently being publicly reported to patients. Objective quality metrics like the ‘high-risk medication in the elderly’ can be used by older adults to differentiate high-quality pharmacies from low-quality pharmacies. Efforts to disseminate this information to older adults as a mechanism for them to choose quality providers when they are seeking care is needed urgently.
Older adults will use the CEPSS to avoid the worst pharmacies. In a previous study, patients stated that they were likely to use quality information to avoid poor quality providers, rather than to seek out the best quality provider.11 ,32 This result has implications for older adults. Older adults use a lot of medicines and possibly need pharmacists' help with medication management. It is important to educate older adults that they need to actively seek quality care. Quality information should not only be used when they are disappointed with their current provider. The public reporting of pharmacies' CEPSS information will enhance older adults' active process of seeking high-quality pharmacies. With access to quality information, patients will be aware of the variation in the quality of pharmacies, they will increasingly become selective of the pharmacy they visit to fill their prescriptions and get their care, and pharmacies will make performance improvements to stay competitive.3
In the selection of a pharmacy, older adults would likely use the CEPSS to finalise their decision-making when choosing between several pharmacies. This is somewhat promising. Previous research shows that the reputation of a healthcare provider,4 price33 and family/friends referrals9 ,34 are factors patients use in choosing a healthcare provider. Also, location and convenience have historically been important and used by patients in the initial selection of a pharmacy.35 ,36 However, this current study showed that when the choice of pharmacies has been narrowed down, quality information might be used in making the final decision.
Though older adults think the CEPSS is important, some participants would still rely on their personal experience rather than the survey. Specifically, some older adults preferred to use their own experience in judging quality, rather than the experience of others. This was surprising since the CEPSS is based on other patients' personal experience and one would expect older adults to actively use this information to choose their pharmacies. On the other hand, it was encouraging to know that some older adults would rely on the evaluations of their peers in changing pharmacies. Past research shows that patients value other consumers' evaluation of their healthcare experience.37 Patients like to use satisfaction measures in decision-making, especially if the responses are from people like themselves who are making similar choices.38 This finding further shows the potential value of publicly reporting pharmacy quality information based on the CEPSS. Future research should consider the appropriate format and/or content of comparative pharmacy quality information.
Older adults perceive that they would need to have a personal negative experience before they would switch their pharmacy based on the CEPSS. Patients who viewed physician performance information reported the likelihood of changing physicians if he/she performed badly in a quality report.39 Previous studies have showed that when patients are satisfied with the care they receive from their healthcare provider, they become loyal and less likely to switch.40 ,41 Usually, it takes having a number of bad experiences before consumers would feel dissatisfied and possibly switch their pharmacy.40 If older adults wait to have a negative experience in their pharmacy before a decision to seek a higher quality pharmacy is made, a preventable negative medication adverse effect might occur and lead to serious consequences. Owing to the multiple chronic conditions and high number of medicines used by older adults, they are more likely to need additional care from their pharmacist. Older adults are more prone to preventable adverse events and should therefore seek quality providers in their care.
The focus groups and questionnaire results from this study showed that all domains within the CEPSS were considered important. However, based on participants' questionnaire ratings, there was variability in patient perceptions of the importance of each specific CEPSS domain. The questionnaire results confirmed that health/medication-focused communication and pharmacy staff communication were the most important specific CEPSS domain. These results are not surprising. Hassel et al,26 showed that patients use community (retail) pharmacies because they perceive the pharmacy staff to be experts on medicines, have time to talk compared with their doctors and generally are more approachable than their doctors. In a previous study of lay consumers' perception of clinical quality measures, the relationship with the pharmacist was an important factor favoured over the use of clinical quality measures in choosing a pharmacy.8 Franic et al,42 also showed that service-related features determined the pharmacy that patients chose to fill their prescriptions. Their study results highlighted the value of the pharmacy staff and pharmacists in patients' pharmacy decision-making process.42 Using the CEPSS, pharmacies can highlight their communication skills in providing medication information, including their friendliness and caring attitudes.
Based on the questionnaire results, a pharmacy's low rating in health/medication-focused communication was extremely likely to cause a switch in pharmacy. Whitehead and colleagues observed that patients who used pharmacies with insufficient provision of medication information wanted a pharmacy with better information about medicines. These individuals were also likely to use this factor to choose their pharmacies.41 If the amount of medication information that is provided to patients is likely to influence their pharmacy choice, then it is important for pharmacies to publicise their CEPSS results as a way of increasing their patronage by other patients. The questionnaire results showed pharmacy staff communication was perceived as extremely important in evaluating pharmacies, yet a lower proportion of participants considered it extremely likely that this domain would prompt them to change pharmacies. We hypothesise that while patient–provider communication is important in enhancing patient's satisfaction with pharmacy services, patients may place a higher value in the safe administration of their medicines (reflected in their responses to the importance of health and medication-focused communication, clarity of written information, and pharmacy care) because it may be linked directly to improved health and medication use outcomes, and a reduction in medication errors.
Older adults reported that the credibility of the quality information was an important consideration in the use of CEPSS as a quality metric for pharmacies. These results are similar to a previous study of clinical pharmacy quality measures among patients with chronic illnesses.11 In addition, Hibbard et al's24 proposed consumer choice model has reported a lack of trust in quality information as a barrier to the use of such information in patients' decision-making.2 To enhance the use of CEPSS in patients' pharmacy choice, a credible source needs to be used in the communication of this quality information.
The older adults in this study thought that the internet, the doctor's office, AARP magazines and mass media communications were portals that could be used in disseminating pharmacy quality information. According to the consumer choice model, patients need to be aware of the availability of quality information before it can be used in their decision-making.24 Hence, the information on these possible dissemination avenues is vital to the publicising of pharmacy quality information and the use of CEPSS by older adults.
This study had some limitations. A convenience sampling approach was used in the recruitment of older adults. Our sample was predominantly female and well educated. Participants' health literacy was not addressed and will need to be examined in the future. Inter-rater reliability between the two authors who coded the data was determined by consensus and not by statistical analysis. The discussion of the CEPSS domains during the focus group might have impacted the questionnaire results. The CEPSS was developed and validated in 2007. Hence, the pharmacy services represented in the survey may not adequately represent changes in types of services increasingly offered in ambulatory pharmacy including preventative health screening, immunisation and medication therapy management services, etc. The survey may need to be revalidated prior to distribution. Also, we did not explore the question of how CEPSS data might be collected and who would pay for it.
Conclusion
The CEPSS may be important and influential as a quality metric in older adults' pharmacy choice. The older adults in this study would use information related to the pharmacist's communication about health and medicines in their decision to switch pharmacies. Pharmacies should consider using and publicly reporting CEPSS information as a means of publicising the quality of care provided to consumers.
Acknowledgments
The authors would like to acknowledge the Community Academic Aging Research Network (CAARN) for helping with the recruitment of older adults into the study. The project described was supported by the Clinical and Translational Science Award (CTSA) programme, through the National Institute of Health (NIH) National Center for Advancing Translational Sciences (NCATS), grant UL1TR000427.
References
Footnotes
Contributors OOS and DAM designed the study. OOS and KDC were involved in data collection and data analysis. OOS and KDC wrote the manuscript and DAM critically revised the content. All authors approved the final version of the manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sector.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Education and Social/Behavioral Science Institutional Review Board of the University of Wisconsin-Madison.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.