Article Text

Abstract
Objectives Papillomavirus Dumfries and Galloway (PaVDaG) assessed the performance of a high-risk human papillomavirus (hrHPV) PCR-based assay to detect high-grade cervical intraepithelial neoplasia (CIN2+) in self-collected vaginal and urine samples.
Setting Women attending routine cervical screening in primary care.
Participants 5318 women aged 20–60 years provided self-collected random urine and vaginal samples for hrHPV testing and a clinician-collected liquid-based cytology (LBC) sample for cytology and hrHPV testing.
Interventions HrHPV testing. All samples were tested for hrHPV using the PCR-based cobas 4800 assay. Colposcopy was offered to women with high-grade or repeated borderline/low-grade cytological abnormalities; also to those who were LBC negative but hrHPV 16/18 positive.
Primary and secondary outcome measures The self-tests' absolute sensitivity and specificity for CIN2+ were assessed on all biospecimens; also, their relative sensitivity and specificity compared with clinician-taken samples. Interlaboratory and intralaboratory performance of the hrHPV assay in self-collected samples was also established.
Results HrHPV prevalence was 14.7%, 16.6% and 11.6% in cervical, vaginal and urine samples, respectively. Sensitivity for detecting CIN2+ was 97.7% (95% to 100%), 94.6% (90.7% to 98.5%) and 63.1% (54.6% to 71.7%) for cervical, vaginal and urine hrHPV detection, respectively. The corresponding specificities were 87.3% (86.4% to 88.2%), 85.4% (84.4% to 86.3%) and 89.8% (89.0% to 90.7%). There was a 38% (24% to 57%) higher HPV detection rate in vaginal self-samples from women over 50 years compared with those ≤29 years. Relative sensitivity and specificity of hrHPV positivity for the detection of CIN2+ in vaginal versus cervical samples were 0.97 (0.94 to 1.00) and 0.98 (0.97 to 0.99); urine versus cervical comparisons were 0.53 (0.42 to 0.67) and 1.03 (1.02 to 1.04). The intralaboratory and interlaboratory agreement for hrHPV positivity in self-samples was high (κ values 0.98 (0.96 to 0.99) and 0.94 (0.92 to 0.97) for vaginal samples and 0.95 (0.93 to 0.98) and 0.90 (0.87 to 0.94) for urine samples).
Conclusions The sensitivity of self-collected vaginal samples for the detection of CIN2+ was similar to that of cervical samples and justifies consideration of this sample for primary screening.
- PRIMARY CARE
- PUBLIC HEALTH
- SEXUAL MEDICINE
- VIROLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Population-based using simple vaginal swabs and random urine samples compared with clinician-taken cervical (liquid-based cytology) samples.
Comparator test was a validated PCR-based assay on a cervical sample, also applied to the self-taken samples.
Reliability of gold standard (colposcopy and histology) assured by consistency of national screening protocol and practices.
Constrained by ethics from undertaking colposcopy in patients who were high-risk human papillomavirus positive in only their self-samples.
Not feasible to optimise the urine sample collection and assay for this study.
Introduction
Global evidence indicates that high-risk human papillomavirus (hrHPV)-based screening is more effective than cytology in reducing the incidence of cervical precancer/cancer1 ,2 using clinically validated hrHPV assays.3 ,4 This is based on the higher sensitivity of hrHPV testing compared with cytology for the detection of high-grade cervical intraepithelial neoplasia (CIN2+) and the scope for extended screening intervals. Accordingly, a clinically validated hrHPV assay on a cervical sample rather than cytology is becoming the preferred policy for cervical cancer screening. Self-taken samples also provide an opportunity to reach women who do not otherwise attend,5–7 although concerns about the quality of samples have been reported.8 ,9
There is a growing body of evidence on the analytical and clinical performance of different assays for detection of hrHPV as well as assessment of devices designed to aid self-collection. The absolute specificity of self-collection tests as assessed in a colposcopy clinic is irrelevant for primary screening, although relative test performance can be assessed with little bias and the need for verifying that women with a negative screening test are truly free from disease.10 A meta-analysis of the clinical accuracy of vaginal self-sampling for CIN2+ detection, assessing studies on these principles, found acceptable sensitivity and specificity of self-vaginal samples if validated PCR-based HPV tests were used.11 That conclusion was swayed by a Chinese study12 whose multiplex primary PCR assay did not meet guideline standards for assay reproducibility. There is, to date, no published primary screening study of self-testing using a fully clinically validated assay.
Compared with self-taken vaginal samples, urine sampling offers a less invasive option and it has been reported that women favour this approach to cervical and/or vaginal sampling.13 ,14 Studies of hrHPV detection in urine have been mainly assessed on virological outcomes and only partially address clinical accuracy.15–17
Advantages of self-sampling for women are multiple, yet studies on performance have been derived mainly from women who default from traditional screening.5 Since molecular hrHPV testing rather than cytology will be the method of primary cervical screening for the future, assessment of self-sampling in the general population of eligible women becomes apposite. Self-sampling should be simple and inexpensive.
Our objective was to determine the clinical performance of hrHPV testing in self-samples (urine and vaginal swabs) taken by women attending cervical screening as part of a national programme. We aimed to validate self-sampling for routine cervical screening.
Methods
Setting and recruitment
Papillomavirus Dumfries and Galloway (PaVDaG) is a population-based screening study in a region of Scotland with 160 000 inhabitants served by 40 general practice clinics. All women, other than those previously diagnosed with CIN2+, presenting for routine cervical screening (April 2013 to July 2014) were invited to consent to the study. In Scotland, women receive their first invitation to cervical screening in the year of their 20th birthday (including a ‘catch up’ HPV-vaccinated cohort) and their last invitation in the year of their 59th birthday.
Participants first provided a random void urine (if unable to, they were encouraged to hand that in later), then self-collected a vaginal sample prior to a routine cervical sample being collected by the clinician. We followed all recalls for cytology and colposcopy relevant to this screening round for a minimum of 8 months from enrolment.
The study was conducted over one round of primary cervical screening in Dumfries and Galloway, Scotland. Clinical performance of self-sampling for the detection of CIN2+ was assessed, as was the relative accuracy of the vaginal and urine samples compared with the clinician-taken cervical sample. The analytical range (cycle threshold (Ct)) values of the three biospecimens were also assessed as was the interlaboratory and intralaboratory agreement for all self-specimens. Finally, the impact of age on hrHPV detection in self-samples was analysed.
Sample collection, processing and testing
Urine was collected in universal containers; in the laboratory, 6 mL was mixed with 3 mL of Roche PCR media (Roche Molecular Systems).
Self-collected vaginal samples were obtained using cobas PCR female swab sample packets (Roche Molecular Systems), validated for chlamydia/gonorrhoea (CT/NG) self-vaginal sampling. Women were advised to follow instructions printed on the collection kit. Swabs were immediately immersed in tubes containing Roche PCR media. Vaginal samples were vortexed for 30 s with the swab in situ, as per the protocol used for CT/NG, before testing.
In an early pilot phase, 200 patients used two swabs together for sampling, one immersed immediately in buffer as above, the other left dry for 28 days before immersion in the laboratory immediately prior to assay.
Cervical liquid-based cytology (LBC) samples were clinician-collected using a Rovers Cervex-Brush (Oss, the Netherlands) and suspended in 20ml of ThinPrep solution (PreservCyt Solution, Hologic, UK) as per routine practice. Three millilitre of LBC sample was aliquoted into a separate tube for HPV testing.
All three samples were tested with the cobas 4800 DNA HPV test using the standard procedure. This test is clinically validated and the Food and Drug Administration (FDA) approved for primary cervical screening using LBC samples4 ,18 and was our reference standard. This test is a real-time PCR fully automated method detecting separately HPV 16, HPV 18 and 12 other hrHPV types (HPV 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68) with the β-globin gene as an extraction and amplification control.
Sets of 520 vaginal and 526 urine samples were retested in the Dumfries laboratory and in the Coombe Women and Infants University Hospital, Dublin, Ireland, for intralaboratory and interlaboratory reproducibility. Collection and testing kits were supplied by Roche Global.
To determine the number of PCR amplification cycles (Ct values) needed to detect hrHPV DNA in the cobas assay, a randomly selected set of positive samples—376 cervical, 381 urine and 449 vaginal—was analysed.
Management of abnormal smears and ascertainment of CIN2+
Abnormal cytology results and histopathology reporting were according to the UK Cervical Screening Programme guidelines.19 Accordingly, participants with high-grade abnormalities were referred for colposcopy, while women with borderline changes or low-grade cytology were recalled for repeat cytology after 6 months. Women with two low-grade or three borderline smears were referred for colposcopy. Participants with an unsatisfactory smear were recalled for repeat cytology after 3 months. Three consecutive unsatisfactory smears or a subsequent abnormal smear resulted in referral for colposcopy.
For the PaVDaG study, all participants with normal cytology but a positive cervical hrHPV test (cyto−/hrHPV+) were invited for repeat hrHPV testing on all three samples after 4–6 months. Colposcopy was offered to cyto−/hrHPV+ women if they were positive for HPV 16 and/or 18 at their baseline and/or follow-up. To ascertain CIN2+ status, histological abnormalities were graded on the biopsies taken at colposcopy. In cases of significant disparity, a second pathology opinion was standard. Screening history, HPV vaccination and cytology results (past and current) were accessed through the Scottish Cytology Call-Recall System using the person-specific Community Health Index population register.
Sample size calculation
We assumed, on the basis of a published performance of the cobas 4800 assay,4 a sensitivity for CIN2+ of 96% and a specificity of 89%. Since this was a screening study, sensitivity rather than specificity was the driver of the sample size computation. A formula proposed by Tang et al20 was used to compute the sample size to address the hypothesis of equivalence of test performance in studies with a matched-pair design (multiple tests applied on the same participants). Under a worst case assumption7 for a PCR-based assay on self-samples that 5% of CIN2+ cases are positive on clinician samples but negative on self-samples and accepting a confidence level of 95% and a power of 80%, the required sample size was 83 CIN2+ cases. Anticipating a detection rate of CIN2+ of 1.7%21 in the population gave a sample size estimate of 4882—rounded up to 5000.
Ethical approval
The study was sponsored by National Health Service (NHS) Dumfries and Galloway and approved by West of Scotland Research Ethics Service. An important prerequisite of approval was that the study should not compromise in any way (or raise public concern about) the effectiveness of standard screening. Women were informed about their hrHPV results after having received the standard information based on their cytology. This demanded a particularly sensitive interchange with patients whose positive hrHPV results were in a setting of negative cytology. To limit the burden of follow-up and risk of overdiagnosis, we focused only on patients positive for HPV 16 and 18 (but not other) types in their cervical sample. It was deemed inappropriate to press for colposcopy in participants positive for hrHPV in only their vaginal and/or urine self-samples, who had normal cervical cytology and were HPV negative in their cervical sample.
Statistical analysis
The primary outcome measure was sensitivity and specificity of the assay in cervical and self-collected samples to detect CIN2+. This analysis was based on hrHPV test results at the initial visit; all cervical and self-test samples with a failed hrHPV result were excluded from analysis. Where only vaginal and/or urine samples were hrHPV positive in this first sample, the calculation was of inferred sensitivity and specificity as these findings in isolation did not permit referral for colposcopy and histological grading.
Absolute specificity could not be assessed directly from this study since it is not feasible to submit all screen test-negative women to gold standard verification.10 We assumed that women with no history of CIN2+ and two previous consecutively negative cervical cytology results (for women <23 years, this precondition was necessarily restricted to one previous negative cytology) did not have underlying cervical precancer. This proxy definition of disease outcomes, combined with the use of a highly sensitive and fully validated HPV test, reduces the consequences of verification bias.10 ,22 ,23 Moreover, even if some verification bias would have affected the estimation of the absolute accuracy measures, the relative sensitivity and specificity would not be affected given the PaVDaG design.
The relative accuracy of hrHPV test results in vaginal and urine samples versus cervical samples was computed and 95% CIs were calculated according to binomial distributions. The χ2 test of McNemar was used to assess discordances. A χ2 test was used for linear trend.
Intralaboratory and interlaboratory reproducibility of the assay in self-samples was assessed by the κ statistic.
Outcomes in young women who had received at least two doses of vaccine were recorded separately.
Results
Participants
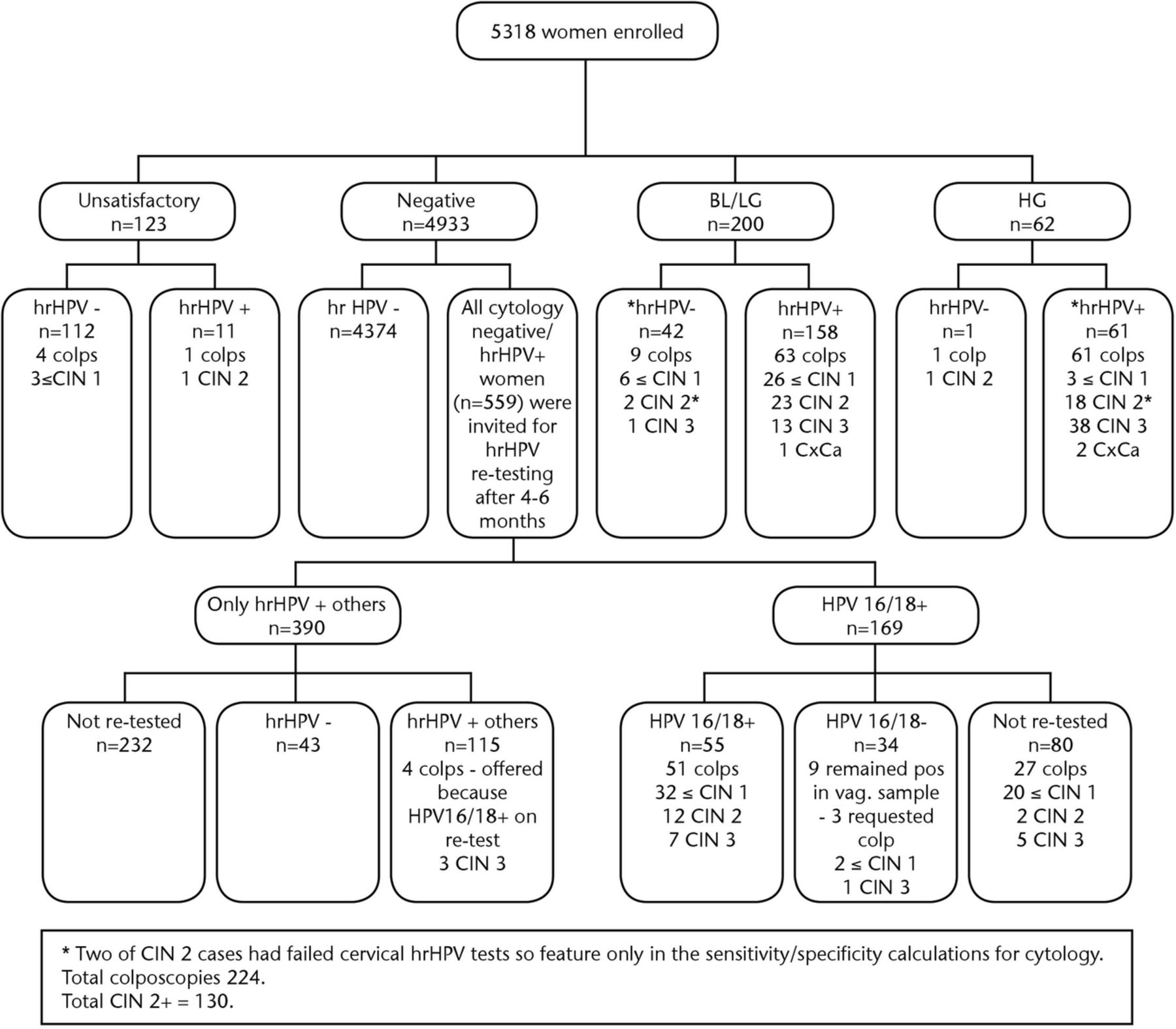
In total, 5318 women were enrolled. Mean age was 41.3 (18–76: median=46, <20=7 and >59=145); 97% belonged to the screening target age group 20–59 years. Of the women aged ≤23 years, 66% (354/533) had been vaccinated with at least two doses of the bivalent HPV vaccine. The flow chart of cervical hrHPV detection, cytology results and detection of CIN2+ lesions is presented in figure 1.

Cytology and hrHPV results with corresponding colposcopies and histological outcomes. Cytology results reported as: negative (normal); unsatisfactory (inadequate); BL (ASCUS)/mild dyskaryosis=LG and moderate/severe dyskaryosis=HG. Histology results reported as CIN grade <CIN1 (neg or CIN1), CIN2 or 3 (note: CIN3 includes two cases of glandular CIN) and cervical cancer (CxCa; three cases of adenocarcinoma). BL, borderline abnormality; CIN, cervical intraepithelial neoplasia; colp, colposcopy; HG, high grade; hrHPV, high-risk human papillomavirus; LG, low grade.
Cytology
The prevalence of abnormal cytology was highest in women aged ≤24 years (13.8% vs 4.9% overall), while high-grade abnormalities were most prevalent in women aged 25–29 years (3.4% vs 1.1%). This same group of women had the highest prevalence of CIN2+ lesions (8.0% vs 2.4% overall; table 1). The prevalence of abnormal smears decreased from 13.7% to 0.6%, while the proportion of unsatisfactory smears increased from 0.4% to 6.8% with increasing age. In the group of 122 women with unsatisfactory smears at baseline, 24 participants did not complete recall follow-up cytology; further screening of the remainder resulted in four colposcopies and one CIN2 lesion. Compliance with follow-up cytology after borderline/low-grade smears was 87%, resulting in 72 colposcopies associated with 40 CIN2+ lesions. All 62 women with high-grade smears had colposcopy, which was associated with 59 CIN2+ lesions (figure 1).
Prevalence of cytological abnormalities, unsatisfactory smears and histologically confirmed high-grade cervical intraepithelial neoplasia by age group
HPV prevalence in self-taken versus clinician-taken samples and influence of prior vaccination and age on detection.
HrHPV was detected in 14.7%, 16.6% and 11.6% of cervical, vaginal and urine samples, respectively, with HPV 16/18 in 4.9%, 5.5% and 3.1% of the respective samples (table 2).
Age-specific distribution of Cobas 4800 HPV detection in all three samples presented in numbers and per cent
Positivity in cervical samples from HPV-vaccinated versus non-vaccinated women was 127/354 vs 81/179, yielding a calculated relative risk of 0.79 (95% CI 0.64 to 0.98; p=0.0361). However, there was a greater difference for HPV16/18 detection, which was 29/179 in non-vaccinated compared with 10/354 in vaccinated women; relative risk 0.17 (95% CI 0.09 to 0.35, p<0.001).
Prevalence of hrHPV positivity in participants aged ≥25 years was 11.3%, 13.1% and 9.0% in cervical, vaginal and urine samples, respectively. The decrease in hrHPV detection by age was smaller in vaginal samples compared with cervical samples with a significant increase in relative test positivity in older women. The proportion of hrHPV-positive results was similar in cervical and vaginal samples in women aged ≤29 years. Comparatively, hrHPV positivity was 38% (24–57%) higher in vaginal compared compared with cervical samples in women aged ≥50 years. This was also reflected in HPV16/18 positivity, which was 26% higher in vaginal samples compared with cervical samples in women aged ≥50 years. The increase from 1.01 to 1.38 with increasing age showed a significant linear trend (p=0.03; figure 2A). Similarly, the ratios of hrHPV positivity in urine versus cervical samples increased from 0.66 to 0.95, with a significant linear trend (p=0.02; figure 2B). Of the 76 women over 50 years who were hrHPV positive in their cervical samples, 72 (95%) had provided ‘screening’ urine samples which were also hrHPV positive.
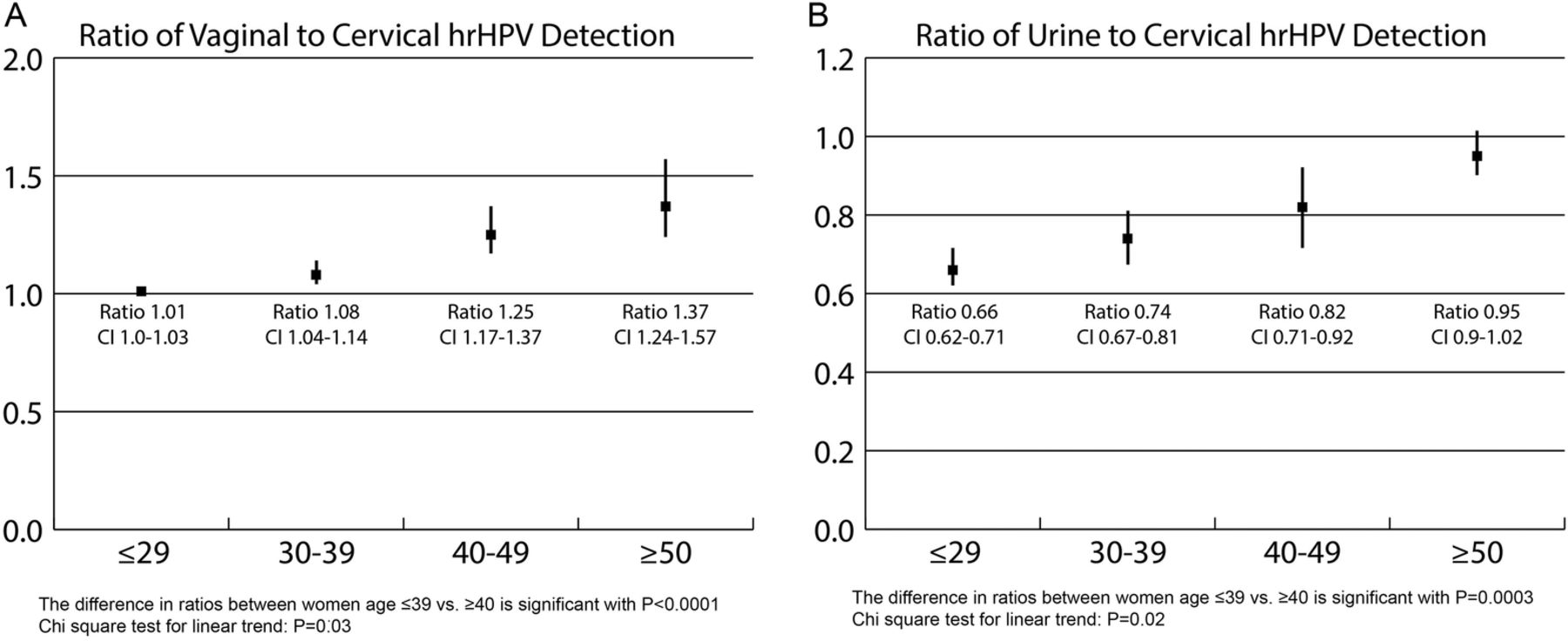
(A, B). Age-specific relative increase of cobas 4800 HPV detection in vaginal versus cervical and urine versus cervical samples corrected for no samples/no HPV results for each type of sample. This is presented as a ratio of hrHPV+ vaginal/hrHPV+ cervical and hrHPV+ urine/hrHPV+ cervical samples with corresponding 95% CIs. hrHPV, high-risk human papillomavirus.
Analysis of the average number of PCR cycles needed to detect hrHPV DNA (Ct values) indicated higher values for the urine samples than for cervical or vaginal samples (figure 3). The cut-off set is approximately 40 cycles (Ct<40), but in a number of urine samples hrHPV DNA would have been detected had the cut-off level been extended to 45 cycles.

{kind=link}
{kind=link}
{kind=link}
The distribution of ct values (cycling time=number of PCR cycles needed to detect hrHPV DNA) observed in PCR hrHPV DNA amplification using cobas 4800 assay in three samples. hrHPV, high-risk human papillomavirus.
In the pilot study of vaginal self-samples using 200 dry swabs immersed in buffer at 0 and 28 days, there was a reasonable concordance (κ 0.693) in HPV positivity in the 176 pairs for which full results were available. Nine swabs were positive only on the day of collection and immersion against 16 only positive when immersed and assayed at 28 days.
Sensitivity and specificity of self-sampling for the detection of high-grade cervical lesions.
A total of 130 CIN2+ lesions were diagnosed during the study (3 cervical cancers, 68 CIN3, 59 CIN2 lesions; table 1). The CIN2+ lesions were detected as a consequence of 137 routine colposcopies (yielding 100 CIN2+ lesions) and 85 colposcopies (yielding 16 CIN3 and 14 CIN2 lesions) performed according to study-driven indications. Twenty seven of these were requested by patients in preference to further hrHPV testing (figure 1). Colposcopic assessment alone was deemed normal in 11 cases, and four patient biopsies were considered ungradeable.
With respect to hrHPV detection for CIN2+, cervical samples (n=5299) had the highest absolute sensitivity of 97.7% (95% CI 95.0% to 100.0%); the inferred sensitivity of vaginal samples (n=5208) was 94.6% (95% CI 90.7% to 98.5%) and for urine (n=5003) 63.1% (95% CI 54.6% to 71.7%). As to specificity, the absolute value of cervical results for detection of CIN2+ was 87.3% (95% CI 86.4% to 88.2%), the inferred values being 85.4% (95% CI 84.4% to 86.3%) for the vaginal samples and 89.8% (95% CI 89.0% to 90.7%) for the urine self-samples, respectively. All these results, with the corresponding figures for CIN3+, are summarised in table 3.
Absolute sensitivity of hrHPV testing on cervical, vaginal and urine samples and cytology to detect CIN2+ or CIN3+
The relative sensitivity and specificity of all samples are presented in table 4. HrHPV positivity on self-collected vaginal samples was comparable to that of clinician-collected cervical samples for detection of CIN2+ and CIN3+ lesions with relative sensitivity of 0.97 (95% CI 0.94 to 1.00) and 0.97 (95% CI 0.93 to 1.00), respectively. This was achieved with little compromise in relative specificity, which was 0.98 (95% CI 0.97 to 0.99).
Relative sensitivity and specificity estimates, 95% CI and p values for difference in matched proportions
Intralaboratory and interlaboratory agreement of cobas 4800 HPV detection using self-sampling.
Intralaboratory agreement of hrHPV positivity was 99.8% (95% CI 98.9% to 100.0%) and 98.1% (95% CI 96.5% to 99.1%) with κ values of 0.98 (0.96 to 0.99) and 0.95 (0.93 to 0.98) for vaginal and urine samples, respectively. Similarly, interlaboratory agreement was 97.8% (95% CI 96.2% to 98.8%) and 96.1% (95% CI 94.1% to 97.5%) with κ values of 0.94 (0.92 to 0.97) and 0.90 (0.87 to 0.94) for vaginal and urine samples, respectively.
Discussion
The study has shown that in routine cervical screening, self-collected vaginal samples are comparable to clinician-collected cervical samples for the detection of CIN2+ by hrHPV testing. Vaginal sampling increased detection of hrHPV by approximately 2%. Relative sensitivity and specificity of vaginal versus cervical samples for detecting CIN2+ was 0.97 and 0.98. Scotland offers screening to women aged 20–60 years, so the study population is slightly younger than in other screening programmes. However, when sensitivity and specificity of the self-vaginal samples in women aged ≥25 years was compared with that in women aged ≥30 years, the conclusions were fundamentally unchanged. This study provides important original data for the use of self-vaginal sampling in routine screening.
There are caveats to the analysis. First, the sensitivity of hrHPV testing could have been biased by the non-attendance of cyto−/hrHPV+ women for a follow-up hrHPV test. Assuming that this group had the same prevalence of CIN2+ as the attendees (figure 1), approximately 14 CIN2+ lesions may have been missed, which would have further reduced the observed sensitivity of cytology. Second, the accuracy of the hrHPV test in the self-taken samples may have been slightly underestimated as the study protocol did not offer women who were hrHPV+ in at least one of their self-samples (but not their equivalent cervical sample), a follow-up hrHPV test and/or referral for colposcopy. Indeed, some self-sample hrHPV-positive cases without follow-up may have contained CIN2+ (yielding some true positive cases currently considered as false positive). Third, hrHPV ‘other’ positivity in any sample was not, per se, an indication for further evaluation. However, analysis of hrHPV distribution indicated that the 12 hrHPV types other than the HPV16/18 group were evenly distributed through the self-sample and cervical groups.
A key strength of this study is that it was population based, used a widely accepted reference standard and intercalated with the primary screening services within an entire Scottish health board. The UK national screening programme requires consistency of practice and protocol across all its aspects—ensuring that variation in local practice is likely to be less than that associated with opportunistic programmes.
Sensitivity of hrHPV testing for CIN2+ using urine samples was significantly lower than the cervical and the self-taken vaginal samples. However, we cannot dismiss completely the potential of urine sampling for hrHPV testing on the basis of our data. We used random void samples collected in vials with no preservative. The cobas 4800 assay cut-off was applied with cervical samples in mind and adjustment of the cut-off for urine samples (as shown in figure 3) may considerably enhance sensitivity. Preliminary analysis of Ct values in the present study suggested that sensitivity for detection of CIN2+ could be increased to approximately 78% if the cut-off was increased to 45 PCR cycles. Should urinary HPV, for cultural or cost reasons, be the only option available, it could match the performance of an established cytology-based programme. Urine samples, like self-taken vaginal samples, may have a particular place in older participants.
We hypothesise that the quality of cervical sampling deteriorates around the menopause and that menopausal atrophic changes in urogenital mucosa contribute to an increase in unsatisfactory cytology (witness the highly significant trend shown in table 1) and a lower content of HPV DNA in cervical samples. A significant decline in sensitivity of cervical hrHPV detection in women aged ≥40 years compared with women aged ≤29 years for detection of CIN2+ has been reported.24 That was attributed as most likely due to misclassification of CIN2+ in older women. Others25 ,26 have confirmed the finding and suggested25 that false-negative HPV tests (in the setting of CIN2 within ASCUS) might increase further with increasing age. The loss of concordance between hrHPV detection and cytological abnormalities with age clearly points to a need for caution.2 We cannot rule out the possibility that, in follow-up, relatively more CIN2+ may be detected in older women compared with younger women who were hrHPV+ on the self-sample alone. Longitudinal analysis of the PaVDaG cohort is planned which will address this directly. We are also embarking on a self-sampling study in women beyond the normal cut-off age for routine screening and plan to offer colposcopy to all who prove hrHPV (all 14 types) positive.
To conclude, PaVDaG has demonstrated that hrHPV testing with a PCR-based test on self-samples is as sensitive and specific in finding cervical precancer as clinician-collected samples.
Acknowledgments
The authors thank all women participating in the study. They acknowledge the contribution and support of medical staff in all GP practices in Dumfries and Galloway, in particular all practice nurses, who are the main providers of cervical sampling, counselling and health education delivered to all women participating in cervical screening. The authors thank Dr W Forson for clinical support, J Keggans for establishing database and support in data collection and governance, and H Barrington and A McFadyen for help with data analysis. They thank their colleagues in the microbiology laboratory in DGRI and at the Coombe Women and Infants University Hospital, Dublin, Ireland, for performing HPV testing and colleagues in the pathology laboratory in DGRI for logistic and diagnostic support. They also thank S Boyle and G Zhang for analysis of Ct values. MA was supported by the seventh Framework programme of DG Research & Innovation of the European Commission through the COHEAHR Network (grant No. 603019), coordinated by the Free University of Amsterdam.
References
Footnotes
Contributors GS was the chief investigator of the study and was responsible for study design, literature search, data collection, data analysis, data interpretation, coordination of care delivery, dissemination and manuscript preparation. HC provided input into study design, involvement in patient-facing activities and clinical management, dissemination and manuscript preparation. GB provided input into study design, governance, delivery, dissemination and manuscript preparation. JL provided input into study design, governance, dissemination and manuscript preparation. KC provided input into study design, literature searches, data analysis, data interpretation and manuscript preparation. MA was involved in literature search, data analysis, data interpretation and manuscript preparation. AW provided input into study design, data collection, governance and manuscript preparation.
Funding This work was supported through general research funding of the Chief Scientist Office, Scotland. The study collection kits and HPV testing were donated by Roche.
Competing interests GS and GB have received speaker's fees from Roche. GS, GB, HC and JL are current or past employees of National Health Service (NHS) Dumfries and Galloway. That organisation received collection and testing kits for the study from Roche. KC has received project funding and/or consumables to carry out assay evaluations from Roche.
Ethics approval NHS research ethical approval was granted by West of Scotland Research Ethics Service Ref. 12/WS/0085.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data set is available from the corresponding author.