Article Text

Abstract
Objectives Population-based health risk assessment and stratification are considered highly relevant for large-scale implementation of integrated care by facilitating services design and case identification. The principal objective of the study was to analyse five health-risk assessment strategies and health indicators used in the five regions participating in the Advancing Care Coordination and Telehealth Deployment (ACT) programme (http://www.act-programme.eu). The second purpose was to elaborate on strategies toward enhanced health risk predictive modelling in the clinical scenario.
Settings The five ACT regions: Scotland (UK), Basque Country (ES), Catalonia (ES), Lombardy (I) and Groningen (NL).
Participants Responsible teams for regional data management in the five ACT regions.
Primary and secondary outcome measures We characterised and compared risk assessment strategies among ACT regions by analysing operational health risk predictive modelling tools for population-based stratification, as well as available health indicators at regional level. The analysis of the risk assessment tool deployed in Catalonia in 2015 (GMAs, Adjusted Morbidity Groups) was used as a basis to propose how population-based analytics could contribute to clinical risk prediction.
Results There was consensus on the need for a population health approach to generate health risk predictive modelling. However, this strategy was fully in place only in two ACT regions: Basque Country and Catalonia. We found marked differences among regions in health risk predictive modelling tools and health indicators, and identified key factors constraining their comparability. The research proposes means to overcome current limitations and the use of population-based health risk prediction for enhanced clinical risk assessment.
Conclusions The results indicate the need for further efforts to improve both comparability and flexibility of current population-based health risk predictive modelling approaches. Applicability and impact of the proposals for enhanced clinical risk assessment require prospective evaluation.
- case finding
- clinical decision making
- chronic care
- Health risk assessment
- Patient stratification
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The manuscript compares five population-based health risk assessment and stratification strategies placed in five European regions leading deployment of integrated care for chronic patients.
Characteristics of population-based health risk predictive modelling tools limiting comparability across regions and precluding their adaptation to evolving needs are explored.
A conceptual approach making use of the potential of population-based health risk prediction to enhance clinical risk predictive modelling is formulated.
A conceptual frame for dynamic integration of heterogeneous data to pave the way toward personalised medicine is proposed.
Validation and implementation of the study proposals require further work beyond the scope of the current research.
Introduction
Large scale deployment and adoption of integrated care services in Europe seek health efficiencies with simultaneous reduction of outcome variability within and among regions.1–4 It is well recognised that health risk assessment can be relevant for regional adoption of integrated care5–7 because of its impact on the design of healthcare services, as well as for stratification and clinical management of chronic patients.6 ,8 ,9
The current study was carried out within the frame of the Advancing Care Coordination and Telehealth (ACT) programme (http://www.act-programme.eu)9 involving five leading European Union (EU) regions in terms of scaling up integrated care: Basque Country (ES), Scotland (UK), Lombardy (I), Groningen (NL) and Catalonia (ES). Integrated care was defined as the organisation of activities among participants involved in a patient's care to facilitate the appropriate delivery of healthcare services.9
The 2.5-year ACT programme, initiated in 2013, explored the organisational and structural processes needed to successfully implement integrated care services on a large scale. By specifically investigating four key drivers influencing the effective deployment of integrated care services and generating ‘best practice’ examples, ACT intended to provide the foundation to help overcome current barriers for extensive adoption of integrated care. The four key drivers addressed in the ACT programme were: risk assessment and stratification, workflows and organisational structures, staff engagement and patient adherence.
In the healthcare services domain, population-based risk predictive modelling facilitates the elaboration of stratification maps characterising risk strata distribution of the entire population in a given geographic location. It allows identification of subsets of citizens with similar healthcare requirements facilitating both case finding and screening. The former, case finding, identifies highly vulnerable patients, allocated at the tip of the risk pyramid, who are prone to major deleterious health events such as unplanned hospital admissions/readmissions, fast functional decline and/or death.10 ,11 Likewise, performing screening for discovery of cases with non-manifest illnesses may benefit from early diagnosis and cost-effective preventive interventions.6
In the clinical management domain, risk prediction of well-defined medical problems (ie, prediction of survival in acute exacerbations of chronic obstructive pulmonary disease (COPD))12 can support health professionals in the decision-making process. Moreover, clinical risk prediction may contribute to patient classification in the optimal healthcare tier, helping to define shared care arrangements between primary care and specialists. However, it is acknowledged that modelling tools addressing specific clinical issues with a high predictive power may present limitations for their general application outside the source population.7 ,13
The study, therefore, addresses two specific aims. First, to analyse population-based health risk assessment strategies, including assessment tools and health indicators, in the five ACT regions, in order to identify current barriers and to elaborate recommendations for large scale deployment of integrated care at the European level. The second aim was to elaborate on strategies toward enhanced health risk predictive modelling in the clinical scenario.
Methods
Whereas the general characteristics of the population and healthcare organisation of these five regions have been reported in detail elsewhere,9 the analysis of population-based health risk assessment and stratification strategies in place in the five ACT regions was carried out focusing on two specific components: (1) analysis of health risk predictive modelling tools and (2) comparison of reported health indicators. The latter was addressed to assess comparability of health status among regions. Finally, a use case to analyse the potential for innovation in population-based health risk prediction was identified and explored.
Population-based health risk predictive modelling
We performed a two-phase survey approximately 8 months apart (Summer 2014 and Spring 2015), addressing the person responsible for the development/maintenance of the risk assessment strategy in each of the five ACT regions. The five persons (see acknowledgements) were fully accessible through the duration of the project, but the interviews were naturally grouped in two periods, as described above. Details on the characteristics of the survey are reported in the on-line online supplementary material (part I, pages 1 to 24).
Supplemental material
In the first survey, systematic responses to a standardised questionnaire elaborated for this purpose by Opimec14 were collected. Participants answered the questionnaire by mail and subsequently underwent an interview. We captured information on several key dimensions characterising the risk predictive modelling tools, namely: (1) modelling approach, (2) source sample, (3) main and summary statistics, (4) outcome (dependent) variables and covariates, (5) update periodicity, (6) target population and (7) maturity of clinical implementation. This facilitated the elaboration of an initial map of regional practices.
The second survey had a twofold purpose: (1) to fill specific information gaps identified after the first survey and (2) to ask additional questions inquiring on existing plans for evolving the risk predictive modelling tool in place. Also, we assessed the potential for transferability across regions at EU level. The core objective of the second survey was to elaborate on future strategies to overcome limitations of current population-based risk assessment tools that were identified during the first survey. To this end, four main items were analysed: (1) openness of algorithms, (2) flexibility for adjustments to other populations, (3) license costs associated with the use of the case finding tool and (4) licence agreements binding its applicability to specific territories.
The comparative analyses of health risk assessment tools among ACT regions were carried out taking into account a clear distinction regarding the characteristics of the source population. That is, health risk assessment tools generated from modelling the entire population of a given region (or geographical area) with a holistic approach were considered to follow a population health approach, as proposed by Kindig and Stoddart in 2003.15 On the other hand, health risk assessments derived from modelling patient populations were regarded as following a population medicine approach.16
Owing to our interest in case finding and screening analyses, the current study focused on healthcare forecasting17 that implies predicting an individual's healthcare utilisation for interventional purposes with either preventive or therapeutic goals. Comprehensive descriptions of the characteristics of health risk predictive modelling and the logistics required for deployment are reported elsewhere.18–20 It is of note that other analyses such as risk adjustment21–23 or actuarial approaches24 were not considered in the current research.
Health indicators
One of the initial goals of the ACT programme was to identify a common set of indicators useful to evaluate the impact of health interventions at population level in order to facilitate comparability of the effects of integrated care services over time within and across regions. As a first step of this objective, a semistructured questionnaire including indicators to evaluate health status at population level was sent via email to the ACT coordinator in each of the five regions. The specific objective of the questionnaire was to assess comparability of health status across regions at baseline. The characteristics and dimensions covered by the questionnaire are reported in detail in the online supplementary material (part II, table 1S). The indicators selected in the current study were shared by the five ACT regions and had been previously defined and agreed within the consortium.
Overcoming current limitations of health risk assessment tools
In 2015, a novel population-based health risk assessment tool (GMAs, Adjusted Morbidity Groups) was deployed in Catalonia (see online supplementary material tables 2S-3S and figures 1S and 2S). The deployment included display of the GMA stratification results in the clinical workstation used by primary care physicians.
The GMAs were developed independently from the ACT programme. It is of note, however, that the evaluation of this risk assessment tool, carried out before its regional deployment, provide the basis to generate a proposal for enhanced health risk predictive modelling in the clinical setting.
The performance of the GMAs was compared with the results of the Clinical Risk Groups (CRGs) risk predictive model,25 used in Catalonia until 2014, through two complementary approaches: (1) statistical evaluation assessing prediction of relevant healthcare outcomes, namely: mortality, unplanned admissions, emergency department consultations and healthcare expenditure (figure 1), and (2) clinical evaluation carried out by general practitioners. The latter consisted of a comparative clinical evaluation of GMA and CRG classifications blindly undertaken by 40 general practitioners examining electronic health records from 1000 cases (25 cases per general practitioner; see online supplementary figure 3S).

Explained variability indicated by R2 (expressed as a percentage) in the y-axis, for four main outcomes: mortality, hospital admissions, emergency department visits and total healthcare expenses obtained from the analysis of the Catalan population (7.5 million inhabitants) in 2014, using three different health risk assessment models built-up with different covariates: A+S+SE includes only age, sex and socioeconomic status as covariates; A+S+SE+CRG additionally includes Clinical Risk Groups as morbidity grouper25 and A+S+SE+GMA includes information from Adjusted Morbidity Groups as morbidity grouper (see online supplementary material for further details, part I).
Results
Population-based health risk assessment tools
The main characteristics of the health risk predictive modelling tools in place in four out the five ACT regions are depicted in table 1. Groningen (NL) is not represented because the site does not use any population-based health risk predictive modelling for the two integrated care programmes currently deployed.9 Instead, Groningen prioritised individual health risk characterisation based on information collected in the electronic health records.
Risk predictive modelling tools in the ACT regions*
Table 1 indicates that a population health approach15 is currently only adopted in the Basque Country26–29 and in Catalonia. Since 2010, Scotland30 is clearly evolving in this direction. The source population of the current health risk predictive modelling tool already covers 63% of the entire Scottish population. Strategically, it is moving from a strong focus on use of hospital-related resources (eg, emergency department consultations, unplanned hospital admissions and/or early readmissions) toward integration of needs for frail patients, including social support and long-term care. Periodic updates are carried out in the three regions.
In contrast, Lombardy31 has a population medicine approach consisting of a classification system based on stratification by health costs. It serves the coordinated care programme for chronic patients, especially those with conditions such as COPD, cardiovascular disorders and diabetes mellitus types I and II.
The analysis of the risk-strata distributions resulting from the different regions showed poor comparability (table 2). This is explained by differences among risk predictive modelling tools, and by the diverse classification criteria used to define risk groups.32
Risk prediction strategies and characteristics of data reporting for the study on top indicators in the five ACT regions
We identified significant constraints for transferability across regions due to three main factors, namely: (1) lack of openness of algorithms, (2) inclusion of expert-based criteria in the morbidity groupers and (3) license bindings constraining applicability of health risk assessment tools to other EU regions. It is of note that only Catalonia and Scotland (table 2) have white-box tools owned by the regions, which, in principle, implies high potential to properly deal with the limitations for such transferability.
We identified a consensus on the need for transferring information on high-risk patients to practising clinicians in order to trigger preventive interventions and to support clinical decision-making processes. However, we observed different degrees of maturity in the interactions with clinicians, from only providing a list of high-risk candidates for interventions to the display of simple clinical decision support systems in the clinical workstation of primary care physicians.
Despite the actual differences among the five ACT regions, the two surveys showed consensus in the basic aspects, indicated (in table 3) that they should be covered by an ideal health-risk assessment strategy showing transferability among regions and potential to generate synergies with clinical risk predictive models. The practicalities for deployment of health risk assessment tools at regional level are summarised in online supplementary table 4S.
Recommendations for good practice population-based health risk assessment
Health indicators
The list of recommended indicators identified by the consortium is included in the online supplementary material. We found that, despite availability of most of the data at the regional level, two main limiting factors precluded baseline comparisons among the regions, namely: (1) insufficient data harmonisation (eg, different versions of International Classification of Diseases (ICD) coding)33 and (2) differences in data reporting (ie, different levels of data aggregation and/or differences in calculation of complex indices). The outcome of the baseline assessment did not allow completion of the initial ACT plan on health indicators described in the Methods section.
The GMA as a use case
Among the different population-based health risk assessment tools evaluated in ACT (table 1), only GMA as the novel predictive modelling tool deployed in Catalonia34 ,35 complied with the main characteristics recommended in table 3. The current GMA version covers four key requirements: (1) a population health approach using the entire source population of 7.5 million inhabitants of the region, with a bi-annual update of the risk pyramid distribution, (2) publicly owned without licensing constraints, (3) open source computational algorithms and (4) that the GMA morbidity grouper relies only on statistical criteria thus facilitating quick adaptation to different territories. Accordingly, it was selected as a use case for the analysis carried out in the current section.
Figure 1 illustrates the percentage of explained variability by GMA for four relevant outcomes, namely: mortality, hospital admissions, emergency department admissions and total healthcare expenses. It is of note that GMAs accounted for a higher percentage of variability than did CRGs.25 Additionally, the results of the analysis of concordance among clinical evaluators indicated that the two morbidity groupers (GMA and CRG) agreed with clinicians in the classification of the cases by complexity, but GMAs showed a better performance in the strata of greater complexity (see online supplementary figure 3S). Moreover, in most cases, clinical evaluators preferred GMAs.
Overall, the GMA shows flexibility and transferability, as demonstrated by its recent adoption by 13 of the 17 regional healthcare systems in Spain, covering 92% of the overall Spanish population, approximately 38 million citizens. Consequently, the GMA can be considered a health risk assessment model that overcomes the main limitations identified in the current study. Accordingly, it seems suited to aid future assessment of the potential of population-based risk assessment and enhance clinical risk modelling. To this end, the steps that should be fulfilled in order to shape the proposal are described below.
Statistical refinement of the computational modelling of the current GMA,36 in order to generate an enhanced GMA personalising current information on socioeconomic status, is recommended as the first milestone to enhance clinical risk predictive modelling. In a second step, we propose to incorporate the classification of the individual in the risk stratification pyramid as one of the covariates of clinical risk predictive modelling. It is of note, however, that prospective assessment of both practicalities and quantification of the added value of the proposed approach are needed but were beyond the scope of the current research.
Discussion
Summary of main findings
The results of the two surveys indicated a high degree of conceptual agreement among the five ACT regions on the relevant role of population-based health risk assessment for regional deployment of integrated care. The entire ACT consortium shared its usefulness for service commission, case finding and screening. There was also consensus on the use of a population health approach15 as the optimal strategy for population-based risk assessment.
However, the health risk predictive modelling tools in place displayed marked heterogeneities that precluded comparability of the risk pyramid distributions across regions. Likewise, different well-identified problems mostly associated with data reporting precluded appropriate comparisons of the recommended health indicators described in the online supplementary material table 1S.
The current study identified transferability across regions and the potential for evolving, namely, flexibility, as two key requirements for any population-based health risk assessment tool. Factors such as: (1) license binding constraints, (2) insufficient public availability, (3) lack of availability for inspection and/or (4) rigidity of some computational algorithms (ie, due to inclusion of expert-based criteria in some morbidity groupers)—are currently limiting transferability. These factors might also preclude adaptation of the current risk prediction tools toward evolving requirements such as: (1) integration between healthcare and social services and (2) implementation of synergies between population-based and clinically oriented risk predictive modelling, as described in the study. The analysis of the GMA as a use case (figure 1 and see online supplementary figure 3S) seems to support the recommendations on innovation on population-based health risk prediction, as displayed in table 3.
We acknowledge some intrinsic limitations of population-based predictive modelling in terms of robustness of derived estimations. However, allocation of individuals into the risk stratification pyramid based on this approach seems to facilitate the design and implementation of sustainable and successful preventive strategies. Along these lines, we forecast that recommendations generated by the current study (table 3) will contribute to strengthen evidence on the cost-effectiveness of population-based risk predictive tools.
Moreover, the study reports on the conceptual steps required for development of innovative strategies for clinical risk predictive modelling with potential to enhance its supporting role for decision-making in the clinical scenario. We acknowledge, however, that further studies evaluating feasibility, benefits and applicability of the proposals for enhanced clinical risk prediction are needed.
Population-based health risk prediction
While the ACT project has confirmed consensus on the role initially ascribed to population-based health risk assessment in regional deployment and adoption of integrated care services, the core lesson learnt from the current study is the need for innovative approaches to risk predictive modelling. Our analysis suggests two basic pillars for a future European extension: (1) implementation of the recommendations for risk predictive modelling tools displayed in table 3 and (2) ability to report on the list of basic indicators depicted in the online supplementary material. The current heterogeneities among regions clearly indicate that adjustment of the current settings to the recommended good practice will require site-specific transitional strategies the common goals and basic principles of which are described in the current study. Key operational steps needed for practical implementation of a regional strategy for population-based health risk predictive modelling are summarised in online supplementary table 4S.
There is a lively debate regarding management modalities associated with generation and exploitation of population-based health risk predictive modelling. Should model generation and maintenance be publicly funded (ie, Department of Health) or should there simply be policies promoting open market in terms of private suppliers of risk predictive tools?18 ,37 The current study only emphasises the need for openness, flexibility and transferability of risk predictive modelling in order to fulfil their core purposes. However, as stated below, we acknowledge the complexities of the issue, also involving ethical aspects. Doubtless, this issue will require proper regulation irrespective of the finally adopted business model.
Enhanced clinical health-risk assessment
The authors acknowledge that only a small proportion of the huge potential of risk predictive modelling is currently applied for health forecasting purposes in the clinical arena. A detailed description of the bottlenecks constraining the developments recommended for enhanced clinical risk predictive modelling, as proposed in the current study, are reported elsewhere.38 Under the subheading, we are highlighting only a few key aspects that need attention to successfully accomplish the roadmap proposed in the current study. No doubt the milestones described above to explore the current proposal for enhanced clinical risk prediction, in terms of validation and implementation, constitute the first priority.
Toward personalised medicine
We believe that the current study contributes to paving the way for a future holistic approach to risk prediction.39 Such a strategy will consider multiple covariates influencing patient health and should allow personalised design medicine care pathways for chronically ill patients.
Three categories of covariates have been identified to show potential for inclusion into clinical risk predictive modelling, as displayed in figure 2: (1) input from enhanced case finding tools, that is, population-based health risk predictive models, as mentioned above, (2) individual clinical, physiological and biological information relevant to the medical problem being assessed, and (3) subject-specific informal care data including lifestyle, adherence profile, socioeconomic status, requirements in terms of social support and environmental factors. It is hypothesised that inclusion of all these covariates influencing patient health will markedly increase the predictive accuracy and facilitate clinical decision-making based on sound estimates of the prognosis of an individual.

The dimensions of patient health indicated in the figure may contribute to enrich clinical risk predictive modelling. As a first step, we propose to include the outcome of the population-based risk assessment as a covariate in clinical risk predictive modelling. For future personalised care for chronic patients, enhanced dynamic communication among Informal Care, Health Care and Biomedical Research will allow inclusion of several dimensions into clinical risk predictive modelling. It will be carried out through multilevel/multiscale heterogeneous data integration within a Digital Health Framework, as depicted in figure 3.
The three categories of covariates, as alluded to above, shall be dynamically captured from different sources, respectively: (1) population-based health risk predictive models; (2) articulated healthcare and biomedical research knowledge (integration of clinical, physiological and biological/molecular information), and (3) in-place personal health folders (lifestyle, adherence profile, socioeconomic status, social support and environmental factors).
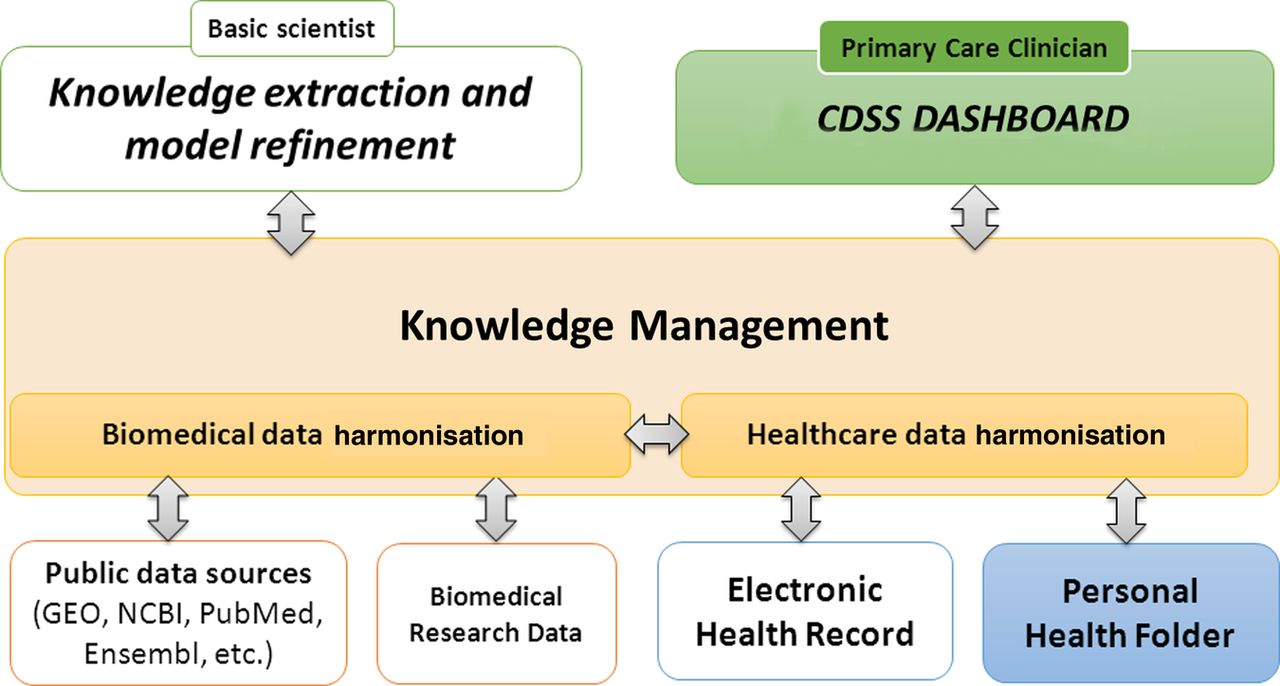
The implementation of specific solutions within a Digital Health Framework, conceptually formulated elasewhere,40 should have the potential to articulate the three categories of variables, potentially allowing for dynamic assessment of health risk both for population-based purposes, as well as for specific clinical problems. Nowadays, a Digital Health Framework, as depicted in figure 3, is only a conceptual formulation, but it contains the seeds to foster the concept of the ‘exposome’, as defined by Coughlin,39 which provides the basis for personalised medicine in chronic cases. There is no doubt that the implementation of specific solutions within the envisaged Digital Health Framework constitutes an ambitious endeavour requiring a stepwise approach to effectively overcome major challenges involved in the transitional process to make it operational.
{kind=link}
{kind=link}
{kind=link}
Scheme of the Digital Health Framework,40 composed of digital data normalisation and knowledge management layers for knowledge generation, and novel Clinical Decision Support Systems (CDSS) embedded into integrated care processes.
Enhanced applicability and integration of powerful data analytics, including risk predictive modelling, into clinical practice also constitutes a central goal of the above Digital Health Framework. In this regard, the development of novel clinical decision support systems, bolstered by advanced visual analytics, facilitating representation of patient information for effective clinical management of time-varying individualised data, is a real yet unmet need to facilitate clinical judgement for decision-making. Moreover, studies assessing the potential of different modalities of patient gateways, such as the personal health folder, for patient self-management purposes and for collection of informal care variables, are urgently needed.
Finally, the novel healthcare scenario reveals new emerging needs regarding highly relevant non-solved ethical issues. These are related to privacy, security of data transfer, as well as risks associated with healthcare decisions that rely on inadequate risk predictive models. The complexities involved in some of these aspects can only be addressed through a democratic debate; openness and transparency of the healthcare governance; as well as a timely and appropriate evolution of legal frames.
Conclusions
The implementation of current recommendations for population-health risk assessment, in terms of risk predictive modelling and health indicators, constitutes a priority for the on-going processes of adoption of integrated care at the European level. The current study proposes novel strategies for enhanced clinical risk assessment and stratification, together with a roadmap for evaluation and future implementation of the novel approach.
Acknowledgments
The authors acknowledge the contributions from the ACT consortium; the B3 group from EIP-AHA; and the ASSEHS (Activation of Stratification Strategies and Results of the interventions on frail patients of Healthcare Services) consortium. The authors would like to thank, for the input provided, the technical persons from the regions contributing to the two-phase survey carried out during the project lifetime: Jon Orueta Mendia from Osakidetza (Basque Country, ES), Anne Hendry from the Scottish Government–NHS24 (Scotland, UK); Wietse Veenstra from Scheper Hospital Emmen in collaboration with UMCG (Groningen, NL); and Carlo Scire from Lombardia region in collaboration with Telbios. The authors are grateful to Andrés Cabrera, from Escuela Andaluza de Salud Pública, who created the Opimec questionnaire used in the current research. The authors are also indebted to Montse Bustins and Alex Guarga, from Servei Català de la Salut (Catalan Health Service), Francesc Garcia Cuyàs from TicSalut foundation, Pol Pérez from Institut Català de la Salut, Albert Ledesma from the Departament de Salut de la Generalitat de Catalunya (Catalan Health Department of the Government of Catalonia) and Marian López, Alfredo Martin, Carmen Arias and Paloma Casado, from the Ministerio de Sanidad Servicios Sociales e Igualdad (Ministry of Health, Social Services and Equity), for their support to the current study and for the support from their institutions in developing the GMA.
References
Footnotes
ID-E, EV two authors equally contributed to the research.
Twitter Follow Jordi Piera at @jpieraj
Contributors JR takes responsibility for and is the guarantor of the content of the manuscript, including the data and analysis. IDE, EV and JR led the study, performed the interviews and the comparative analysis and drafted the manuscript. All the authors contributed to the conception, hypotheses delineation, design of the study, acquisition of the data or analysis and interpretation of results, critically revised the article, approved the final version to be published and agreed to be accountable for all aspects of the work. The ACT consortium approved the final version of the manuscript.
Funding Supported by ACT—Advancing Care Coordination and Telehealth Deployment programme (UE Grant number 20121209), PITES (FIS-PI12/01241) and Generalitat de Catalunya (2014SGR661).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.