Article Text

Abstract
Introduction The aim of this systematic review is to assess the efficacy and safety of Chinese herbal medicine for the treatment of patients with vascular cognitive impairment but no dementia.
Methods and analysis We will perform a comprehensive retrieval in the following electronic databases: PubMed, Cochrane Library, EMBASE, CINAHL, Chinese Biomedical Literature Service System (SinoMed), China National Knowledge Infrastructure (CNKI), Chinese Scientific Journals Database (VIP), Wan-fang database and other sources. After screening the studies, the methodological quality of all included trials will be assessed according to the risk of bias instrument provided by the Cochrane Collaboration. A meta-analysis of randomised controlled trials will be conducted using RevMan V.5.3 software. Funnel plot analysis and Egger's test will be used to assess publication bias, if possible. The quality of evidence will be assessed by the GRADE system.
Dissemination This systematic review will be disseminated in a peer-reviewed journal and a relevant conference presentation.
Trial registration number PROSPERO CRD 42015023682.
- Chinese herbal medicine
- Vascular cognitive impairment no dementia
- Protocol
- Systematic review
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study is a comprehensive, objective and normative systematic review on the efficacy and safety of Chinese herbal medicine for vascular cognitive impairment in participants without dementia.
Study screening, data extraction and assessment of the risk of bias will be conducted independently by two researchers.
Currently, there is a lack of internationally recognised diagnostic criteria in vascular cognitive impairment without dementia. Therefore, subgroup analyses will be carried out to explore any sources of heterogeneity.
Introduction
As the population ages and survival from vascular disease are improved, cognitive dysfunction and dementia caused by cerebrovascular disease (CVD) have become prevalent.1 Recently, vascular cognitive impairment (VCI) has been introduced to describe the entire spectrum of cognitive dysfunction—ranging from cognitive impairment without dementia to dementia—attributable to all forms of CVD.1 ,2 There are three subtypes of VCI: VCI no dementia (VCIND), vascular dementia (VaD) and mixed VaD and Alzheimer's disease (AD).3 Among them, VCIND is characterised by early or mild cognitive impairment due to cerebrovascular injuries with an insidious nature.4 It may be considered to be the prodromal stage of VaD,5 with occurrence in 26.9% of patients approximately 3 months after stroke onset.6 A cohort study which included 149 participants with VCIND showed that 46% cases were observed to develop dementia, and 52% of these cases died within 5 years.7 Another community-based, cross-sectional study in China also reported that the overall prevalence of post-stroke cognitive impairment (PSCI) was 80.97% (95% CI 77.82% to 84.11%), while that of non-dementia PSCI (PSCI-ND) and post-stroke VaD was 48.91% (95% CI 44.91% to 52.92%) and 32.05% (95% CI 8.32% to 35.79%), respectively.8
Fortunately, VCIND is potentially treatable and preventable.3 Early diagnosis and appropriate interventions may contribute to the improvement of the prognosis.9 However, there are limited treatment options to improve cognition and function in VCI.1 Chinese herbal medicine (CHM), which has been used for thousands of years in China, has been considered promising for improving cognitive function.10 A meta-analysis of CHM for VaD showed that there were significant benefits associated with CHM groups in terms of effective rate, Mini-Mental State Examination (MMSE) scores and Hasegawa Dementia Scale scores at the end of treatment. Furthermore, fewer adverse events occurred in the treatment group. In the light of this evidence, CHM appears to be safe and effective for VaD.11 A meta-analysis which focused on the efficacy and safety of CHM for VCIND indicated that CHM could improve patients’ cognitive and behavioural functions compared to the treatment with Western medicine.12 However, the information source was limited to Chinese medical databases and there was no flow chart to show the study screening process. Therefore, we aim to carry out a more comprehensive and normative systematic review to provide objective and scientific evidence on CHM for the treatment of VCIND.
Methods and analysis
Inclusion and exclusion criteria for study selection
Types of studies
Randomised controlled trials (RCTs) which used CHM or a combination of CHM and routine pharmacotherapy as treatment measures will be eligible. Language will be limited to English and Chinese.
Types of participants
No internationally recognised diagnostic criteria currently exist and no laboratory tests are available for VCIND diagnosis.13 ,14 Therefore, this study will include patients who were diagnosed with VCIND based on diagnostic criteria used in international clinical trials15–17 or Chinese expert consensus.18–20
The study will include all types of patients regardless of their age, sex, ethnicity, education or economic status and whether or not they were outpatients or inpatients.
Patients should have acquired cognitive impairment, but not meet the diagnostic criteria for any type of dementia. Furthermore, their cognitive impairment was judged to have vascular risk factors or CVD (including clinical features or radiographic features).
Types of interventions
Studies reporting any type of CHM treatment will be included. CHM could be used alone or combined with routine pharmacotherapy. Studies where the control group is different from the pharmacotherapy in the intervention group will be excluded. Trials in which the intervention group includes any other Chinese medicine therapies (eg, acupuncture, moxibustion, massage, taichi, etc) will be excluded.
Types of comparators
Comparators will include placebo control, no treatment, routine pharmacotherapy, routine care and other conventional treatments.
Primary outcome assessments
Primary outcome measures for assessment should include at least one of the internationally recognised evaluation scales, which refer to one of the following aspects: cognitive function, activities of daily living, behavioural and psychological symptoms of dementia (BPSD) or global evaluation scales (table 1).
Summary of primary outcome assessments
Secondary outcome assessments
The secondary outcome assessments will be the incidence and severity of adverse events.
Search methods for identification of studies
Electronic searches
We will perform a comprehensive retrieval for studies that evaluate the efficacy and safety of CHM in patients with VCIND in major Chinese and English medical databases including PubMed, Cochrane Library, EMBASE, CINAHL, Chinese Biomedical Literature Service System (SinoMed), China National Knowledge Infrastructure (CNKI), Chinese Scientific Journals Database (VIP) and Wan-fang database from their respective inceptions to July 2015. The following subject terms and key words will be used in the search: (‘vascular cognitive impairment’ OR ‘mild cognitive impairment’ OR ‘post-stroke cognitive impairment’ OR ‘VCI’) and (‘Medicine, Chinese Traditional’ OR ‘Drugs, Chinese Herbal’ OR ‘herbal medicine’ OR ‘Chinese traditional medicine’ OR ‘Traditional Chinese medicine’). Chinese translations of these search terms will be utilised to search the Chinese databases. The search strategy for PubMed is given in table 2 and detailed steps are shown in online supplementary appendix 1.
Supplemental material
Search strategy used in the PubMed database
Other sources
Studies from other sources will also be obtained from the following sources:
Google scholar (http://scholar.google.com) and Baidu scholar (http://xueshu.baidu.com/);
Clinical Trials.gov (http://www.clinical trails.gov) and Chinese Clinical Trial Registry (http://www.chictr.org/cn/);
The reference lists of the retrieved articles.
Data extraction and quality evaluation
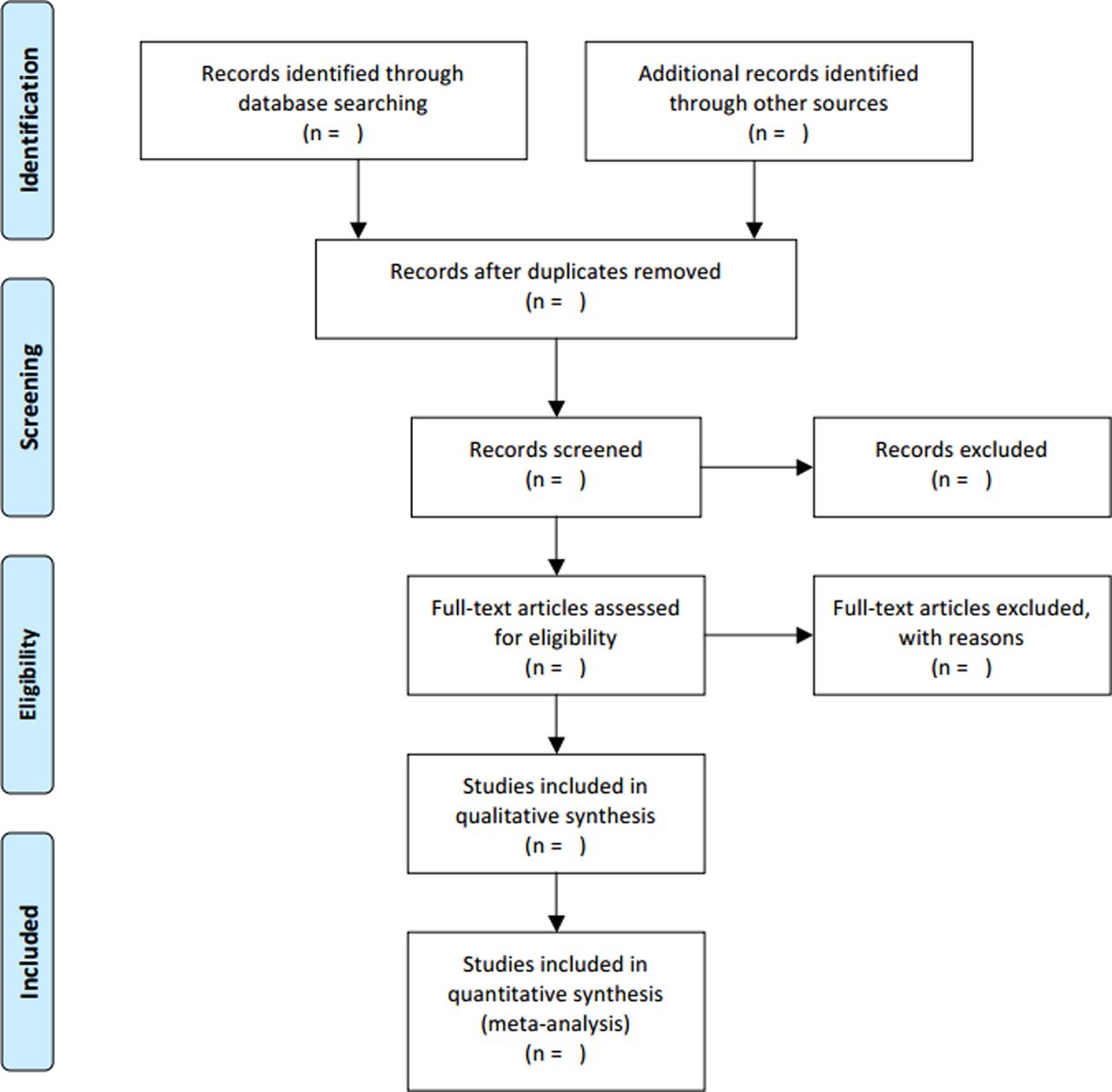
EndNote X6 software will be used to manage the literature and the process of removing duplications. A data extraction EXCEL table will be designed which includes the data on age, sex, duration, education level, lifestyle (eg, smoking, alcohol consumption), vascular risk factors (eg, hypertension, hyperlipidaemia, diabetes), medical comorbidities, concurrent medications (eg, antiplatelet aggregation drugs, antihypertensive drugs, hypoglycaemic drugs), randomisation, blinding, interventions, comparators, outcomes, study dropouts, the incidence and details of adverse effects. Two researchers (MF and JL) will extract and double-check the data from the included articles. Any discrepant data will be reviewed by discussion with another team member (SL). The details of the study selection will be shown in a PRISMA flow chart (figure 1).

{kind=link}
Flow diagram of selection process.
Risk of bias assessment of included studies
The methodological quality of all included trials will be assessed by a ‘risk of bias assessment tool’ according to the Cochrane Handbook 5.1 by two independent researchers (MF and JL). Any different views will be discussed with another team member (SL). The risk of bias in the included studies will be evaluated according to the eight domains: randomisation sequence generation, randomisation allocation concealment, blinding of participants, blinding of personnel, blinding of outcome assessors, incomplete outcome data, selective outcome reporting and other sources of bias. Since many reports of RCTs published in Chinese journals lacked an adequate description of randomisation sequence generation and allocation concealment,21 we will retrieve related protocols in clinical trials registration websites and contact first author/s or corresponding author/s through email or telephone for further details of these two domains.
Strategy for data synthesis and statistical analysis
We will use RevMan V.5.3 software for data analysis. For continuous data collected using the same measurement scale, we will calculate weighted mean difference and 95% CIs. For continuous data collected using similar measurement scales for the same outcome, we will calculate standardised mean differences with 95% CIs. For dichotomous outcomes, we will use risk ratio with 95% CI and p values to assess the efficacy and safety of CHM. A standard χ2 statistic and I2 statistic will be used to test heterogeneity between groups. Data will be analysed with a fixed-effect model if no statistical heterogeneity was observed between subgroups (p≥0.1, I2≤50%). In the presence of heterogeneity (p<0.1, I2>50%), a random-effect model will be used and the possible causes of heterogeneity will be examined.
Dealing with missing data or unclear scale type
We will attempt to contact the authors of included studies in which there are missing data or unclear sources of the evaluation scales through email or telephone. For missing data, if we fail to obtain sufficient data after contacting authors, an intention-to-treat analysis will be performed if feasible.
Planned subgroup analyses
Where possible, we will perform subgroup analyses based on different demographic characteristics or vascular risk factors, severity of included patients, different disease durations, diagnostic criteria, intervention type (CHM or CHM in combination with routine pharmacotherapy), routes of administration, dosage, preparations and ingredients of CHM interventions and controls.
Sensitivity analysis
Where feasible, we will carry out sensitivity analyses to investigate the robustness of the study conclusions, such as grouping studies by different levels of the methodological quality.
Assessment of publication biases
We will use funnel plots in RevMan V.5.3 and Egger's test in Stata 11.0 to detect publication bias if more than 10 studies are included in the meta-analysis.
Assessment of quality of evidence
The Cochrane Collaboration Network GRADE (The Grading of Recommendations Assessment Development and Evaluation) will be used to assess the results in this systematic review. We will create a Summary of Finding table in http://www.guidelinedevelopment.org/.
Ethics and dissemination
Ethical approval will not be required for this systematic review because there are no concerns regarding the patient's privacy. The results will be disseminated in a peer-reviewed journal and presented at a relevant conference.
Discussion
VCIND belongs to the categories of Jianwang, Shanwang, Daibing in traditional Chinese medicine.22 CHMs have been cited for treating memory disorders in the classical herbal literature for many centuries,23 and the results of preclinical and clinical studies suggest that CHM could improve cognitive decline.24 ,25 For example, Ginkgo biloba extract EGb 761 is the most extensively clinically tested Chinese herbal-based substance for cognitive impairment and dementia and meta-analytic evidence suggests that EGb 761 provides benefit for stabilising or slowing decline in cognition of people with cognitive impairment and dementia.26 Huperzine A is another Chinese herbal derivative which has been authorised for treating AD and benign memory deficits since 1994 in China.27 As an alkaloid isolated from the Chinese herb Huperzia serrata, Huperzine A can selectively inhibit acetylcholinesterase activity and thus facilitate the increase in acetylcholine level in the brain, thereby improving cognitive function in patients with dementia.28 Meta-analysis also shows that Huperzine A could significantly improve the MMSE and ADL scores of patients with AD and VD with a good tolerance.28 However, there is, as yet, no overall assessment of the clinical evidence regarding CHM interventions for VCIND in evidence-based medicine.
Thus, we plan to conduct this meta-analysis to evaluate the efficacy and safety of CHM therapies for patients with VCIND. We hope that this review will provide evidence to assist clinicians and patients’ decision-making process when dealing with VCIND. However, no internationally recognised VCIND diagnostic criteria exist currently. This will be a potential source of heterogeneity for the included study population and influence the extrapolation of conclusion. Therefore, subgroup analyses according to the characteristics of VCIND and different diagnosis criteria will need to be carried out.
PRISMA-P (Preferred Reporting Items for Systematic review and Meta-Analysis Protocols) 2015 checklist29 of this protocol is presented in online supplementary Appendix 2.
Supplemental material
References
Footnotes
Contributors CL, CCX, XG and ALZ conceived and designed the study. The manuscript of this protocol was drafted by MF, JL and BHM and revised by CL and CCX. MF and JL designed the search strategies and will perform the search, screening and assessment of the risk of bias independently. MF and BHM will analyse and interpret the data. SL will arbitrate any disagreements during the review. All authors approved the final version of this protocol.
Funding This study is funded by a Project Grant from the Guangdong Provincial Science & Technology Department and the Guangdong Provincial Academy of Chinese Medical Sciences (GPACMS) (Project Grant no. 2012A032500009). The study is partially supported by a Grant from the International Science & Technology Cooperation Project of the Ministry of Science and Technology of China (Project Grant no. 2012DFA31760) and International Science and Technology Cooperation Project of TCM funded by the State Administration of TCM, China (Project Grant no.1601500000027 (11)).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.