Article Text

Abstract
Objectives The study examines the meaning of good-quality social care for people with Parkinson's disease and their carers. It identifies, from their perspective, the impact of good-quality social care on health and well-being.
Design Qualitative case study methodology, interview and framework analysis techniques were used. Setting: community locations in the north and midlands of England.
Participants Data were collected from 43 participants including individual interviews with people with Parkinson's disease (n=4), formal and informal social care providers (n=13), 2 focus groups, 1 with people with Parkinson's disease and their carers (n=17), and 1 with professionals (n=8), plus a telephone interview with a former commissioner.
Findings Good-quality social care, delivered in a timely fashion, was reported to have a positive impact on health. Furthermore, there is an indication that good-quality social care can prevent untoward events, such as infections, symptom deterioration and deterioration in mental health. The concept of the ‘Impact Gap’ developed from the findings, illustrates how the costs of care may be reduced by delivering good-quality social care. Control, choice and maintaining independence emerged as indicators of good-quality social care, irrespective of clinical condition. Participants identified characteristics indicative of good-quality social care specific to Parkinson's disease, including understanding Parkinson's disease, appropriate administration of medication, timing of care and reassessment. ‘Parkinson's aware’ social care was seen to generate psychological, physical and social benefits that were inter-related.
Conclusions The findings indicate how maximising quality in social care delivery for people with Parkinson's disease can impact on health and well-being. Long-term or short-term benefits may result in prevented events and reductions in health and social care resource. Health professionals can be instrumental in early detection of and signposting to social care.
- QUALITATIVE RESEARCH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study explains how good-quality social care, delivered in a timely fashion may have a positive impact on health, and prevent untoward events.
Criteria are highlighted that are indicative of good-quality social care specific to people with Parkinson’s disease.
Findings illustrate how the costs of health and social care may be reduced by delivering good-quality social care in an integrated manner. Further health economic studies are required to test these claims.
The research indicates how health professionals can be instrumental in early detection of and signposting to social care.
The study focused on the experiences of those in receipt of social care in England, however, the messages are likely to be of interest to other audiences currently reviewing or testing different models of health and social care integration.
Introduction
Parkinson’s disease is a progressive, neurological disorder, with no known cure. There are approximately 127 000 people with Parkinson's disease in the UK. It is the second most common neurodegenerative condition in the UK and is set to become increasingly common as life expectancy increases. Numbers are estimated to increase by 28% by 2020.1 ,2
Parkinson's disease is a condition that affects movement and activity. It becomes less predictable over time, and people report that symptoms can fluctuate rapidly within the day, or week-by-week, the longer they have had the condition. Slowness of movement, rigidity and tremor are often present and will impact on a person's ability to be active and with self-care. There are also over 30 ‘non motor’ symptoms associated with Parkinson's disease including anxiety, depression, fatigue, pain, continence issues, memory problems and sleep disturbance.2 As the condition progresses, it becomes more complex and has a greater impact on daily living activities. This complexity and symptom burden can result in increased healthcare needs, but also an increased dependency on social care.
Defining social care in contemporary society amidst changing welfare states is challenging.3 Reasons for this include a drive to allocate responsibility for the provision of care within the definition, for example, defining social care as that funded by local authorities or voluntary sector.3 ,4 In addition, it can be problematic establishing a difference between health and social care, as activity can lie in the margins or overlap across both.4 For the purpose of this study, social care includes the range of interventions that help people conduct activities of daily living and maintain independence and well-being. This includes ‘traditional’ services, such as personal care at home, support for the person’s carer, aids and adaptations at home, and day-care provision. It also includes ‘non-traditional’ services, for example, care to support engagement in hobbies and interests outside the home. Social care can be provided by a number of different agencies and professions including formal care provider organisations as well as family and friends.4 We did not include interventions from health professionals which were seen to fall within a definition of healthcare. However, we recognised that health professionals may be key to people with conditions such as Parkinson's disease accessing social care. For example, doctors, specialist nurses or occupational therapists making referrals for social care assessment, or for voluntary sector help.
Poor levels of information provision and signposting have been reported, especially with regard to social care.5 ,6 Commissioners of health and social services have been advised not to focus exclusively on ‘high-end’ provision, but consider the long-term cost implications and benefits of more preventative approaches for Parkinson's disease, health and social care services.
Although there is a wealth of anecdotal evidence that low-level (smaller, less complex) social care interventions delivered early, can improve health outcomes and have a preventative impact for people living with Parkinson’s disease, there is little data or hard evidence to confirm these beliefs. Quantifying the health impact of social care for those with Parkinson's disease is difficult as no data is collected in social care ‘by condition’. However, people with Parkinson’s disease are more likely to have an unplanned or emergency admission to hospital. Reasons for admission include falls from altered gait and balance, pneumonia, urinary tract infection and psychiatric disturbances.6 ,7 Once in hospital, length of stay is longer for people with Parkinson's disease, and admission is more likely to have adverse consequences.6–9 These admissions and outcomes cannot be attributed exclusively to inappropriate levels or quality of social care. However, there is a need for evidence to understand what good-quality social care means for people with long-term conditions like Parkinson's disease, and how this can impact on health and health service use.
It is crucial for health professionals to understand how social care is valued and valuable to people with degenerative conditions such as Parkinson's disease. A better understanding of the interaction between social care and health outcomes could promote vigilance and encourage early detection of social care needs and timely referral. Integration of health and social care is high on political agendas. However, previous integrated service interventions have not demonstrated sustainable or sizable benefit.10 There is a call for increased awareness by health professionals, of what type of social care is valued by service users.5 This can contribute to the development of new, more effective models of integrated services.
This study aimed to address the current evidence gap and identify what constituted good-quality social care for people with Parkinson’s disease and their carers, and how this care was seen to benefit their health, quality of life and well-being.5 To achieve this aim, three questions were explored: (1) What are the health and well-being benefits of good-quality social care? (2) What characteristics does social care require in order to accrue those benefits? (3) What are the barriers to accessing good-quality social care, and therefore attaining the benefits identified?
This evidence is essential to inform healthcare professionals’ practice in order to detect and refer social care need as deemed appropriate. The evidence is timely to consider with regard to current debates on integration of health and social care at policy, professional and organisational levels.
Methods
Design
A qualitative collective case study methodology was used.11 ,12 This qualitative approach uses a small number of ‘cases’ to explore understanding, experiences and meaning in detail.11–14 Case study methodology has the capacity to capture detailed insights into how the provision of quality social care interventions impacts on health, well-being and quality of life from the perspective of people with Parkinson's disease, their carers and relevant service providers. In this study, in line with the methodology, four people with Parkinson's disease formed the ‘cases’.
Sample and setting
This study was undertaken in the north and midlands of England.
Purposive sampling was used to select cases for the study. Sampling criteria were developed in collaboration with Parkinson's UK to ensure variation in terms of gender, living circumstances (eg, housing, rural/urban), family and social connections, income and benefits, length and stage of Parkinson's disease, diagnosis and impact, care needs and provision. The case study included 17 individual interviews in total (table 1). In each of the four individual case studies, up to four additional interviews were conducted with people who could provide insight into formal or informal social support or care. These included social workers, information and support workers (ISW) (Parkinson's UK employees), care workers and informal carers such as family and friends (n=13).
Overview of case study and focus-group participants
Two focus groups were also conducted to expand on and verify the preliminary individual interview findings (table 1). One with people with Parkinson’s disease and their carers (n=17), and one with professionals (n=8). A further telephone interview was also conducted with a former health and social care commissioner who was unable to attend the focus group.
An overview of the individual and group interview participants is provided in table 1. A description of the four cases is presented in table 2. Pseudonyms are used throughout.
Description of the cases
Recruitment
Cases were initially contacted by Parkinson's UK ISWs. These are community-based support and advice staff who recruited from their caseload. The ISW sent the person with Parkinson's disease the study information sheet, and asked if they were interested in participating. On receiving their permission, the research team were informed, and they contacted the person directly to further discuss the study. Carers were identified by the person with Parkinson's disease, who was asked to identify individuals who could give insights about providing them with formal or informal support or care.
The focus groups were organised, and participants recruited by Parkinson's UK.
Data collection
Data were collected between October and December 2013.
Individual case studies
The in-depth interview with the person with Parkinson's disease was conducted in the person's home. In two of the case studies, by request of the participants, these interviews also included a carer (eg, husband) and/or family member (eg, daughter).
Carer interviews took place in the carer's home or by telephone, as appropriate, and in line with the participant's preference. All the interviews followed an interview schedule informed by literature and discussions with the Project Advisory Group. The schedule included questions on the support currently received, what they wanted and valued from social care, and the impact that social care had on their lives. Interviews with carers also focused on the nature and impact of the social care interventions from their perspective.
Focus groups
The focus groups took place in a community venue, neutral to the participants. Two researchers facilitated the discussion, and two others acted as scribes. The focus groups were guided by a topic guide generated from the preliminary findings of the case studies.
Ethical considerations
The study was approved by the university faculty Research Ethics Committee (REC). Following appropriate consultation, we were advised by NHS that REC approval was not required.
All participants were given an information sheet and were assured that their data would be treated confidentially. Written informed consent was obtained prior to any data collection.
Data analysis
With consent of the participants, all interviews and focus group discussions were digitally recorded, transcribed verbatim and anonymised. Data analysis used the ‘framework approach’ outlined by Ritchie and Spencer.15 Framework is commonly adopted in applied health and social care research. It provides a systematic process involving sifting, charting and sorting the data into key themes using five stages: familiarisation, developing a thematic, indexing, charting, and mapping and interpretation. A thematic framework was developed, shaped by the study's aims and questions. Each case study was analysed individually followed by cross-case and cross-theme analysis to identify key characteristics and themes.
Analysis was primarily conducted by three researchers. Following initial analysis by one researcher, the transcripts were then independently coded by another analyst. Data analysis meetings with the wider team were held to ensure that interpretation of themes was consistent.
Findings
findings are presented here under the headings that reflect the underpinning research questions: What are the benefits of social care, the components of good-quality social care and the barriers to accessing social care? Verbatim quotes are used to illustrate key points. Pseudonyms are used for the cases to protect anonymity.
Benefits of social care
‘Parkinson's aware’ social care generated physical, psychological, social and service/societal benefits (box 1 and figure 1), which were often inter-related. For example a benefit to the person with Parkinson’s disease (eg, improved safety) would have a physical benefit for the persons themselves, but may also reduce the psychological burden for the carer, or result in the avoidance of wider societal costs such as residential care or hospital admissions.
Benefits of social care
Psychological and societal
Researcher: If all that care [informal care] wasn't there how would life be?
Crap! In a word, crap! Because if I wasn't there she'd be in a home, and that would be her life! (Informal carer—focus group)
Physical and psychological
And he [husband/main carer] can go with the good days and the bad days, and he knows when she's more mobile, and when she has, you know, she's faced a lot of what she was saying dyskinesia. It can go on for hours where she's rolling around on the floor, and he can ignore that, knowing, and they know how she will be when she's gone through that. You know, it's that bond really and that relationship that is holding them together. Whereas when you see people in the communities who haven't got that kind of support you know that the deterioration is much more rapid. (Social care worker—case study 1)
Physical
Like this with her leg, I mean that could flare up to anything, whereas the district nurse came in and we caught it before it did get any worse. She's been having problem with her eye. And we've had a doctor out a couple of times, you know what I mean, but I brought that to her attention from the start. If it was left up to [Mrs Clark] she'd probably push that to one side a bit. (Carer—case study 2)
Psychological
Paid care enables [Mr Rogers] to live his life and social care makes it worth living.
Researcher: That's really good way of putting it actually and if that wasn't there?
Well I think he'd sink into a really grim depression frankly. I mean he does sometimes anyway…Sometimes I just can't imagine what's it's like at like four o'clock in the morning for him. (Friend—case study 4)
Social
If people like myself weren't around in his life, who are friends with him and would be going to pub sessions anyway, he would need a lot more of that kind of stuff…from formal care providers, but that's unlikely to come from more community care budgets because it would be a low priority, taking someone to the pub to play the guitar…despite the gigantic plus impact it has on his quality of life. (Friend—case study 4)

Benefits of social care. GP, general practitioner.
While some of these benefits take immediate effect, others have long-term implications and may result in prevented events (eg, live-in or residential care) and reductions in the need for increased health and social care resource in the future. In particular, the impact of prevented events was characterised in two ways—a reduction in the number of ‘crisis events’ for the person or their carers, and a slowing down of the trajectory of deterioration associated with good management of symptoms and complications.
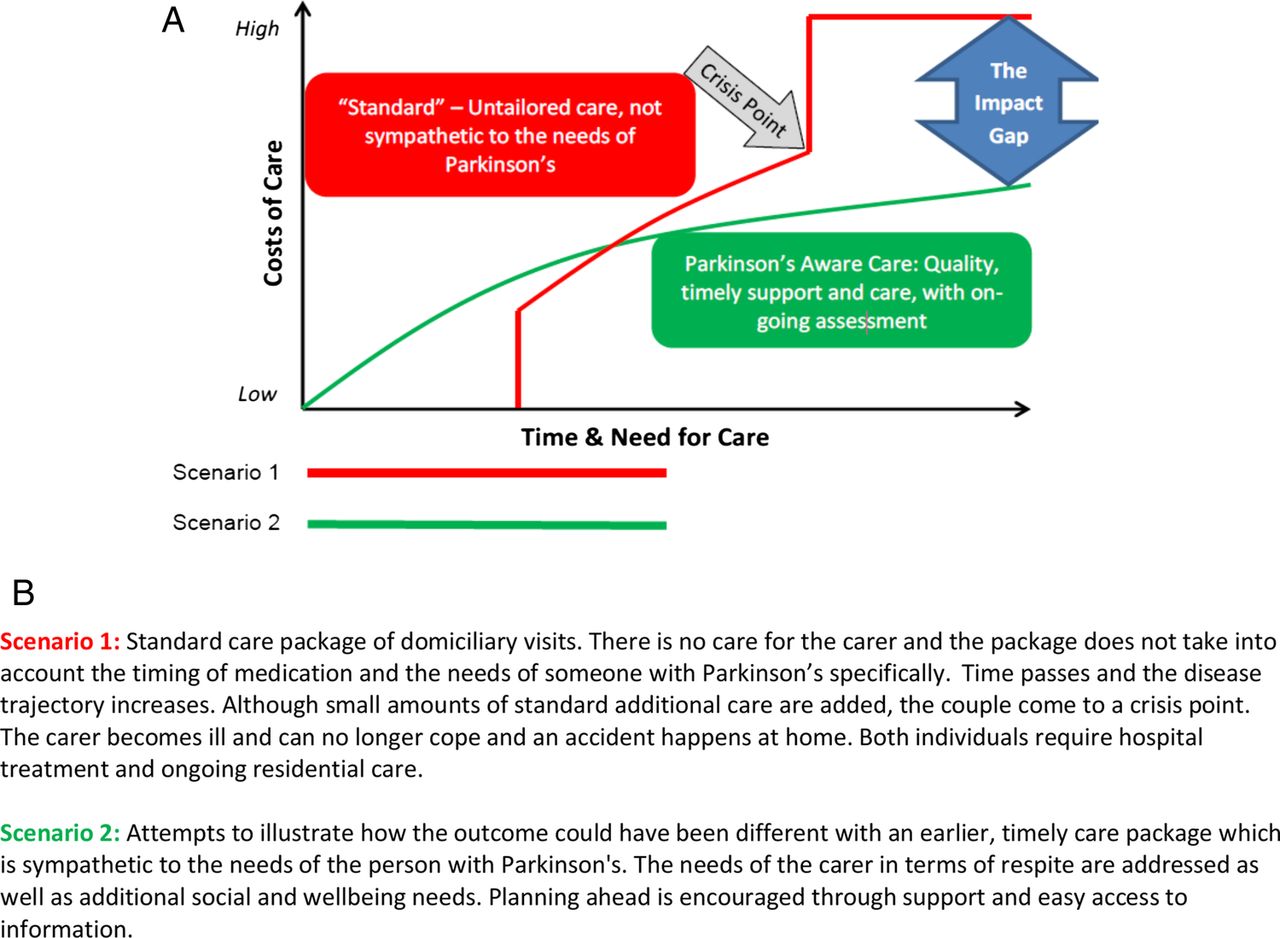
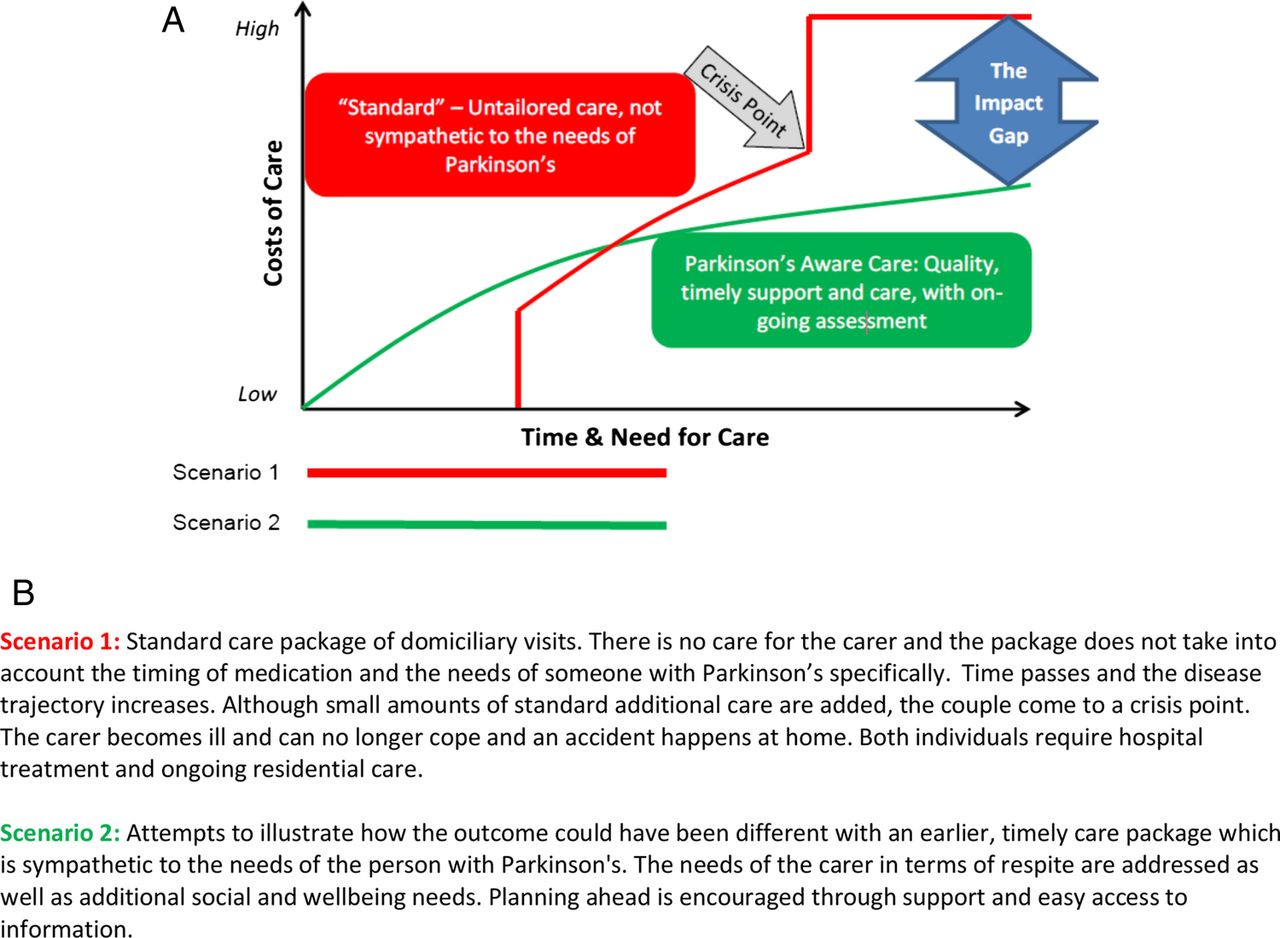
Through these findings, the concept of the ‘Impact Gap’ was developed (figure 2).
{kind=link}
{kind=link}
The Impact Gap (A) diagram and (B) scenarios.
This illustrates two possible outcomes using the same individual (a person with Parkinson's disease living with a partner who cares for them, but both are increasingly frail). The two scenarios highlight how the outcome is very different in terms of the need for expensive residential and hospital care, but importantly, the outcomes also differ vastly in terms of the psychosocial well-being and independence of the couple. The ‘Impact Gap’ demonstrates how the costs of care for people with Parkinson's disease may be offset by delivering good-quality social care (often initially small, low-cost packages) in a timely fashion, with on-going assessment.
Characteristics of good-quality social care
In order to attain the health, well-being and cost offsets described above, participants reported that social care had to have certain characteristics that indicated good quality. Some were general characteristics that apply whatever the medical condition a person has. Other characteristics are Parkinson's disease specific.
General social care characteristics
First, there was a wealth of evidence that the person with Parkinson's disease and/or their carer valued social care that gave them choice, control and enabled them to maintain their independence where possible (box 2).
General characteristics of good-quality social care
Choice, control and independence
Even though she's having still problems with that same arm, she was able to use the mobility scooter. So I thought that was good also that she's doing as much as she can do when she can do it really. (Social care worker—case study 1)
There's times when I'd like more help, but then again as I say I cherish my independence. (Person with Parkinson's—case study 3)
Continuity and flexibility
Some carers probably might go in and just do what is actually on the care plan, but then what you've got to realise is, with [Mrs Clark 2] being very independent, it probably says personal care, but [NAME] has actually got herself ready, has actually washed herself before I've got there. So that time that I'm allocated for that I can be doing other things to help her. (Care worker—case study 2)
I think they [Mr and Mrs Clark 2] could do with more help…but the thing is enabling them to do things as well, and maybe looking at care in terms of they still want to do some things, so why, instead of having a care package that says oh we do this that and the other, be a bit more changeable in well, I think I could manage to do this this week, but could you do this for me instead. So it's a bit, I don't know, a bit more rounded and a bit less regimented I suppose. (Daughter—case study 2)
Positive personal qualities of those providing care were also highly valued. Not only should they be reliable and respectful, but participants considered that formal carers should be an appropriate demographic (eg, age and gender) compatible with the person receiving the care. In addition, the importance of care workers seeing the person as a whole, rather than just a person with a health condition, was emphasised.
Overwhelmingly, continuity was seen as important in order to provide a consistent service from care workers familiar to the recipient. Study participants considered it important that carers came on time and gave the full amount of time allocated. Furthermore, flexibility of services was valued, as illustrated by the care received by case study 2 from a formal care worker (box 2).
Regular reassessment was also highlighted as important to ensure that individuals were receiving the most appropriate help and support.
Parkinson's disease-specific values
The Parkinson's disease-specific components of good-quality social care centred on the importance of ‘understanding Parkinson's’, particularly the symptoms relating to the condition (box 3). For some participants, employing carers through a direct payment scheme was thought to help ensure paid carers had some knowledge of the condition. However, this also often brought a lot of responsibility and pressure that some individuals did not wish to or feel able to take on.
Understanding Parkinson's disease
Symptoms
Recognising if you like all the different layers that Parkinson's presents, not just the kind of physical stuff that most people know about, like tremors and rigidity, but the psychological stuff, sort of the anxiety and depression, the kind of cognitive stuff about sometimes lacking organizing executive functions. (Friend—case study 4)
Fluctuating nature
Yes, you have to adjust because say I went to [Mrs Brown] this afternoon, and this morning she was on top form but this afternoon she had a wobble, because she doesn't walk around the house, she crawls around the house and clings like a toddler would to the side of the furniture. That frightens me a little bit because I've never had that, but I will say are you okay to do that, or would you like me to go and answer the phone? Because she is crawling across the floor to answer the phone. (Personal carer—case study 1)
Timing of medication
And the thing that concerned us most of all was the immediate drug regime. If a carer came in they'd need to understand what it was that she needed when she needed it. (Husband/carer—case study 1)
Synchronising care delivery
It's not necessary to have two carers to get someone up to give them their breakfast and then give them their medication. If you gave them their medication as soon as they put their feet on the floor they can reduce the carers to one care, and that sounds simple but I see it so many times. (Lead Parkinson's specialist nurse—focus group)
Giving person time
Even if you've only got 15 minutes to do it, don't fire questions at people…'Jack how are you feeling today? Give him a chance to answer, ‘what would you like for your breakfast? Give him a chance to answer…that could actually set the person up.
I agree, because it actually does cognitively set you in gear and that's what you need when you have PD. (Occupational therapists—focus groups)
Research what Parkinson's is all about because, without being rude, some people with Parkinson's appear as if they've got a learning disability and they certainly haven't. And I've found that people treat them with learning disabilities, and they haven't got it because they haven't got the time to listen to their answers, or hear the conversation. They just dismiss them instantly, so it's just researching really. (Personal carer—case study 1)
Regular reassessment
I don't think he needs the amount of contact hours that he's getting now, and this is again to do with the change in his treatment regime, but I think it's the quality…perhaps fewer hours but with someone who's better trained and more able to deal with the psychosocial aspects, alongside the practice stuff. (Friend—case study 4)
The findings indicated that, due to the fluctuating nature of Parkinson's disease (in terms of both physical and psychological symptoms), carers also needed to understand that the condition could vary in presentation on different days or times of day, and be able to accommodate and adjust care accordingly. This variability and unpredictability could cause difficulties when setting up or defending the level of care required in formal care packages.
Understanding the nature and importance of the medication that individuals with Parkinson's disease were taking was also crucial. Carers needed to be aware of the importance of taking medication at fixed times each day and respond to potential side effects (eg, hallucinations, dyskinesia). For example, this was a major concern for Mrs Brown's husband (case study 1) should anything happen to him in the future (box 3).
It was also noted that if carers were aware of the importance of synchronising care delivery with medication times this could yield benefits for care services as well as the person with Parkinson's disease in terms of resource provision and costs (box 3). In addition, participants emphasised that people with Parkinson's disease might require more time to answer a question or complete a task. This highlighted the importance of carers having an underpinning knowledge of Parkinson's disease, and allowing the appropriate time, and avoid overstimulating them. As people with Parkinson's disease may not require any social care at the point of diagnosis, regular reassessment was seen to be particularly important as the condition could deteriorate quite rapidly depending on the effectiveness of medication.
Barriers to accessing social care
The findings reveal a number of barriers that participants experienced in accessing social care. First, awareness of what social care was, what was required, and how it was accessed, was poor. As a result, accessing social care often happened by chance rather than in a systematic way. Often individuals did not know where to turn to start the process of getting help, and there was a strong sense of ‘you don't know what you don't know’ (box 4).
Barriers to accessing care
Awareness
I liken it to a pinball machine that you sort of hit against this or that or, you know, you get your information by happenchance and bumping into people and speaking to people. (Person with Parkinson’s—focus group)
There might be a whole raft of things out there that could benefit Mum and Dad or help them that I don't know about, because there's no one telling us what there is. (Daughter—case study 2)
Lack of planning
When I got to breaking point, I got everything.
Researcher: Right so you had to get to that breaking point.
Yeah…it shouldn't have got to that. (Carer—focus group)
It's left too much to chance and I feel it shouldn't be left to chance. Now I mean the unfortunate thing is at the time they diagnose it most people don't really need anything, and if you're very lucky it'll be many years before you do. But there ought to be a flag in there, there ought to be something to tell those organisations there's a potential problem here. (Husband/carer—case study 1)
Personal factors
I mean delaying accessing things is good…I really felt I was crossing a bit of a personal Rubicon when I started letting people in my house to do stuff for me who I didn't know…. I don't really like it really, because your privacy's gone out the window. (Person with Parkinson's—case study 4)
Champions and supporters
I think one of the things is it has been difficult to access the care, equipment, adaptations, and it seems to be every single thing has been difficult. But when things have eventually happened then there has been a big improvement. And I think a lot of people won't keep asking and keep asking and keep asking. (Daughter—case study 2)
Service logistics
When you're going out to assess somebody obviously best practice says you don't just do one visit to assess them, because of fluctuation conditions, whether it's dementia, whether it's MS, whatever it is you need to see people on different days, different weeks, different times, but that's not the way social services work anymore because of the budget restrictions and the fact that you've got to go out, hit your targets of doing four assessments a week whatever, I'm afraid that that seems to be going out the window. (Social worker—focus group)
From the perspective of the participants, individuals with Parkinson's disease and their carers often reached a crisis point before they tried to access help. It was evident that social care was generally not accessed in a timely fashion, which had a profound impact on health, well-being and quality of life (figure 2). There was consensus among many that there was a lack of planning, or ‘future proofing’, in terms of the support and help that people with Parkinson's disease might need. There were no reported instances of individuals being informed about, or offered social care support or information at the time of diagnosis. Awareness was therefore essential among both individuals with Parkinson's disease and their carers, but also among professionals (eg, general practitioners (GPs), social workers, ISWs) who needed to keep up-to-date about what was available. However, this was seen as very difficult because services were not stable, but constantly changing.
There was evidence that the process of finding out and accessing social care was influenced by personal factors within the individual or their family (eg, acceptance, striving to maintain independence for as long as possible). Furthermore, the presence or absence of champions and supporters, who helped individuals navigate the process, was key. For two of the case studies this was a family member. In another case study, the person with Parkinson's disease had the resources to be their own advocate. However, for the remaining case study there was no central advocate, and so only minimal services had been accessed and provided. Finally, various service/system logistics, such as budget cuts, services being squeezed, and a lack of integration between health and social care services acted as significant barriers.
Discussion
In this paper, we have presented findings that indicate what good-quality social care means to people with Parkinson's disease and their carers. It responds to a call for additional evidence from the perspective of service users.4 The findings illustrate how social care can have a benefit to health, quality of life and well-being, especially if delivered in a timely and appropriate manner. Importantly, the findings indicate that if social care is ‘Parkinson's aware’ and anticipatory in nature, the level of social care intervention required is lower. By increasing receipt of appropriate social care, preventable deterioration and complications may be avoided with a subsequent offset in health and social care costs. Of importance to health services is the long-term gain in terms of avoidable suffering, but also cost offsets, due to the illness and health episodes that are prevented. The Impact Gap diagram illustrates this point. The diagram also demonstrates how social care not provided or not tailored to the needs of Parkinson's disease is more likely to lead to a need for more expensive crisis intervention and high-end healthcare.
The findings indicate that certain barriers are encountered in accessing social care. These are: low levels of awareness to identify what social care was needed, how to access them, and how to plan ahead and avoid crisis. Additional personal factors, such as a drive to protect privacy also featured. Participant's experiences illustrate how services with characteristics of good social care can help to overcome these barriers and enable access in a timely fashion. Key examples include services that are delivered by people knowledgeable about the condition, see ‘the whole person’, and acknowledge personal preferences and values (eg, privacy), offer control, choice and continuity, and that understand the fluctuations and unpredictable nature of Parkinson's disease. Those without social support or family to help overcome barriers were compromised further in accessing social care. In addition, information about what services are available and how to access them needs to be available in accessible ways to different audiences, experiencing different barriers. One size is unlikely to fit all in terms of services provision, and in how to deliver information to prompt access. Experiences of participants in this study reveal that people ‘don't know what they don't know’, as certain stages of their journey. These findings also indicate how direct payments increase the control of some but inhibit access of Parkinson's disease-aware social care for others. For some, the direct payment process is not easy to understand or to manage, especially if living alone.
This study explains the benefit from good-quality social care experienced by family care givers as well as those with Parkinson's disease. Our findings also resonates with other research that reveals how, from diagnosis, enduring care demands can have a physical and emotional health consequence for the family carer.16 These consequences are aggravated by lack of service coordination and integration, difficulty in accessing information about services, and a lack of responsiveness by services.16
The study provides novel insight into how a person with Parkinson's disease may lack awareness of the whole trajectory of their illness and the associated future social care needs. They may be struggling to accept the diagnosis or in denial of the reality of their condition. These factors can blind someone to recognising a current or pending social care requirement for themselves or a family carer. Taken alongside the general lack of awareness of how to access social care and what is available, it is challenging for people with Parkinson's disease to get the help they need at a point when it will have a preventative impact. Arguably, this is where the contribution of health professionals can have the most impact, whether a GP, neurology specialist, district nurse or other staff group. Those working in healthcare have more awareness of the trajectory of conditions such as Parkinson's disease, and are well placed to signpost and support access to care for the patient or their family carers. In addition, clinicians can overcome reluctance or denial preventing people from acknowledging social care needs, by highlighting that it may reduce adverse events or delay deterioration and associated loss of independence. This study indicates that it is vital that those in healthcare do not assume social care is being accessed. Timely assessment by health professionals and referral to statutory or voluntary social care service providers can reduce the impact gap.
Comparing the experiences and requirements of health and social care in England is difficult, as formal social services, unlike health services, are not condition specific. However, the characteristics of good-quality social care identified in this study are similar to aspects of care recommended in guidelines and recommendation related to healthcare for people with Parkinson's disease, especially in relation to holistic care, addressing the fluctuations and unpredictability of Parkinson's disease and delivering care that is person-centreed.17–19 While aspirations regarding service characteristics for Parkinson's disease may be similar for health and social care, significant gaps have been highlighted across current health and social care provision in England.6 ,20 In addition, examples of good-quality healthcare, such as the Dutch Model, promotes integrated multidisciplinary teams, inclusive of health, social, domiciliary and home care staff.10 ,18 ,19 Such multidisciplinary services will work with patients and family to provide for their variable needs over the course of their condition. The findings from this study support the proposal that integrating health and social care, working in a holistic, person-centred manner will help to deliver care that is Parkinson's disease aware and overcomes the barriers identified.19
The Dutch Model19 provides an example of such an integrated approach. It provided education initially to physiotherapists, but has expanded this to include the broader multidisciplinary team, including social workers. The work of this ‘community’ promotes the empowerment of individuals with Parkinson's disease, and their carers’ aims to influence their own care provision, and has shown to improve health outcomes and reduce costs to services in that population.18 ,21
At the time of writing, health and social care integration is being fiercely discussed at a policy and organisational levels.22 ,23 New models of integration are emerging, but there is confusion about a clear way forward regarding integrated structures and processes.4 ,5 These findings draw attention to the importance of integration at a practice and professional level. A question remains regarding what systems and processes are required to facilitate this in the current environment, with pressures on both clinical time and funding. In addition, when services are in a state of flux or reconfiguration, clear strategies are needed to ensure that staff in both health and social care maintain current knowledge regarding availability of care across services.
To address this issue, Parkinson's UK have developed the Parkinson's Excellence Network, which is a partnership of health and social care professionals, with a strong service user voice. It echoes the findings here that support integrated working across health and social care in delivering Parkinson's disease-aware care in a timely manner.21
As new models of health and social care integration emerge, it is important to evaluate whether integration improves early, timely referral to appropriate social care, and what the impacts of these new integrated services are on health, quality of life and well-being of people with long-term conditions, such as Parkinson's disease. There is an urgent need for full economic analysis of the impact of Parkinson's disease-aware social care provision.
Limitations of this study
As a qualitative study, the main limitation of this research relates to generalisability. However, generalisability was not the purpose here. As with other qualitative studies, the aim here was to generate insight into a complex condition and identify associated service needs, where little current evidence exists, and where one size of service does not fit all. The case study approach, and diversity of our sampling, ensured inclusion of perspectives and experiences from a wide range of participants with different characteristics. This provides a multifaceted picture that would not have been available using survey or other observational methods.
The transferability of our findings is further strengthened by challenging and testing the findings from the case studies in group interviews. These allowed us to check the emerging findings for resonance among a wider group of participants.
Finally, as social care is a devolved issue, and the study focused on the experiences of those in receipt of social care in England, the findings are directed at audiences in England. However, the messages are likely to be of interest to audiences in the rest of the UK and beyond, especially those countries currently reviewing or testing different models of health and social care integration.
Conclusions
This study describes how good-quality social care can enhance the health of people with Parkinson's disease. The research demonstrated, very powerfully, the need for social care packages sympathetic to those with neurological disorders such as Parkinson's disease. It demonstrates how good-quality social care, integrated with healthcare, can impact on quality of life and well-being, and what this could mean in terms of the escalating need for care and the cost of care. The findings indicate that in order to achieve improved outcomes for those with Parkinson's disease and their carers, some behaviour changes are required by significant stakeholders, including individual clinicians and practitioners. However, the systems and processes need to be in place to support easy assessment for, referral to and receipt of health and social care services that are Parkinson's disease aware and anticipatory in nature.
Acknowledgments
The research team would like to thank Parkinson’s UK for funding the study and for the advice and support of Donna O’Brien and Sarah Gray from Parkinson’s UK. Dr Oliver Bandmann (Sheffield Teaching Hospitals NHS Foundation Trust), Joanne Rose (Rotherham NHS Foundation Trust), Pamela Goff, (Sheffield Branch, Parkinson's UK) and Errol Guest (Doncaster Support Group, Parkinson's UK) for their valuable advice, expertise and contributions on the Project Advisory Group. The authors would like to express their thanks especially to the participants of the study. They are very grateful to all the participants for their willingness to share their experiences and views.
Footnotes
Contributors The article is based on a project designed by AMT, AM, A-JS and MW. Data was collected mainly by BW and FK, supported by the other authors. All authors contributed to the analysis but was led by FK, AM, AS and BW. AS led the development of the Impact Gap model. AMT and FK produced the final draft of the paper, but all authors commented and contributed to the earlier drafts.
Funding Parkinson's UK.
Competing interests None declared.
Ethics approval Ethical approval was obtained from Sheffield Hallam University Research Ethics Committee (Faculty of Health and Wellbeing).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Anonymised data will be made available on request to the corresponding author at angela.tod@manchester.ac.uk