Article Text

Abstract
Objectives Response rate in public health programmes may be a limiting factor. It is important to first consider their delivery and acceptability for the target. This study aimed at determining individual and unit-related factors associated with increased odds of non-response based on hepatitis C virus screening in primary healthcare.
Design Primary healthcare units (PHCUs) were extracted from the Register of Health Care Centres. Each of the PHCUs was to enrol adult patients selected on a random basis. Data on the recruitment of PHCUs and patients were analysed. Multilevel modelling was applied to investigate individual and unit-related factors associated with non-response. Multilevel logistic model was developed with fixed effects and only a random intercept for the unit. Preliminary analysis included a random effect for unit and each of the individual or PHCU covariates separately. For each of the PHCU covariates, we applied a two-level model with individual covariates, unit random effect and a single fixed effect of this unit covariate.
Setting This study was conducted in primary care units in selected provinces in Poland.
Participants A total of 242 PHCUs and 24 480 adults were invited. Of them, 44 PHCUs and 20 939 patients agreed to participate. Both PHCUs and patients were randomly selected.
Results Data on 44 PHCUs and 24 480 patients were analysed. PHCU-level factors and recruitment strategies were important predictors of non-response. Unit random effect was significant in all models. Larger and private units reported higher non-response rates, while for those with a history of running public health programmes the odds of non-response was lower. Proactive recruitment, more working hours devoted to the project and patient resulted in higher acceptance of the project. Higher number of personnel had no such effect.
Conclusions Prior to the implementation of public health programme, several factors that could hinder its execution should be addressed.
- PREVENTIVE MEDICINE
- PRIMARY CARE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first in-depth study of the experiences of primary care units concerning the delivery and acceptability of public health programmes in Poland.
This study was carried out on a large and representative sample of primary care units and patients.
Participating primary healthcare units (PHCUs) could differ from non-participating PHCUs which could have an effect on high response rates observed in study population.
Methods of sampling of patients employed by PHCUs were not universal which could have resulted in differences in response rates observed.
Owing to a small number of PHCUs, we were not able to study the independent effects of all unit-level factors.
Background
Screening is a widely adopted instrument in the secondary prevention of asymptomatic chronic diseases. In general, it offers an optimal way to ensure earlier, more effective treatment and, consequently, avoid late complications of disease.1–3 Nevertheless, screening programmes should be designed in a way to avoid overdiagnosis and overtreatment.4 Several infectious diseases, for example, viral hepatitis, HIV, chlamydia infections are also candidates for screening programmes. Additional advantage of early detection consists in preventing an onward transmission and reinfections.5–7 Effectiveness of screening depends, inter alia, on its acceptability for the target population. It is important to first investigate healthcare system capacity and public acceptance of the programme.8 ,9
Even well-organised programmes may fail to succeed due to, for example, low coverage rates with an example being the population-based cervical cancer (CC) screening in Poland. It was introduced in 2007; however, CC incidence (15.3) and mortality (7.4) rates in 2012 still exceeded the average rate for the European Union countries (11.3; 3.7).10 Low coverage rate may result from ineffective invitation.11 ,12
Introduction of screening programmes into primary healthcare (PHC) may be a solution. There is evidence confirming the effectiveness of these settings in reaching the target population.13–17 Involvement of PHC allows for reaching those most at risk who tend to have poorer access to healthcare.18 Generally, healthcare system based on PHC is more efficient in tackling health inequalities.19–21
Poland adopted healthcare system model based on primary care in 1994. Since then, the role of general practitioners is promoted.22 High potential of PHC, however, still seems to be underestimated. The role of PHC is poorly described in policy documents.23 Notably, the role of PHC concerning public health interventions is rather limited with only a few preventive programmes conducted.24 On the other hand, there is a high accessibility of primary care services. More than 70% of population take advantage of them.25 Greater engagement of PHC in public health programmes could enhance their coverage.
This study aimed at determining individual and unit-based factors associated with increased odds of non-response in hepatitis C virus (HCV) screening in primary health care units (PHCUs). HCV testing was offered to randomly selected individuals registered to participating units. Understanding of factors driving non-response rates in HCV screening programme in PHC would enhance hepatitis C prevention. It would also allow anticipating barriers in future public health programmes and propose models improving their coverage.
Methods
Study design
This study is a part of ongoing project ‘Improvement of HCV diagnostics, estimation of HCV prevalence in general population and analysis of factors associated with HCV prevalence’ within the ‘Prevention of HCV Infections’ programme which was approved by the Ethics Committee at the National Institute of Public Health-National Institute of Hygiene (NIPH-NIH; Warsaw, Poland). Our study is a post hoc analysis of data collected for the purpose of evaluation of the project. Individual variables were determined before the study started.
Recruitment procedure
PHCUs
Sampling frame consisted of all PHCUs located in 10 (out of 16) Polish provinces (dolnośląskie, kujawsko-pomorskie, lubelskie, łódzkie, małopolskie, mazowieckie, podkarpackie, podlaskie, pomorskie, zachodniopomorskie). All eligible units were extracted from the Register of Health Care Centres. Sampling was performed, using the mathematical function ‘RAND’ in Excel. Each PHCU was attributed a random value (0≤v<1.0). Then, data were sorted from the lowest to the highest numbers. First 12 PHCUs on the list were contacted. PHCUs were informed that they would be rewarded for each patient recruited (€13 per patient and additional €26 for HCV-infected patient; EUR*=PLN4.26). Payment was transferred to the PHCU's account. PHCUs were encouraged to use these resources to ensure the most efficient implementation of the programme. They were not, however, requested to provide information how and if these funds were distributed to personnel. Other units were invited if there was refusal or non-response to invitation.
Patients
Each PHCU selected adults from their list of patients. Exclusion criteria were: age <18 years and diagnosis of hepatitis C provided patient was under infectious disease specialist control. Systematic sampling was performed by PHCUs to obtain the list of potential participants. Each PHCU had to declare the number of potential participants (200–800 persons; 400 on average) based on the capabilities of PHCUs and the total population served. The proportion of selected individuals out of the total population differed substantially between the PHCUs (from 1% to 58%). In the majority of cases, it accounted for <10% (55%) of the total population served. PHCUs were instructed on possible methods of patient sampling; however, they were not induced to employ one standard as organisation of patients registries varied widely between PHCUs, ranging from electronic to paper-based, specific to primary care unit or a part of general list in case of multispecialty facilities (different sorting strategies). Therefore, specific method of patient sampling had to be adapted to local registries. The majority of PHCUs (66%) relied on Nth name selection technique, that is, every Nth patient (eg, every 5th or every 10th, the N depended on the size of the population served and the number of declared patients) on the list was selected to be contacted. The modifications of this procedure included stratification of sampling (by the regularity of visits to focus telephone recruitment on those who do not visit PHCUs regularly or by the demographic feature, eg, year of birth). Some units were able to apply random sampling. Recruitment of volunteers was not allowed.
Selected patients were contacted using telephone, letter, short message service or face-to-face contact. At least three attempts were recommended for telephone-based contact at different hours. Face-to-face contact was attempted if a patient visited a PHCU due to other reasons or if the study nurse was attending another patient living in the vicinity of that patient (small communities).
During the first contact, a patient was informed on the study and invited to participate. At this stage, patient's eligibility was verified. If a patient met the inclusion criteria, the date of first visit was arranged. Contrary to PHCUs, patients were not paid or rewarded in any other manner for their participation in the study. During such visit, patients were first to provide informed written consent. Then, they were assigned an anonymous identification number, provided a leaflet and counselled on HCV infection. Patients were also to fill in questionnaire on exposures to HCV in non-medical and medical settings. Then, a blood sample was collected for HCV testing. Samples were processed using enzyme immunoassay (EIA). PCR was carried out for reactive samples. Patients were informed when they could receive their test result. HCV-infected individuals attended follow-up visit. Serum samples were processed in the Department of Virology of the NIPH-NIH.
Data collection
Data on PHCUs were derived from the Register of Health Care Centres and collected during on-site monitoring visits. Such visits were conducted by the coordinators to gather information on the programme's acceptability, challenges, etc. These visits were planned in PHCUs that had already recruited 50% of patients or less in case of identified difficulties. PHCU personnel were requested to describe their recruitment process and experience in running public health programmes.
The database of invitations from 44 randomly selected PHCUs was analysed. Information on invitation results were documented, using a special data format. Provided a patient refused to participate in the project during the first or next contacts, the recorder was to note the basic information (age, gender, place of residence, date of contact and reason of refusal). Other information such as socioeconomic factors (eg, education, income) was not included in the database used for this analysis. These data were gathered only for patients who agreed to participate in the study. Each PHCU was asked to send an anonymised list of individuals invited on a weekly basis.
Definition of the variables
Mode of invitation was determined on the basis of interviews with personnel. We defined passive modes of invitation as traditional mail or short message service, active as telephone invitation or in person invitation when a person attended the unit for some other reason and very active as using personal contacts and community nurses to recruit patients directly from households. Since only one PHCU relied solely on passive invitation modes and the majority of units used mixed strategies, we classified unit invitation modes into the following categories: passive-active (using passive modes in parallel to active modes or using passive modes at the beginning), active and active-very active (using active modes in parallel to very active).
Information on the project was disseminated through its website and media. Furthermore, PHCUs were provided with information leaflets. They could also propagate the project locally, using their own website, through local events, etc. If any of these additional activities were undertaken, the PHCU was classified as having local promotion programme.
The total working time devoted to a patient was not measured directly. To estimate the time spent per patient, we used the recruitment monitoring data (number of patients invited and number of weeks of effective recruitment). Weeks in which the recruitment was suspended (eg, due to holidays) were excluded from final calculations. Additionally, each unit estimated the overall number of working hours devoted to the project in a week. The time spent per person was calculated by dividing the weekly workload by the average number of patients invited per week.
PHCUs were also questioned about the implementation of public health programmes in the past. Public health programmes were defined as any forms of public health activities separately funded and monitored.
Statistical analysis
Since both individual-level and PHCU-level factors associated with non-response were analysed, multilevel modelling was applied. Individual covariates included age, gender and place of residence. PHCU-level covariates involved ownership, the number of patients registered, prior experience in public health programmes, presence of local promotion programme, mode of invitation, number of personnel involved and number of working hours per patient.
A multilevel logistic model was developed with fixed effects and only a random intercept for the unit. Preliminary analysis included a random effect for unit and each of the individual-level or PHCU-level covariates separately. Owing to a small number of PHCUs, construction of a single model accounting for all PHCU's variables was not feasible. For each PHCU-level covariates, we applied a two-level model with individual-level covariates, unit random effect and a single fixed effect of this unit-level covariate.
Laboratory methods
Serum samples were processed using EIA (Cobas e 411, Roche). Samples that were repeatedly reactive were subject to PCR (Qiagen).
Anti-HCV and HCV RNA prevalence were calculated relating the number of anti-HCV and HCV RNA-positive individuals to the total population. We calculated crude prevalence and prevalence standardised to the year of birth and gender distribution in the population of Poland as of 2014.
Detailed analysis on the prevalence and related factors was beyond the scope of this article and will be reported separately.
Results
PHCUs
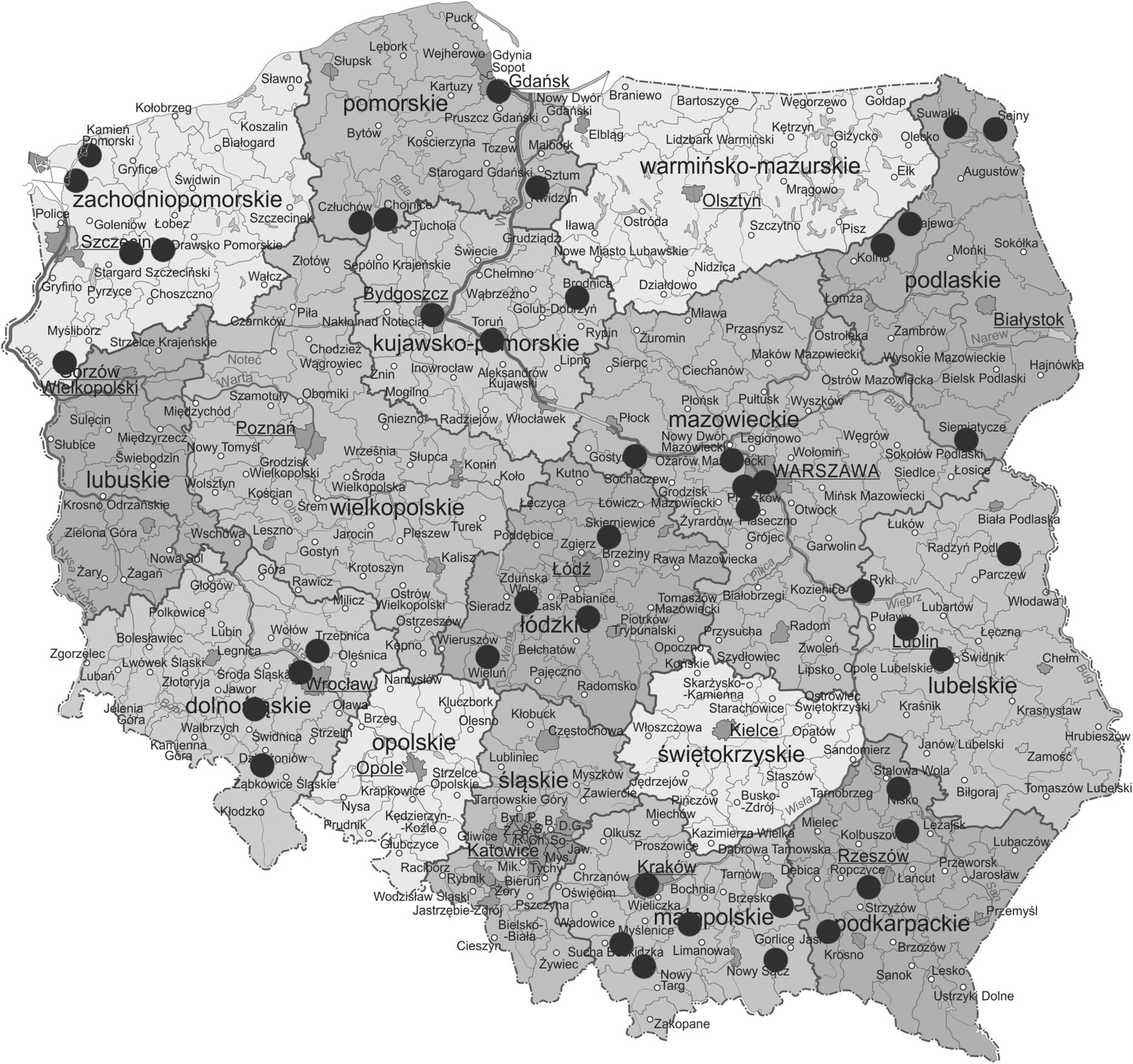
Between November 2012 and April 2014, 242 PHCUs were invited (telephone, fax, letter, email). Each PHCU was given 2 weeks for consideration and then recontacted. Of the 242 PHCUs, 98 (40%) refused, 91 (38%) did not provide their final decision and 53 (22%) agreed to participate in the study, but then 9 of them resigned. Finally, 44 PHCUs (18%) were enrolled (figure 1).
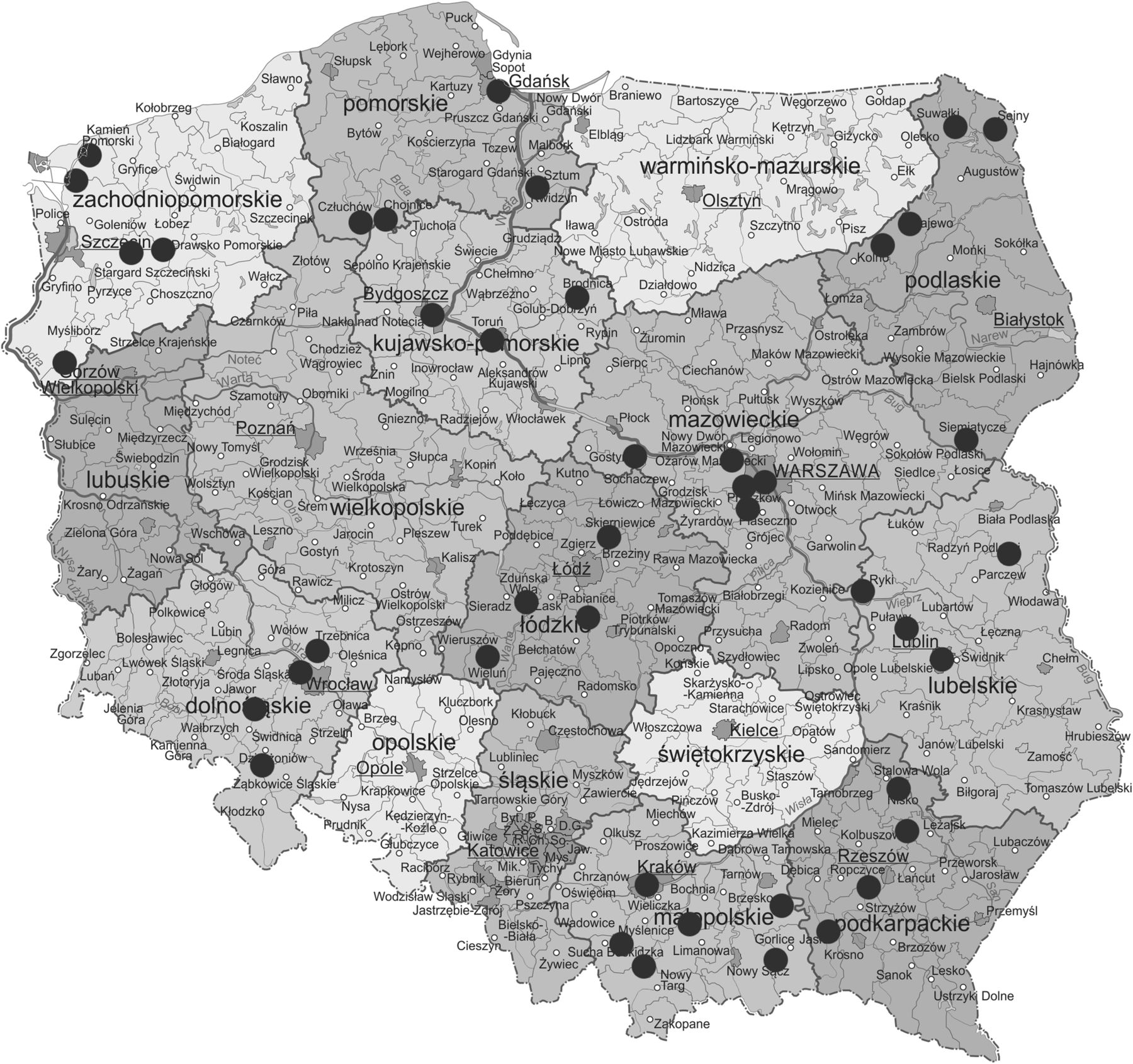
Locations of primary health care units enrolled in the study.
Each of the 44 PHCUs was required to attend training on the project's procedure (table 1).
Characteristics of PHCUs and recruitment process
The majority of them were medium-sized units (2500–9999 patients registered; 56.8%) and privately owned (81.8%). Over 90% had prior experience in running public health programmes. Only a quarter of the units tried to implement passive recruitment strategies and only one relied on letter-based invitations. The burden of the project was assessed at 7 hours/week on average. Most of the PHCUs assigned up to two persons who coordinated the project (most often nurses).
Patients
Between March 2013 and March 2015, 24 480 individuals aged between 18 and 94 years (median 48.5 years) were invited (figure 2).

{kind=link}
{kind=link}
Study population. HCV, hepatitis C virus; PHCU, primary healthcare unit.
Of note, 64% of them were women and the majority lived in rural areas (46.7%) or small towns (<20 000 inhabitants; 18.2%; table 2).
Characteristics of study population
Factors related to non-response
Of all individuals, 20 939 (85.5%) agreed to participate in the study. The non-response rate was relatively low, that is, 14.5%.
Factors associated with non-response are presented in table 3.
Factors associated with increased odds of non-response
Adjusted for the population structure (age, gender, place of residence), PHCU-level factors and recruitment strategies were important predictors of non-response. Unit random effect was significant in all models. Larger and private units reported higher non-response rates. For those with a history of running public health programmes, the odds of non-response was lower (adjusted OR (aOR)=0.8, 95% CI 0.7 to 0.9). Proactive recruitment (aOR=0.6, 95% CI 0.5 to 0.6), more working hours (≥10 hours/ week) devoted to the project (aOR=0.7, 95% CI 0.7 to 0.8) and the patient (≥1 vs <0.5 hour/patient: aOR=0.1, 95% CI 0.02 to 0.8) resulted in its higher acceptance. Higher number of personnel had no such effect. Moreover, having corrected for individual-level factors, the province where the unit was located was not a significant predictor of non-response.
Additionally, reasons of non-response were investigated. Predominant reasons of non-response were lack of interest (1843/3541; 52%) and failure to contact the patient (1455/3541; 41%). Other reasons were less notable, including lack of time (99/3541; 2.8%), testing performed in the past (95/3541; 2.7%), fear for testing or its result (31/3541; 0.9%) and other reasons beyond patient's control (22/3541; 0.6%) with the examples being comorbidities and age precluding patient from attending the visit.
HCV prevalence
A total of 228 (1.10%) anti-HCV and 99 (0.43%) HCV RNA-positive individuals were detected. Standardised prevalence of anti-HCV and HCV RNA were 1.14% (95% CI 0.94% to 1.39%) and 0.56% (95% CI 0.41% to 0.74%), respectively.
Discussion
This study reports on factors related to non-response rates in HCV screening programme in PHC in Poland. The non-response rate in the study was low (14.5%) indicating its relatively high acceptability. Having acknowledged that individual and unit-related factors may be influential, we were able to identify more challenging settings and the positive impact of personnel engagement. These findings suggest possible ways to improve the execution of screening programmes in PHC.
High response rate in programmes implemented in primary care is compliant with the findings of the literature data. Many developed countries (the UK, Canada, the USA) underline the benefits resulting from screening conducted by general practitioners.26–28 Primary care offers relatively high level of care and provision of comprehensive range of services as illustrated by the countries which empowered PHC (eg, Denmark, Spain and the UK).29 It is especially relevant for the delivery of public health services, including population screening. From a systematic review and meta-analysis of targeted HCV testing interventions results that direct strategies (eg, risk assessment and/or screening offered by personnel) were of higher effectiveness compared with the general strategies (eg, leaflets, posters, TV and radio spots).30–32 Additionally, such a low non-response rate may result from the fact that PHCUs were paid for each patient enrolled. Evaluation of ongoing cancer screening programmes showed much lower response rates11 ,33 which could be brought up to the levels similar to our study with more proactive approach.34 We speculate that the direct payment associated with patient recruitment intensified the efforts to convince patients to participate in the programme. Furthermore, a short period predicted for the execution of the project could also have an effect on personnel motivation. We have to underline that the effort made by the personnel to recruit the patients from the list largely exceeded what can be expected on the routine bases. We showed the significant personnel time involvement. It was possible on a short time basis and with a financial incentive, but very likely would not be achievable in ongoing programmes. Moreover, we experienced a large non-response rate in PCHUs invited to take part in the project which could have resulted in self-selection of more motivated units. Its short duration could also prompt patients to take part in the study.
Prior experience in running public health programmes contributed to increased response rate. This underlines the role of gaining the experience, but also, potentially, increased health awareness of the population served.
Analysis of PHCU-level factors showed that private (aOR=1.2, 95% CI 1.0 to 1.3), and large units (2500–9999: aOR=3.6, 95% CI 2.8 to 4.4 and ≥10 000: aOR=2.3, 95% CI 1.8 to 2.9) were more likely to note non-response. It may be indicative of better communication between healthcare providers and patients in public units rendering services for smaller populations. Possibly, healthcare workers may devote more time to provide the patient with information required to make an informed decision. Higher number of working hours per patient (0.5 to <1 hour: aOR=0.7, 95% CI 0.2 to 2.8 and ≥1 hour: aOR=0.1, 95% CI 0.02 to 0.8) resulted in higher response rates indicating that at least 0.5 hour (preferably ≥1 hour) per patient should be allotted.
Channels of communication should also be considered. Information on the project was mainly disseminated via classic modes. Internet-based (websites, email) or mobile-based communication (SMS) was used by few PHCUs. As expected, we noted an increased risk of non-response in case of passive contact modes. Having considered lower non-response rates in PHCUs who adopted proactive recruitment, direct contact with patients should be emphasised. Literature data also provide evidence of higher effectiveness of proactive approach.35 We also noted that the implementation of local promotion of the programme was associated with lower response rates. As no precise data were available, we cannot exclude that this finding reflects the fact that programme promotion was implemented in response to unsatisfactory response rates.
Individual-level factors demonstrated that living in urban areas (≥500 000: aOR=1.6, 95% CI 1.4 to 1.8), male gender (aOR=1.9, 95% CI 1.8 to 2.1) and age under 45 years (aOR=1.5, 95% CI 1.4 to 1.6) substantially predicted non-response in the study. Literature data also provide evidence for possible disparities in response with regard to gender, age, etc.36 At the same time surveillance data indicate that reaching young people, especially men, may be crucial to control HCV burden. European Centre for Disease Prevention and Control (ECDC) data as of 2014 suggest that hepatitis C is more frequent in males (male-to-female ratio: 1.8:1). Furthermore, individuals aged 25–44 years were the most affected group (51.3%) and 8% of cases were aged <25 years.37 Available data show that the prevalence of HCV infection in the general population in Poland is about 0.6% (200 000 individuals).38 ,39 Moreover, routine surveillance data suggest that HCV incidence in young men, who were the most resistant to take part in our study, is higher. Furthermore, unlike in many European countries, HCV infections in Poland are not concentrated in specific risk groups (eg, people who inject drugs).40 This suggests a necessity of screening in the general population, potentially with more effort placed on the recruitment of younger men.
Having considered that the most common reason of refusal was the lack of interest, it may be speculated that men and younger individuals are less interested in their health, at least with regard to HCV infection. Low response rate in younger population may also result from logistic barriers, defined as non-flexibility of PHCU's and patient's working schedule, which may hinder communication and arrangement of visit. In the era of modern communication technology, it may be also presumed that attempts to invite young individuals failed as they were not tailored to appropriate communication channels.41 Thus, it would be advisable to verify the effectiveness of novel technologies (eg, social media).42 It may be concluded that prior to the implementation of project, PHCUs should investigate opinions of potential responders on communication preferences to ensure its effectiveness.43
A limitation of our study may be associated with the fact that efficient PHCUs could have been over-represented in our study. Such hypothesis may be strengthened by the long period of recruitment of PHCUs and high non-response rate observed. PHCUs who agreed to participate in the study had to differ from non-participating PHCUs in terms of involvement in public health initiatives and efficacy of their execution. Another limitation may result from the fact that the method of patient sampling employed by PHCUs was not universal. It could have an effect on high response rates; however, it was not feasible to impose one standard method of sampling on PHCUs. Moreover, PHCUs were instructed that they could not rely on the recruitment of volunteers. Furthermore, 41% of all non-responders could not be contacted. Since only a small proportion of them were due to working or studying in another city or abroad, we included this group in the analysis as it may substantially limit the coverage of public health interventions. Additionally, due to the small number of PHCUs, we were unable to study the independent effects of all unit-level factors. Moreover, we could not investigate other predictors which could be useful to identify specific groups who respond poorly to screening programmes. However, we were only allowed to collect basic information on non-responders available through the registration database.
In conclusion, our results suggest that individual and PHCU-related factors may considerably affect response rates in public health programmes. Actually, some of them may constitute strong predictors of non-response. Thus, it is important to identify such factors and address them in an appropriate manner. Irrespective of the difficulties encountered by PHCUs, it seems to be a very effective setting for the detection of HCV infections. It may result from better physician–patient communication and recognition of local population which ensures intervention targeting. On the other hand, there is evidence of experience and knowledge deficits in the management of HCV cases among general practitioners.44 Therefore, special efforts should be undertaken to expand their competences. Evaluation of factors associated with increased odds of non-response in the project revealed several elements that could be resolved in future public health programmes.
Conclusions
Based on the results of the ongoing project, we can present the following conclusions:
Individuals living in urban areas, especially young men, constitute a group for which it is required to develop better communication strategies. They were represented to the largest extent in the group of non-responders.
Prior to the implementation of public health programme, if possible, PHCU's capacity to manage new tasks should be investigated.
Having considered the heterogeneity of patients (age, gender, place of residence) targeted for public health interventions, an emphasis should be put on recruitment strategies, tailoring and marketing messages.
Acknowledgments
The authors would like to acknowledge the colleagues from Primary Health Care Units who participated in the study.
References
Footnotes
Contributors NP collected the data, prepared the database for the analysis, elaborated the draft version of the manuscript and coordinated the works on manuscript. MS provided input and comments to manuscript. KZ participated in laboratory data processing, provided input and comments to manuscript. KM participated in laboratory data processing, provided comments to manuscript. AK and PG carried out laboratory testing, provided comments to manuscript. MR coordinated the study, participated in the design of the study, conducted the statistical analysis, provided input and comments to manuscript. All authors read, revised and approved the final version of manuscript.
Funding This work was supported by grant number KIK 35 ‘Prevention of HCV Infections’ from Switzerland through the Swiss Contribution to the enlarged European Union and the Minister of Health of the Republic of Poland.
Competing interests None declared.
Ethics approval The Ethics Committee of the National Institute of Public Health—National Institute of Hygiene in Warsaw (no. 6/2012 as of 4th October 2012) approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.