Article Text

Abstract
Objectives Many studies have investigated multimorbidity, whose prevalence varies according to settings and data sources. However, few studies on this topic have been conducted in Italy, a country with universal healthcare and one of the most aged populations in the world. The aim of this study was to estimate the prevalence of multimorbidity in a Northern Italian region, to investigate its distribution by age, gender and citizenship and to analyse the correlations of diseases.
Design Cross-sectional study based on administrative data.
Setting Emilia-Romagna, an Italian region with ∼4.4 million inhabitants, of which almost one-fourth are aged ≥65 years.
Participants All adults residing in Emilia-Romagna on 31 December 2012. Hospitalisations, drug prescriptions and contacts with community mental health services from 2003 to 2012 were traced to identify the presence of 17 physical and 9 mental health disorders.
Primary and secondary outcome measures Descriptive analysis of differences in the prevalence of multimorbidity in relation to age, gender and citizenship. The correlations of diseases were analysed using exploratory factor analysis.
Results The study population included 622 026 men and 751 011women, with a mean age of 66.4 years. Patients with multimorbidity were 33.5% in 75 years and >60% among patients aged ≥90 years; among patients aged ≥65 years, the proportion of multimorbidity was 39.9%. After standardisation by age and gender, multimorbidity was significantly more frequent among Italian citizens than among immigrants. Factor analysis identified 5 multimorbidity patterns: (1) psychiatric disorders, (2) cardiovascular, renal, pulmonary and cerebrovascular diseases, (3) neurological diseases, (4) liver diseases, AIDS/HIV and substance abuse and (5) tumours.
Conclusions Multimorbidity was highly prevalent in Emilia-Romagna and strongly associated with age. This finding highlights the need for healthcare providers to adopt individualised care plans and ensure continuity of care.
- EPIDEMIOLOGY
- PRIMARY CARE
- PUBLIC HEALTH
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study conducted in Italy to assess the prevalence and pattern of multimorbidity and its distribution by age, gender and citizenship.
This is a population-based study comprising all adults residing in the region of Emilia-Romagna, a large Italian region with ∼4.4 million inhabitants, of which almost one-fourth are aged ≥65 years and >10% are foreign citizens.
The use of administrative data may have underestimated multimorbidity, as they do not include primary care data.
Introduction
In the past decades, multimorbidity, that is, the co-occurrence of at least two chronic conditions in one individual, has increasingly become a challenge for healthcare services.1
Barnett et al2 estimated that, in Scotland, almost one-fourth of all individuals, and more than half of those with a chronic disorder, have multimorbidity. Multimorbidity is more common among women and older people,3 and is now considered the most prevalent chronic health condition in the overall population.4
It has been reported that people with multimorbidity have poorer quality of life and worse outcomes,5 and are frequent users of healthcare services.6 In fact, the treatment of multimorbidity results in high healthcare costs and involves multiple professionals. However, although many clinical guidelines are available for the management of specific chronic conditions, such as hypertension, diabetes and heart failure, there is a lack of evidence-based integrated treatments for patients with multiple diseases.7 So, the treatment of multimorbidity would require a holistic approach to cope with patients' complex healthcare needs,8 ,9 and continuity of care should be ensured to multimorbid patients.10 ,11 Primary care has thus a key role in managing multimorbidity, as it is person-focused rather than disease-focused, it is continuous over time and co-ordinates specialist care when necessary.12 ,13
Many studies were conducted to investigate the prevalence of multimorbidity in different countries, but results may differ according to the diseases considered, the age of the population, settings and data sources.3 Of note, few studies on this topic have been conducted in Italy, a country with universal healthcare and one of the most aged populations in the world.
The aim of the present study was to estimate the prevalence of multimorbidity in Emilia-Romagna (Italy), to investigate its distribution by age, gender and citizenship and to analyse the correlations of diseases.
Methods
Study design and participants
This cross-sectional study is based on demographic and clinical data retrieved from five data sources linked using the patient's identification code:
The hospital discharge record (HDR) database, which includes demographic characteristics, admission referral source, admission and discharge dates, main diagnosis, up to five secondary diagnoses, up to six interventions (identified using the ICD-9-CM coding system) and discharge status. HDRs are sent by all public and private hospitals to the Regional Authority and on a regular basis from the Regional Authority to the Ministry of Health after data quality control. Since 1995, the diagnosis-related group system has been systematically used to allocate funds to hospitals and to monitor quality of care and outcomes.
The mental health information system. This register was implemented in 2005 for administrative and clinical epidemiological purposes. All adult patients who have at least one contact with the community mental health centres (CMHCs) are recorded in the database, which includes demographic characteristics, the ICD-9-CM diagnosis and information of each type of intervention administered.
Residential mental healthcare discharge records, a database active since 2008 that includes mandatory information on patients discharged from non-profit or accredited private facilities, that is, admission and discharge dates, main diagnosis and discharge status. Accredited facilities are private hospitals where fees are reimbursed by the Italian National Health Service if the patient is an official resident in Italy.
The outpatient pharmaceutical database, which contains information on patients' gender and age, prescriptions (substance name, ATC System code—V.2013, trade name, date of prescription filling and number of packages) and prescribers. This register includes drugs reimbursed by the healthcare system that are prescribed by the general practitioner or a specialist, or directly delivered by the hospital pharmacies.
The regional mortality register database, which contains information on patients' demographic characteristics as well as date, place and cause of death. This database was used to identify patients who alive on the prevalence date.
The study population comprised of all adults (aged ≥18 years) who were residing in the region of Emilia-Romagna on 31 December 2012. Emilia-Romagna is a Northern Italian region with ∼4.4 million inhabitants, of which almost one-fourth are aged ≥65 years and >10% are foreign citizens—one of the highest proportion among all Italian regions.
In Italy, all residents are registered with the National Health Service that provides uniform and comprehensive care. Under the Italian Constitution and its recent modification (2001), the State has exclusive power to set the ‘essential levels of care’ for all residents throughout the country, whereas the regions have responsibility for the organisation and administration of publicly financed healthcare. Primary healthcare is provided by general practitioners remunerated on a capitation base/formula; they are in charge of providing care and assess patients' needs, order diagnostic procedures, prescribe drugs and refer patients to specialists and hospitals. They thus act as ‘gatekeepers’ for the system and ensure continuity of care to patients with chronic diseases.
Foreign citizens with regular stay permit are entitled to registration with the Italian National Health Service and to the same treatment as Italian citizens with reference to contributory burden and healthcare provided. Irregular immigrants, that is, without stay permit, can be assisted as ‘temporarily present foreigners’: they are provided a special card that ensures basic and specialised health services. Doctors in emergency services are not asked to report migrants who have no residence permit (law 94/2009 ‘Norms on public security’). In Emilia-Romagna, hospitalisation is lower among immigrants than among Italians, for men and women, when excluding obstetric causes. Even if hospital admissions of immigrants increased from 3.1% of total in 2002 to 7.4% in 2009, the number continues to be lower compared with hospital admissions of residents. However, immigrants tend to have more frequently urgent hospitalisations, probably due to limited knowledge of community health services and general practitioners.14
Definition of multimorbidity
No standard approach for the measurements of multimorbidity exists, and selection and definition of the diseases to be considered is inevitably subjective and dependent on the data available.2 In the present study, we sought to identify all diseases recommended as core for any multimorbidity measure in a systematic review,15 and which are likely to have a significant impact on patients in terms of need for chronic treatment, reduced function, reduced quality of life and risk of future morbidity and mortality. However, in Italy, electronic clinical records for primary care are not available because general practitioners are not requested to collect information about diseases. Thus, we tracked the presence of a number of diseases using information on hospital discharges, contacts with community mental health services and accredited residential facilities, and drug prescriptions.
Specifically, 16 physical illnesses were defined using the comorbidity ICD-9-CM coding algorithms developed by Charlson et al16 and Elixhauser et al,17 and enhanced by Quan et al,18 whereas 10 mental health disorders were tracked using an ad hoc ICD-9-CM coding algorithm.19 We also used drug prescriptions for tracking hypertension, diabetes, bipolar disorder, depression and anxiety—all diseases that, in Italy, are managed to a large extent by general practitioners. Table 1 provides further details of definitions and the 26 diseases included in the study. Complete lists of ICD-9-CM codes and ATC codes used for defining the 26 diseases are provided in online supplementary files 1 and 2, respectively. In online supplementary file 3, we have displayed the percentage contribution of hospitalisations and drug prescriptions in defining hypertension, diabetes, bipolar disorder, depression and anxiety.
List of the 26 diseases included in multimorbidity count
supplementary file
supplementary file
supplementary file
As in most other studies,15 we defined multimorbidity as the co-occurrence of two or more diseases in one patient.
Statistical analyses
We used graphical displays for descriptive analysis of differences in the prevalence of morbidity and multimorbidity across age groups and between women and men. Age- and gender-standardised prevalence of multimorbidity among foreign citizens was calculated using the Italian population resident in the region of Emilia-Romagna on 31 December 2012 as the standard population. Differences across age-groups, between women and men and between Italians and foreigners were assessed using the χ² test.
The correlations of the 26 conditions were analysed using exploratory factor analysis, as suggested by Schäfer et al,20 and using the iterated principal factor method. We used a tetrachoric correlation matrix for factor analysis: in doing so, we made the assumption that all the dichotomous diagnoses (presence or absence of the disease) reflected an underlying continuous latent trait, that is, that the chronic conditions included in the multimorbidity count had a progressive course and got diagnosed if a certain threshold was reached during this course. The factors resulting from this analysis can be interpreted as multimorbidity patterns (ie, clusters of diagnoses frequently associated with each other), and each factor loading represents the association of the specific disease with a pattern. As a measure of model fit, we reported the proportion of variance of the data accounted for by the multimorbidity patterns. The extraction criterion for factors was a minimum eigenvalue of 1. Factor loadings of 0.30 or more were considered relevant and reported in the results. Since we assumed that multimorbidity factors were associated with each other, we used an oblique (oblimin) rotation of factor loading matrices. Spearman's ρ was used to analyse the relationship of factor scores with age, gender and citizenship.
All analyses were conducted using Stata software, V.13 (StataCorp, 2013, Stata Statistical Software: Release 13, College Station, Texas, USA: StataCorp LP).
Ethics statement
The study was exempt from approval from the Ethics Committee of Emilia-Romagna. It was conducted in conformity with the regulations for data management from the Regional Health Authority of Emilia-Romagna, and with the Italian Code of conduct and professional practice applying to processing of personal data for statistical and scientific purposes (art. 20–21, legislative decree 196/2003; http://www.garanteprivacy.it/web/guest/home/docweb/-/docweb-display/docweb/1115480) published in the Official Journal no. 190 of August 14, 2004, which explicitly exempts the need for approval from the Ethics Committee when using anonymous data (Preamble number 8).
In Italy, anonymous administrative data-gathering is subject to the law Protection of individuals and other subjects with regard to the processing of personal data, ACT no. 675 of 31.12.1996 (amended by Legislative Decree no. 123 of 09.05.1997, no. 255 of 28.07.1997, no. 135 of 08.05.1998, no. 171 of 13.05.1998, no. 389 of 6.11.1998, no. 51 of 26.02.1999, no. 135 of 11.05.1999, no. 281 of 30.07.1999, no. 282 of 30.07.1999 and no. 467 of 28.12.2001) (http://www.privacy.it/legge675encoord.html).
Data were anonymised prior to the analysis at the regional statistical office, and each patient was assigned a unique identifier that eliminates the ability to trace the patient's identity or other sensitive data. As anonymised administrative data are used routinely for healthcare management, no specific written informed consent was needed to use the patient information.
All procedures performed in this study were in accordance with the 1964 Helsinki Declaration and its later amendments.
Results
We analysed data from 3 759 836 adults residing in the region of Emilia-Romagna on 31 December 2012 (women: 1 956 857, 52.0%; aged ≥65 years: 1 018 053, 27.1%; immigrants: 422 834, 11.2%). A total of 2 386 799 participants (63.5%) had no disease, whereas 798 829 (21.2%) had one disease and 574 208 (15.3%) two or more diseases. The demographic characteristics of the study population (ie, patients with one or more diseases) are provided in table 2. The mean number of diseases by age, gender and citizenship is also reported.
Demographic characteristics of the study population
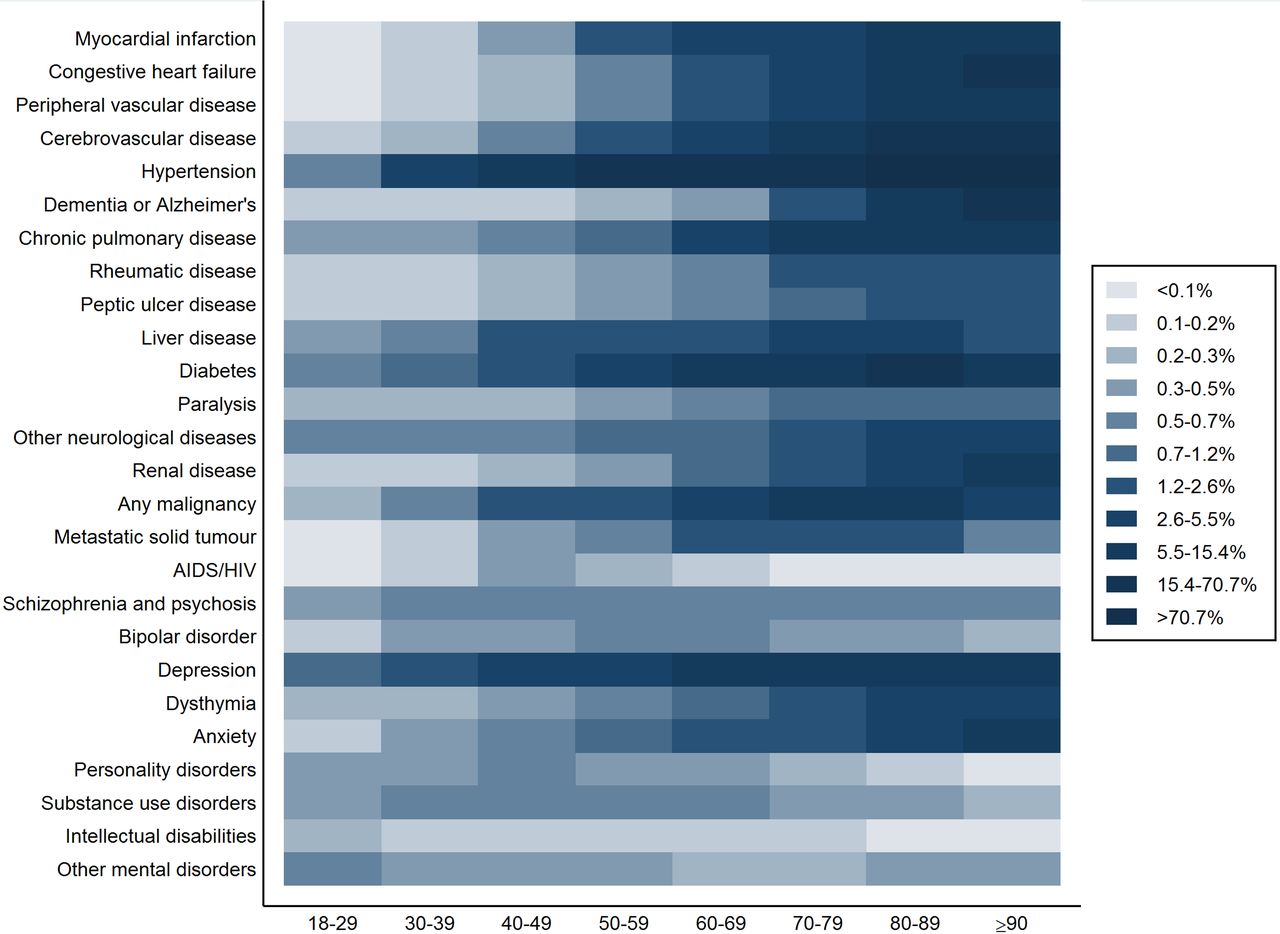
Figure 1 shows the prevalence of each disease by gender. The prevalence of hypertension (men: 27.8%, women: 31.1%; χ²=4700, p<0.001), depression (2.6%, 5.9%; χ²=25 000, p<0.001), anxiety (0.8, 1.5%; χ²=3800, p<0.001), dementia (0.8%, 1.4%; χ²=3500, p<0.001) and dysthymia (0.5%, 1.2%; χ²=5900, p<0.001) was higher among women, whereas diabetes (6.6%, 5.4%; χ²=2200, p<0.001), chronic pulmonary disease (2.8%, 2.1%; χ²=1800, p<0.001), myocardial infarction (2.4%, 1.0%; χ²=12 000, p<0.001), peripheral vascular disease (1.9%, 0.9%; χ²=7700, p<0.001) and renal disease (1.1%, 0.7%; χ²=1800, p<0.001) were more common among men. Figure 2 shows the prevalence of the 26 diseases by age group—dark blocks represent high prevalence values, whereas light blocks represent low prevalence values. The prevalence of all diseases increased with age, with the exception of AIDS/HIV and some psychiatric disorders (schizophrenia and psychosis, bipolar disorder, personality disorders, substance use disorders and intellectual disabilities and other mental disorders).

Prevalence values (%) of single diseases by gender.

Prevalence values (%) of single diseases by age group. Notes: Dark blocks represent high prevalence values, whereas light blocks represent low prevalence values. Cut-points of percentiles are displayed in the legend.
On 31 December 2012, in Emilia-Romagna, patients with a single disease were 798 829 (21.2%), whereas patients with multimorbidity were 574 208 (15.3%). The prevalence of morbidity differed significantly by gender (men: 19.4%, women: 22.9%; χ²=25 000, p<0.001), as well as the prevalence of multimorbidity (men: 15.1%, women: 15.4%; χ²=85.38, p<0.001). However, in this latter case, the significance of the test seemed to be caused by the large size of the study population, rather than by the actual difference between the two prevalence values.
The proportion of people with multimorbidity increased significantly with age (figure 3), from 19.1% in those aged 60–64 years up to 60.8% in the ≥90-year group (χ² for trend=700 000, p<0.001); among old patients (aged ≥65 years), the proportion of multimorbidity was 39.9%. Italian citizens with a single disease were 19.9% and those with multimorbidity were 14.4%, whereas among immigrants these prevalence values, standardised by gender and age, were significantly lower (15.0% and 9.3%, respectively, χ²=8200, p<0.001).

{kind=link}
{kind=link}
{kind=link}
Number of chronic diseases by age group. Notes: Red dots indicate the prevalence of multimorbidity by age group.
Exploratory factor analysis of diseases identified five patterns (table 3). The first factor includes psychiatric disorders; the second factor includes cardiovascular, renal, pulmonary and cerebrovascular diseases; the third factor comprises neurological diseases; the fourth factor includes liver diseases, AIDS/HIV and substance abuse; the fifth factor includes tumours. As for the association between factor scores and demographic characteristics, we found that the only correlation coefficient close to 0.30 was that between multimorbidity pattern 2 and age (Spearman's ρ=0.27, p<0.001), indicating that the presence of cardiovascular, renal, pulmonary and/or cerebrovascular diseases was more common among older than younger age groups.
Multimorbidity patterns derived from factor analysis
Discussion
In this population-based cross-sectional study, one of the six adults were multimorbid, whereas among older people (aged ≥65 years) this proportion was more than one of three. This result is consistent with the range of prevalence values found in other studies on multimorbidity,21–23 although very close to the lower boundary of this range (12.9% for participants aged ≥18 years). A possible explanation is that administrative databases contain only information about people seeking treatment in public services and accredited facilities. Therefore, a prevalence of 15.3% only reflects attended morbidity. Another reason for this results is the lack of a more comprehensive selection of diagnoses, including other relevant conditions mentioned in systematic reviews. It is also worth noting that, in line with other studies,24–26 the proportions of men and women presenting more than one chronic disease were very similar.
The Italian National Institute of Statistics (Istat) reported that, in 2012, multimorbidity affected 20.4% of the Italian population (49.4% in participants aged 54–74 years and 69.4% in participants aged ≥90 years) (http://www.istat.it/it/archivio/5471). These figures differ from those presented in this study for two possible reasons: first, Istat included in multimorbidity count some chronic diseases that we did not detect (ie, celiac disease, allergies, migraine and osteoporosis); second, the Istat survey is based on self-reported information, thus possibly overestimating the prevalence of some chronic health diseases.
When we examined each disease separately we found, consistently with other studies, that hypertension, diabetes and depression were highly prevalent,27 ,28 with some variation between genders (ie, hypertension and depression more common among women, and diabetes more common among men). In general, we found a high prevalence of hypertension, diabetes, depression, cerebrovascular disease, non-metastatic tumours, chronic pulmonary disease, congestive heart failure and myocardial infarction—all diseases that, according to the literature, should be included in every multimorbidity index.15 ,29
As expected, we found that multimorbidity was strongly associated with increasing age. This finding corroborates many other studies2 ,3 ,30 ,31 and may be explained by the longer exposure and increased vulnerability in older persons to risk factors for chronic health problems.3 Age-related multimorbidity has major financial and social implications, as populations are rapidly ageing in most countries, including developing countries and those in transition. Indeed, the burden of chronic disease is the biggest financial challenge to countries and healthcare systems worldwide.32
Of interest, immigrants had fewer diseases than Italian citizens. A possible explanation is that immigrants, presumably of first generation and looking for manual jobs that require intense physical work, are on average healthier than native-born. This phenomenon has been defined as the ‘healthy immigrant effect’.33 ,34 However, it is more plausible that these figures reflect the well-known lower access of immigrants to healthcare and particularly specialist healthcare.35
Using factor analysis, we identified some relevant disease patterns. Comparing our results with those of other studies is difficult because of different diseases, data sources, populations and setting considered. Still, like Islam et al,28 we found the tumours constitute a distinct pattern, probably because risk factors for cancer may be specific. Moreover, similarly to many other studies,21 ,26 ,27 ,36 ,37 we found a strong association between cardiovascular, renal, pulmonary and cerebrovascular diseases, suggesting that this pattern is part of the natural biological and pathological course of these illnesses, such as inflammation, hypoxia, oxidative stress or ageing, and is related to general risk factors such as smoking or pollution.38 In line with Barnett et al,2 we also found that psychiatric disorders tended to correlate with each other and were not associated with age. Finally, we found a multimorbidity pattern composed of liver diseases (ie, chronic hepatitis and cirrhosis), AIDS/HIV and substance use, which is consistent with evidence that liver and infective diseases are common in patients with substance use disorder.
Our results provide useful insights as regards the implementation of healthcare policies and the organisation of healthcare services. Although the evidence base for the management of multimorbidity appears to be thin and much more research is still needed,8 it is now well recognised that best practice should focus on the prevention of common risk factors and an orientation of treatment towards the improvement of functional limitations.21 These are core functions of primary care professionals, and particularly of generals practitioners, who are asked to have a broad knowledge base, be able to coordinate care across a range of different specialist services, have good judgement to balance competing priorities, inquire about patient preferences during a consultation and, as a whole, refine the treatment to multimorbid patients to promote better and more consistent management and self-management of the illnesses.6 ,9 ,39 Therefore, the high prevalence of multimorbidity in older patients underscores the urgent need for providing these care interventions on a routine delivery system.
The identification of clustering of conditions in patients with multimorbidity is no less important for three main reasons:21 from an aetiological perspective, to understand what makes conditions tend to co-occur with the aim to prevent their development in the first place; from a clinical perspective, to identify therapeutic approaches that allow the tailoring of care for significant strata of people with a given condition or combination of conditions and from a policy perspective, to target more common disease combinations and orient the delivery of care with the aim to ensure that the resources match the needs of patients of the same cluster.
The implications of our study need to be interpreted in light of the study's limitations. First, the use of administrative data may have underestimated multimorbidity. In fact, during the observation period, a number of participants suffering from chronic diseases (in particular psychiatric disorders) may have never sought care, been hospitalised or been prescribed long-term drug therapies. Moreover, the underestimation of multimorbidity may have been differential, that is, more pronounced for some patients rather than others (presumably older people and immigrants). However, in order to improve the accuracy of our estimates, we extended the observation period to several years and integrated different data sources, including hospital records and prescriptions, as suggested by other authors.40 ,41 Second, we did not use antipsychotic prescriptions to identify patients with dementia because these drugs are quite non-specific in their effect and are commonly prescribed also for a large number of severe psychiatric disorders, including schizophrenia, mania, agitated psychotic depression and paranoid disorders. Third, hypertension and depression were traced using some drugs that are prescribed also for heart failure, ischaemic heart disease and neuropathic pain, thus increasing the sensitivity of the disease count but lowering the specificity. Fourth, it is possible that a study period of 10 years, from 2003 to 2012, was not long enough to detect thoroughly all chronic diseases, especially for the elderly, once again possibly underestimating the number of morbid and multimorbid patients; an excessively long observation period, however, may lead to the inclusion of conditions with a prolonged course but which are not active at the time of the study.23 It is also worth noting that our study included the periods preceding and following the global financial crisis, and this may have overestimated the prevalence of some diseases which we investigated only in the post-crisis period such as depression and anxiety; for the same reason, estimates may have been inflated to some degree for younger people. Fifth, we did not include in the multimorbidity count a number of relevant conditions mentioned in systematic reviews, such as osteoporosis, angina, arthritis, cardiac arrhythmia, thyroid disease, anaemia, dyslipidaemia and obesity. We are well aware that this issue leads to an underestimation of multimorbidity and makes comparison with other studies difficult; still, our choice was conditioned by the fact that these diseases are not present in the algorithms developed by Charlson and Elixhauser, are managed to a large extent by general practitioners and are characterised by differences and variety in the case definition. For all these reasons, the multimorbidity prevalence estimates calculated in this study should be interpreted as the ‘lower boundary’ for the proportion of participants suffering from two or more chronic health disorders; to summarise, in Emilia-Romagna, the prevalence of multimorbid adults is not lower than 15% (40% among the elderly).
Conclusions
We found that multimorbidity was highly prevalent in Emilia-Romagna and strongly associated with age. We also found five predominant combinations of chronic conditions, suggesting that single disease-oriented clinical guidelines and pathways of care may be less effective than patient-centred care. These findings highlight the importance of planning studies that evaluate the impact of multimorbidity on health outcomes, costs and quality of care, and confirm the need for healthcare providers to promote access to healthcare, adopt individualised care plans and ensure continuity of care for patients who suffer from multiple chronic conditions.
Acknowledgments
The authors thank Eleonora Verdini, Luca Cisbani, Stefano Sforza and Mila Ferri, from the Emilia-Romagna region, for providing data. The authors thank Elisabetta Poluzzi from the University of Bologna for her assistance in the development of the algorithm for the identification of mental health disorders and Stewart Mercer from the University of Glasgow for his assistance in writing the paper.
References
Footnotes
Contributors JL and MPF made substantial contributions to the conception and design, analysis and interpretation of data, drafted the article and revised it critically for important intellectual content, and approved final version to be published. VMA, PR and MPF were responsible for interpretation of data, drafted the article and revised it critically for important intellectual content, and approved the final version to be published. GP was involved in conception and design, revised the article critically for important intellectual content, and approved the final version to be published. MPF is a guarantor for the study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Statistical code and raw data are available by emailing mariapia.fantini@unibo.it.