Article Text

Abstract
Introduction The frail elderly in Canada face a tough decision when they start to lose autonomy: whether to stay at home or move to another location. This study seeks to scale up and evaluate the implementation of shared decision-making (SDM) in interprofessional (IP) home care teams caring for elderly clients or their caregivers facing a decision about staying at home or moving elsewhere.
Methods A stepped wedge cluster randomised trial involving 8 Health and Social Service Centers (HSSCs) will be conducted with IP home care teams. HSSCs are the unit of randomisation. A decision guide will be passively distributed to all of the participating HSSCs at the beginning of the project. The participating HSSCs will then be randomised to 1 of 4 intervention start times, separated by 7-month intervals. The primary outcome is whether or not clients and caregivers assumed an active role in decision-making, assessed with a modified version of the Control Preferences Scale. The intervention, targeted at IP home care teams, consists of a 1.5 hour online tutorial and a 3.5 hour skills building workshop in IP SDM. Clients will be eligible for outcome assessment if they (1) are aged ≥65; (2) are receiving care from the IP home care team of the enrolled HSSCs; (3) have made a decision about whether to stay at home or move to another location during the recruitment periods; (4) are able to read, understand and write French or English; (5) can give informed consent. If clients are not able to provide informed consent, their primary caregiver will become the eligible participant.
Ethics and dissemination Ethics committee review approval has been obtained from the Multicenter Ethics Committee of CISSS-Laval. Results will be disseminated at conferences, on websites of team members and in peer-reviewed and professional journals intended for policymakers and managers.
Trial registration number NCT02592525, Pre-results.
- Frail elderly
- Home care services
- Shared decision making
- Interprofessional collaboration
- Knowledge translation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Frail elderly
- Home care services
- Shared decision making
- Interprofessional collaboration
- Knowledge translation
Strengths and limitations of this study
This trial addresses a difficult decision for the elderly: whether to stay home or move to another location. This decision is frequently encountered by home care teams.
By the end of this trial, all enrolled clusters will have been exposed to the intervention.
The novel stepped wedge design reconciles the need for robust evaluations with political or logistical constraints.
Recruiting elders and busy providers may be challenging.
It may be challenging for enrolled clusters to follow the randomisation schedule strictly.
Introduction
In the context of home care in Canada, one of the important decisions the frail elderly must face is whether to remain at home (with or without assistance) or move to another location.1 The care setting has a direct association with a wide array of outcomes impacting negatively on health, notably depression, pain, pressure ulcers and falls.1 In other words, where elderly people live is an important determinant of health.2 As older persons with better self-perceived health have lower mortality,3 ,4 feelings of control over healthcare decisions ought to play a part in the decision about where they live. Often, this decision is poorly or insufficiently planned with clients and caregivers receiving little or no decision support.5 Involving frail elderly clients and caregivers in this decision presents particular challenges as it is often associated with emotional turmoil.6–9 Shared decision-making (SDM) tools, such as patient decision aids, increase the involvement of patients in decisions about their care10 and can improve agreement between patients and their healthcare professionals.11 However, little is known about the most effective strategy to promote the use of decision tools in clinical practice or, ultimately, how to scale up SDM across the health and social care system. An interprofessional (IP) approach to SDM is especially relevant to caring for the frail elderly, as chronic illness often means that several different kinds of healthcare providers are involved in their care. Intentional interaction as a team enables healthcare providers to collaboratively support clients in facing difficult decisions, meet their decisional needs and reach healthcare choices that are agreed on by the client, family members/caregivers and the IP team.12 ,13 However, multiple barriers to achieving SDM have been identified that are specifically associated with multidisciplinary care settings, such as lack of visibility, lack of trust in expertise of other disciplines and lack of communication between disciplines.14 Therefore, training home care teams in SDM using an IP approach that addresses these barriers should facilitate effective uptake of decision tools in clinical practice and ultimately, scale up the implementation of SDM across the health and social care system. The objective of this study is to evaluate the impact of a training programme in IP-SDM (interprofessional approach to SDM) on the proportion of clients and caregivers who report taking an active part in the decision-making process, compared with the passive dissemination of a decision guide. Passive dissemination of printed educational material may have a small beneficial effect on professional practice outcomes, but its effectiveness compared with that of printed educational material as part of a multifaceted intervention is uncertain.15 For this purpose, a cross-sectional stepped wedge cluster randomised trial (cRT) is proposed. The null hypothesis is that the addition of a training programme in IP-SDM to the passive dissemination of a decision guide will not increase the proportion of clients and caregivers reporting an active role in the decision-making process.
Methods and analysis
Study setting and design
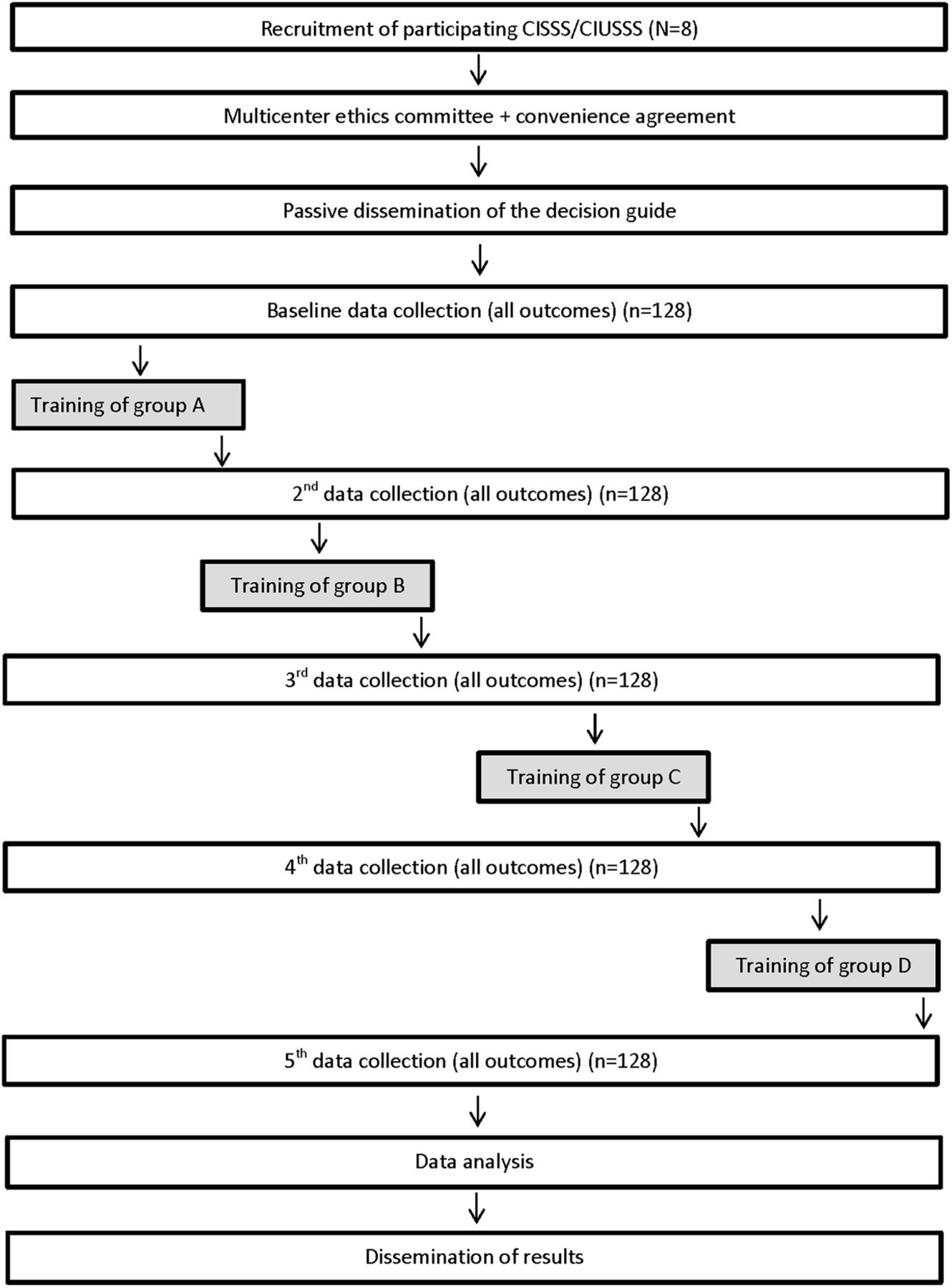
Stepped wedge cRTs are particularly well suited for evaluating interventions during implementation into routine practice and in situations in which there is a prior belief that the intervention (SDM training of IP home care teams) will do more good than harm, rather than a prior belief that there is equipoise (harms and benefits are equally balanced).16 This stepped wedge cRT will be conducted in the province of Quebec, Canada, with IP home care teams of eight Health and Social Services Centers (HSSCs), which are the units of randomisation. A decision guide will be passively distributed to all participating HSSCs at the beginning of the project. The HSSCs will then be randomised to one of four steps with a total of five data collection phases (figure 1). By the end of the study, all HSSCs will have received the intervention. Data will be collected on different (cross-sectional) samples of clients and caregivers at each data collection phase, but the same IP teams and providers will be involved throughout the trial.

Study flow diagram.
Eligibility criteria
All HSSCs of Quebec province, which are known in French as Centres intégrés de santé et de services sociaux (CISSS) or Centres intégrés universitaires de santé et de services sociaux (CIUSSS), will be eligible17 unless they have participated in an earlier cRT that compared the impact of training home care teams in SDM and provided them with a decision guide during training to usual care.18 We will contact the managers of the home care teams of all eligible HSSCs in random sequence to present the project and ask them about their interest in participating in the study. Clients of participating sites will be eligible for data collection if they: (1) are aged ≥65; (2) are receiving care from the IP home care team of the enrolled HSSC; (3) have made a decision about whether to stay at home or move to another location during the recruitment periods; (4) are able to read, understand and write French or English; (5) can give informed consent. In the case of clients who are not able to provide informed consent, their informal caregiver will become the eligible participant. Caregivers are defined in this study as close relatives or friends. Healthcare professionals of participating IP teams will also be recruited as participants.
Passive dissemination of the decision guide (control period)
At the beginning of the project, we will ask managers of all enrolled HSSCs to distribute a decision guide to their IP home care teams to be used with their clients and caregivers (passive dissemination). We will offer managers and healthcare professionals as many decision guides as they need, on request.
Intervention
All IP home care teams will receive the multifaceted intervention at different time points (figure 2). The intervention consists of (1) a 1.5 hour online tutorial, based on the Ottawa Decision Support Tutorial,19 ,20 and (2) a 3.5 hour skills building workshop which includes a lecture, a video demonstrating SDM in the context of an IP home care team and performance feedback during a role play.21 The online tutorial is completed individually. The intervention will be delivered at the sites allocated to the intervention step. The decision guide distributed before the intervention will still be available in sufficient quantities after the intervention.

{kind=link}
{kind=link}
Stepped wedge study design.
Allocation of participating sites to intervention groups
The unit of randomisation will be the HSSC responsible for the IP home care teams. Eight HSSCs will be randomised to one of four steps, representing different start times for the intervention, namely at 4 (T4), 11 (T11), 18 (T18) and 25 (T25) months after the start of the baseline data collection (T0) (figure 2). An independent biostatistician will perform randomisation using computer-generated numbers. Allocation will be concealed from investigators involved in the study. The biostatistician performing the allocation will not be involved in data analysis.
Proposed frequency and duration of follow-up
There will be a total of five data collection periods with 1 month for the intervention between each of them at T4, T11, T18 and T22 (figure 2). Thus, the total duration of data collection will be 32 months. Every 7 months, the intervention will ‘step up’ to the next group of HSSCs, while the previous groups continue to apply their newly acquired skills, until all four groups have received the intervention (figure 2). As outcome assessments of the trial can only take place once the decision guide is available for use, the decision guide will be passively disseminated to each cluster 3 weeks before the baseline data collection.
Recruitment and loss to follow-up
We will assign trained research assistants (RAs) to each participating site for data collection. The HSSC will be responsible for identifying and contacting eligible clients and caregivers and asking permission for the RA to contact them. Their agreement will indicate their interest in participating in the project. Then, the RA will meet interested participants at their home, complete informed consent and proceed with data collection. Healthcare professionals of the IP home care teams will provide informed consent prior to the training session. To facilitate engagement, the research study budget will cover all fees the HSSC may incur in relation to the project. Owing to the nature of this study, which entails no follow-up of participants for the main outcome (only one data collection point for each participant), we expect no loss to follow-up at the clients and caregivers levels.
Outcomes and measures
The primary outcome will be the role assumed in decision-making by clients and caregivers regarding whether the clients have to stay at home or move to another location. To assess the proportion of clients and caregivers reporting an active role, we will use the modified version of the Control Preferences Scale22 designed to assess the role assumed in the decision-making process.23 This single-question scale is most frequently used in studies assessing the implementation of SDM in clinical practice.24 Response options are: (A) I made the decision; (B) I made the decision after seriously considering my providers' opinion; (C) My providers and I shared the responsibility for making the decision; (D) My providers made the decision after seriously considering my opinion; (E) My providers made the decision. A and B represent a client or caregiver-controlled decision-making process, C represents an SDM process, and D and E represent a provider-controlled decision-making process.23 For the primary outcome, we will collapse these five categories into just two: A, B and C will represent an active role in the decision-making process and D and E will represent a passive role. The modified version of the Control Preferences Scale is used to reduce the burden on frail elderly participants, as suggested by our stakeholders.
Secondary outcomes assessed in caregivers and clients will be (1) their involvement in decision-making, assessed with the D-OPTION scale, a 12-item instrument that assesses 12 specific SDM behaviours during decision-making;25 ,26 (2) preferred and chosen option (remain at home or move to another location); (3) decisional conflict, assessed with the 16-item Decisional Conflict Scale;27 ,28 (4) decision regret, assessed with the 5-item Decision Regret Scale;29 (5) uptake of the decision guide, assessed by showing an image of the decision guide and asking the question ‘Were you shown this decision guide?’; (6) health-related quality of life (only in client), assessed with two subscales (social isolation and emotional reactions) from the Nottingham Health Profile;30–33 and (7) burden of care (only in caregivers), assessed with the Zarit Burden Inventory scale (ZBI).34–36 Healthcare professionals' behavioural intention to engage into SDM will be measured before and after the intervention with a 12-item theory-based instrument assessing the impact of continuing professional development.37 Tutorial and workshop also include an evaluation component. In addition, we will collect qualitative data on the research process by the use of RAs' logbooks in which participants' comments and reactions will be recorded. We will also periodically contact site managers and research agents to solicit their views on the research process.
Protection against sources of bias and data management
Given the sequential nature of this trial, the investigators and project coordinator will know which HSSCs are receiving the intervention and therefore will not be blinded to group allocation. However, the allocation list will be concealed from the research team for as long as possible; when the next HSSCs group needs to schedule the intervention, only those randomised in that step will be revealed. Also, to minimise sources of bias: (1) we will respect strict concealment of allocation; (2) we will ensure that data collection forms and packages look the same for all groups and data collection periods; (3) two independent data clerks will use a secret group code to perform double data entry; (4) the biostatistician, who will not be involved with randomisation, will be blinded for data analysis as the database will not identify the names of the HSSCs; (5) RAs who collect data from clients and caregivers will be blinded to the allocation status of the HSSC and will be asked not to discuss this information with any participants; they will moreover meet clients and caregivers at their homes or talk to them on the phone); (6) the information given to participants will be the same in the control and intervention periods, and will not refer to the intervention; and (7) analysis will be by intention-to-treat. Questionnaires will be verified by the project coordinator immediately after completion to minimise missing data. Recruitment of clients will be sequential and will be the responsibility of the research team. As HSSC-based home care teams do not share clients and are geographically separated, we do not expect any contamination of the intervention among providers in participating HSSCs. We will emphasise to participants the importance of not sharing the information and material provided with their colleagues from other HSSCs.
Statistical analysis
Sample size
The primary outcome is the proportion of clients and caregivers who report an active role in the decision-making process. The sample size estimate is informed by preliminary data from another study titled DOLCE.18 We used the method developed by Hussey and Hughes for stepped wedge designs.38 ,39 We assumed an average of eight clients and eight caregivers per HSSC in each 6-month data collection period and an ICC of 0.05.40–44 To detect an absolute improvement of 20% in the primary outcome (from 70% to 90%) with 80% power using a stepped wedge design with four steps and a two-sided test at the 5% significance level, a total of eight clusters is required (ie, a total of 320 clients and 320 caregivers).
Analysis plan
We will calculate descriptive statistics of organisational (HSSC) and sociodemographic characteristics for clients, caregivers and healthcare providers. All primary and secondary outcomes will be analysed using the approach described by Hussey and Hughes,38 using the ‘intention-to-treat’ principle. The unit of analysis will be the client (or caregiver). Dichotomous outcomes will be analysed using multilevel logistic regression analysis, while continuous outcomes will be analysed using multilevel linear regression analysis. Time will be modelled as a fixed categorical variable, while the HSSC will be modelled as a random effect to account for the intracluster correlation.38 For each outcome analysed, goodness of fit will be assessed and the validity of the underlying assumptions of the model will be checked. All analyses will be conducted using SAS statistical software V.9.4 (SAS Institute, Cary, North Carolina, USA).
Data monitoring
The main co-PIs (FL, DS and NB) and the project coordinator (GPG) will form a monitoring committee which will provide regular guidance throughout the project (meetings once per month). A trial steering committee made up of co-PIs (FL, DS, NB), co-Is (GL, SDe, SDu, KDF, L-PR and PJD), the project coordinator (GPG) and two caregivers representatives (LR, HB) will also provide regular expert feedback for project monitoring (meetings once every 4 months).
Discussion
This trial will address challenges and knowledge gaps in the implementation of SDM. There is a growing number of ageing Canadians who are facing the decision regarding location of care and who need client-centred decision support. Hence, there is an urgent need to improve the decision-making process via training of IP home care teams in SDM, as it is not implemented yet in clinical practice.45 Therefore, in this study, we seek to scale up the implementation of an (SDM) intervention to IP home care teams in eight HSSCs working with hundreds of clients and caregivers facing decisions about the location of care, and to evaluate the impact of this intervention on the uptake of SDM as indicated by the role assumed by clients and caregivers in the decision-making process. Our results will also enhance the knowledge base about effective interventions for scaling up evidence-based practice across multiple clinical settings by increasing knowledge in the following high-priority research areas: (1) designing health services and supportive policies that meet the health needs of older adults; (2) evaluating innovative and integrated models of primary and community care; (3) empowering patients/self-management/patient experience; (4) supporting caregivers; (5) scaling up evidence-based innovation and (6) advancing decision support and population health monitoring.
Dissemination
This trial is registered at clinicaltrials.gov (NCT02592525). All participants (clients, caregivers and healthcare professionals) will sign consent forms approved by the ethics boards of their respective institutions. All authors will contribute to the dissemination of study results, including caregiver representatives on the trial steering committee. We will tailor effective knowledge translation strategies for each targeted user group (eg, policymakers, clinicians, healthcare organisation managers, seniors' associations). We will disseminate study results: (1) at conferences (scientific and professional) whose themes relate to SDM, IP and health policy; (2) on the websites of team members and (3) as articles in peer-reviewed journals and professional journals intended for policymakers and managers (eg, the Ministère de la Santé et des Services sociaux bulletin Coup d’œil). Furthermore, skills gained by home care teams in this study are likely to be transferable to support clients who are making other decisions, such as those related to mental health.
Trial status
Participant recruitment started on November 2015 and we anticipate it will be complete by June 2018.
Acknowledgments
FL is supported by a Tier 1 Canada Research Chair. DS is supported by a Research Chair at the University of Ottawa. SDe is supported by a New Investigator Salary Award from the Canadian Institutes of Health Research (CIHR). L-PR is supported by a Tier 1 Canada Research Chair GL is supported by the Industrial Alliance Research Chair on the Economics of Population Ageing.
References
Footnotes
Contributors FL, NB and DS conceived the study. GL provided guidance for the planned cost-effectiveness analyses. SDe, SDu and KDF provided guidance on the Interprofessional Shared Decision-making Model and the training workshop materials. L-PR, MT and ST provided guidance for the planned statistical analyses. PJD, HB and LR validated the relevance of the trial and provided guidance on the methods. GPG is coordinating the project. FL and GPG drafted the manuscript. All authors have read and approved the final version of the manuscript. FL is its guarantor.
Funding This research is funded by the Canadian Institutes of Health Research (Grant number: 201403MOP-325236-KTR-CFBA-19158), and also supported by the CIUSSS de la Capitale-Nationale (in kind contribution included in the CIHR grant).
Competing interests DS reports personal fees from Washington State Health Authority Patient Decision Aid certification programme, outside the submitted work.
Patient consent Obtained.
Ethics approval Centre intégré de santé et de services sociaux de Laval (CISSS de Laval).
Provenance and peer review Not commissioned; externally peer reviewed.