Article Text

Abstract
Introduction Positive health behaviours such as regular physical activity and a healthy diet have significant effects on cancer outcomes. There is a need for simple but effective behaviour change interventions with the potential to be implemented within the cancer care pathway. Habit-based advice encourages repetition of a behaviour in a consistent context so that the behaviour becomes increasingly automatic in response to a specific contextual cue. This approach therefore encourages long-term behaviour change and can be delivered through printed materials. ‘Healthy Habits for Life’ is a brief intervention based on habit theory, and incorporating printed materials plus a personally tailored discussion, that has been designed specifically for patients with a diagnosis of cancer. The aim of this trial was to test the effect of ‘Healthy Habits for Life’ on a composite health behaviour risk index (CHBRI) over 3 months in patients with a diagnosis of breast, colorectal or prostate cancer.
Method and analysis A 2-arm, individually randomised controlled trial in patients with breast, colorectal and prostate cancer. Patients will be recruited over 18 months from 7 National Health Service Trusts in London and Essex. Following baseline assessments and allocation to intervention or usual care, patients are followed up at 3 and 6 months. The primary outcome will be change in CHBRI at 3 months. Maintenance of any changes over 6 months, and changes in individual health behaviours (including dietary intake, physical activity, alcohol consumption and smoking status) will also be explored.
Ethics and dissemination Ethical approval was obtained through the National Research Ethics Service Committee South Central—Oxford B via the Integrated Research Application System (reference number 14/SC/1369). Results of this study will be disseminated through peer-reviewed publications and scientific presentations.
Trial registration number 17421871.
- CANCER
- SURVIVOR
- BEHAVIOUR CHANGE
- HABITS
- INTERVENTION
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This intervention is a novel approach to improving health behaviours of cancer survivors.
This intervention has potential to be delivered within the cancer care pathway without prohibitive cost.
Owing to the nature of the intervention it will not be possible to blind participants.
The majority of outcome measures are self-reported.
Introduction
Smoking, poor diet and low levels of physical activity are established risk factors for development of cancer, but there is now a growing body of evidence linking them with survival after diagnosis.1–7 The weight of scientific evidence has led to consensus statements regarding lifestyle change for cancer survivors.8–10 The most comprehensive of these recommendations are by the World Cancer Research Fund (WCRF) who recommend that cancer survivors should follow guidelines for cancer prevention.10 They include recommendations for diet, physical activity, alcohol consumption, tobacco and body weight.10 They are an important development for the field, although a recent study demonstrated that oncology health professionals' awareness of them is suboptimal.11 Previous research has also shown that the majority of cancer survivors are not meeting these recommendations,12 but would like advice post-treatment on how to make positive lifestyle changes.13 There is therefore a need to translate the recommendations into effective behaviour change advice that is appropriate for use with cancer survivors and can be disseminated cost-effectively through existing care pathways.
A number of studies carried out in the USA, Canada and Australia have demonstrated that lifestyle interventions for prostate, breast and colorectal cancer are not only acceptable to patients, but can successfully improve more than one health behaviour.14 ,15 These studies have demonstrated the effectiveness of tailored, mailed print materials (eg, two 5-month workbooks and newsletters),14 and of telephone delivered sessions combined with mailed materials (eg, 11 phone calls over 6 months combined with a participant handbook, regular motivational postcard prompts, a pedometer and a quarterly study newsletter).15 These results are promising, but to date there is a lack of behaviour change interventions in a UK healthcare setting. Furthermore, these approaches are fairly labour intensive. In order to benefit enough cancer survivors to have a significant public health impact, an intervention must be cost-effective and feasible to implement in the current clinical pathway. In other words, it needs to be both brief and inexpensive so that it can be delivered to all eligible patients by health professionals within the National Health Service (NHS), where time and resources tend to be limited.
A potential strategy, which combines elements from previous successful approaches but within a briefer format, is to use standard print materials containing guidelines and simple behavioural skills as the ‘first-line’ intervention, and combine this with a single individually tailored, brief, telephone discussion. This maximises coverage, takes advantage of patient preferences for print materials16 and simple advice17 and also capitalises on patients' desire to receive personalised advice, which is viewed as more relevant than generic communications.18 ,19 Furthermore, tailoring can enhance the effects of health-promoting messages, through stimulating greater cognitive activity than messages that are not tailored.20 A recent systematic review also demonstrated the effectiveness of the telephone for the delivery of lifestyle interventions to cancer survivors.21
Previous lifestyle interventions with cancer survivors have not had a consistent theoretical basis. For example, the study of mailed tailored materials14 drew on Social Cognitive Theory22 and the Transtheoretical Model,23 whereas the combination of telephone-delivered sessions and mailed materials15 was based on Acceptance Commitment Therapy.24 Studies within other patient populations suggest that an ideal theoretical basis for providing behaviour change advice in a brief format is the habit model.25 According to habit theory, the essential feature of habits is that they are ‘automatic’ (ie, require minimal willpower or deliberate effort), and therefore are well maintained.26 Psychological research shows that repetition of an action in a consistent context enables it to become automatic, and once automatic, it is more resistant to extinction than deliberative (intentional) actions; increasing the likelihood the action will become a habit and therefore continue over the longer term.27 There has therefore been increasing interest in the application of habit theory within the healthcare context.28
Providing individuals with advice on how to try and form habits for specific health behaviours (ie, by integrating simple actions into their existing routines, and associating the new action with a specific context, such as always taking a walk straight after lunch) is less time consuming to explain, and easier for patients to implement than traditional behaviour change strategies.28 There is growing evidence that brief habit-based interventions can encourage positive changes in dietary and physical activity behaviours for a range of populations, including older adults and patients with obesity.29 ,31 In particular, one recent study demonstrated the potential for combining printed materials on habit-based health behaviour change with a brief discussion with a health professional.25 However, this approach has not been tested with cancer survivors.
The proposed study therefore explores the impact of a behaviour change intervention that has been developed based on habit theory and which can be delivered via printed materials and a brief tailored discussion to all eligible patients with a diagnosis of breast, colorectal or prostate cancer. This is an individually randomised trial to evaluate behavioural outcomes. If successful, it will lead on to a future, large-scale, pragmatic randomised controlled trial (RCT) with cancer-relevant outcomes (biomarkers, physical function, adverse effects of treatment, survival) and a full cost-effectiveness analysis.
Aims
Primary research objective
To test the effects of an intervention incorporating tailored advice plus patient materials on a composite health behaviour risk index (CHBRI) over 3 months in patients with a diagnosis of breast, colorectal or prostate cancer, compared with the effects of ‘usual care’.
Secondary research objectives
The main secondary research objectives are to test for differences in individual health behaviours (physical activity, sedentary behaviour, diet, smoking and alcohol) and body mass index (BMI) over the trial period, and examine whether any changes in CHBRI observed at 3 months are maintained at 6 months. Improvements in fatigue, sleep and quality of life at 3 and 6 months will also be investigated as secondary outcomes. Compliance and satisfaction with the intervention, alongside basic costs, will also be recorded.
Methods and analyses
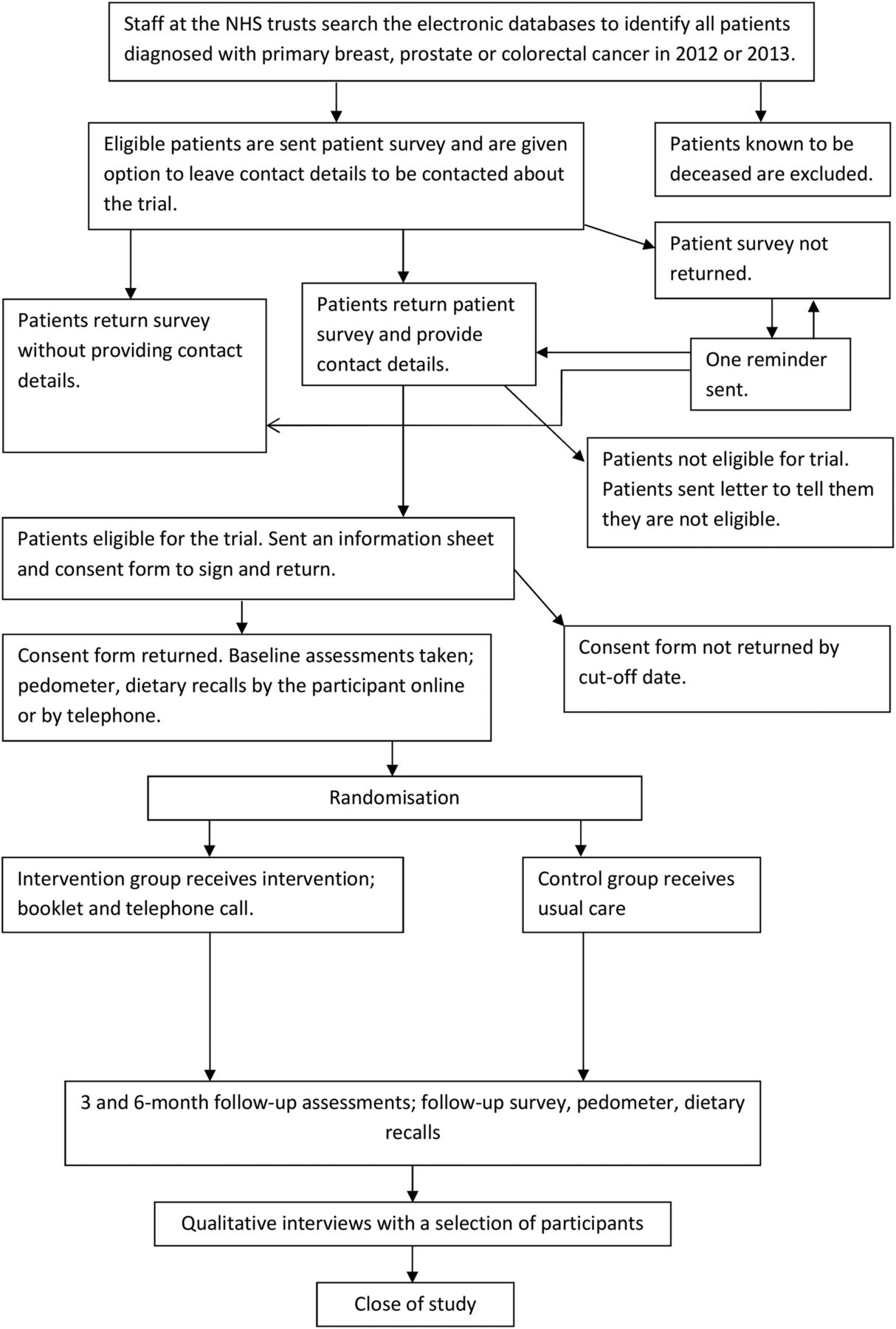
The trial will be a two-arm, individually randomised, parallel-group trial in patients with a diagnosis of breast, colorectal or prostate cancer, comparing the ‘Healthy Habits for Life’ intervention with ‘usual care’. Figure 1 illustrates the pathway through the trial.
{kind=link}
Flow chart of patient recruitment and involvement in study. NHS, National Health Service.
Participants
Patients who received a diagnosis of breast, colorectal or prostate cancer in 2012/2013 and who express an interest in taking part in a trial of a lifestyle programme from seven NHS Trusts across London and Essex.
Recruitment
NHS Trusts were recruited to take part in a cohort study to explore the health and lifestyle of patients with cancer postdiagnosis. NHS Trusts were initially recruited through London Cancer (five trusts) and two additional trusts were recruited following the posting of the study on the Clinical Research Network Portfolio. Participating sites mail a health and lifestyle questionnaire to all patients diagnosed with breast, colorectal and prostate cancer in 2012/2013. On the final page of the questionnaire, patients have the opportunity to express their interest in taking part in a trial of a lifestyle programme and to provide their contact details. Interested patients will be checked for eligibility based on their responses to the survey. Eligible patients will be mailed an information sheet and consent form (figure 1), and receive a reminder telephone call if this is not returned. The information sheet states that the study is concerned with promoting a healthy lifestyle among people who have been diagnosed with breast, prostate or colorectal cancer, and that we have developed a lifestyle programme (consisting of a lifestyle booklet, and telephone call) and are interested in finding out what patients think about it. No further details of the intervention will be given. Recruitment is expected to take place over 18 months to achieve the required sample size.
Inclusion criteria
The study will be restricted to adults (age ≥18) who are able to consent for themselves (presumed from completion of the consent form). Individuals who report a diagnosis of non-metastatic (stage I–III) breast, prostate or colorectal cancer or report that their cancer has not spread (as a proxy measure for stage), and who state they are no longer receiving active cancer treatment (with the exception of oral cancer treatments taken at home) will be included. If patients report that they do not know the stage of their disease or whether it has spread, this will be checked with the NHS Trust from which they were initially recruited. Similarly, any lack of clarity around receipt of treatment will be queried with the appropriate NHS Trust.
Exclusion criteria
Patients will be excluded if they (1) are unable to provide informed consent due to severe cognitive impairment, (2) have metastatic disease (stage IV, their cancer has spread) or (3) are receiving active cancer treatment requiring hospital admission. Although these groups may also benefit from lifestyle change, they are likely to require a different interventional approach with a higher level of input and supervision. There is not an upper age limit because previous studies have demonstrated that interested older patients are able to benefit and are important to include given the impact of cancer on functional decline.32
Randomisation
The unit of randomisation will be the patient, and the allocation ratio will be 1:1. Allocation will be determined based on minimisation using the software MinimPY (an open-source customisable minimisation program for allocation of patients to parallel groups in clinical trials)33 after the participant has provided informed consent and baseline data. Randomisation will be stratified by cancer type (breast, colorectal or prostate). The first participant will be randomly allocated, then each subsequent participant, will be allocated based on the imbalance scores (calculated as a function of current allocations after a hypothetical allocation of the new participant in each study arm). The new participant will be allocated to the arm with the lowest imbalance score.34 A 20% random element will be included in the algorithm.35
The researcher responsible for randomisation will inform the trial assistant and trial manager of treatment allocation using a password-protected spreadsheet. Once allocated, the trial assistant will inform participants of their allocation by mailing the intervention materials or making a brief phone call to those allocated to usual care stating that all of their data have been received, and they have not been allocated to receive the booklet.
The intervention
The ‘Healthy Habits for Life’ intervention consists of a self-guided printed booklet designed to help cancer survivors make healthy lifestyle behaviours habitual (see online supplementary material 1). The intervention was developed through an iterative process with input from patients, health professionals and experts in the field. A social marketing company designed the booklet, which includes a description of recommended health behaviours and their potential benefits based on the WCRF recommendations for cancer survivors.10 Specifically, it gives advice on nine target areas that participants might set goals around. These are: (1) being active every day for 30 min or more (and aiming for 10 000 steps a day), (2) getting stronger and fitter (doing strength, balance and stretching exercise twice per week and two 30 min sessions of vigorous exercise per week), (3) increasing fruit and veg (five portions or more a day, mostly vegetables), (4) maximising fibre (choosing wholegrain and adding fruit, vegetables and pulses to meals), (5) watching out for high calorie foods and drinks (reducing fat and sugar and cutting out sugary drinks), (6) reducing red meat (no more than 500 g across the week), (7) cutting out processed meat, (8) quitting smoking, and (9) cutting back on alcohol (no more than 2–3 units per day for women and 3–4 for men, with at least 2 days alcohol free). For each target behaviour, there is a list of new actions that could be incorporated into a daily routine to help participants meet their goals (ideas for everyday change).
Supplementary material 1
In addition to the description of the recommended health behaviours and their benefits, the booklet contains advice on forming healthy habits (eg, repeating the new actions in a similar context), in line with habit theory. Based on patient input, it also has quotes from health professionals endorsing the health behaviours, quotes from other cancer survivors encouraging participation, and links to resources (eg, NHS smoking cessation services). The booklet also uses evidence-based behaviour change techniques; goal setting, planning, self-monitoring and the use of rewards.36 ,37 ‘Healthy Life Action Plan’ sheets (see online supplementary material 2) encourage participants to set goals for the recommended behaviours, to plan how they will fit the new action into their existing routines, and to track their progress throughout the intervention (to support self-monitoring). Participants are also encouraged to reward themselves for progress made. During intervention development, some patients reported a desire for more information. Because of the need to keep the booklet brief, there is therefore a corresponding simple website with additional information on habit theory, the scientific evidence base behind the recommendations, suggestions for home exercise, a frequently asked questions section and sources of additional information and support.
Supplementary material 2
Participants in the intervention group will receive a telephone call from a researcher who will talk participants through the printed booklet, to check understanding, answer any questions and encourage engagement with the material. This call will take place ∼1 week after they have been sent the booklet. During the telephone call, the researcher will follow a guide (see online supplementary material 3), which includes talking through the recommendations, giving advice on forming healthy habits, discussing with the participant which health behaviours they are going to change, and giving instructions for using the ‘Healthy Life Action Plan’ sheets. Participants will be encouraged to start with between one and three behaviours, and then add other changes as and when they feel able to do so. Participants will be provided with feedback from their baseline data (including average step count and which recommendations they appear to be meeting), and encouraged to focus on behaviours which they could benefit most from changing.
Supplementary material 3
Researchers delivering the intervention will have a background in psychology and experience of talking to patients. They will receive brief (2 hours) training on delivering the intervention from senior psychologists and dietitians within the team, including practice going through the script, how to manage concerns, likely questions that may come up and problem solving. Quality control checks will be made, with the trainers observing each staff member delivering the intervention on at least one occasion. During these calls the trainers will complete a checklist on adherence to the guide, and provide feedback at the end of the call.
Usual care
Patients randomised to the control comparator will receive ‘usual care’. Previous research suggests that patients do not receive health behaviour advice unless they specifically ask for it,38 and this has been confirmed by clinicians involved in the trial. All participants will be asked at baseline about any other lifestyle programmes they are involved in, and at follow-up they will be asked about any changes to their health or treatment.
Measures
Demographics and health status
Demographic data including age, sex, education, employment status (current and precancer diagnosis), marital status and living arrangement (who they live with), and ethnicity will be taken from the initial health and lifestyle questionnaire (pretrial entry).
Within this questionnaire, patients are also asked what type of cancer they were diagnosed with in 2012 or 2013 (breast, prostate or colorectal; as the questionnaire is intended to be sent to these patients) and the date of their diagnosis. They are asked the stage of their cancer and if it has spread to any other part of their body. Two questions ask about cancer treatment including the type of treatment they had and the time since they completed their initial treatment for cancer. They are also asked if they have any other health problems.
The pretrial entry health and lifestyle questionnaire also includes self-report measures of health behaviours, anthropometrics and psychosocial variables identical to those used in the trial (see below). Where participants are added to the trial within 2 months of their initial questionnaire, these responses will be used as their baseline (prerandomisation) for the variables outlined below. In addition, participants will be sent a pedometer and invited to complete a dietary recall (further details below). When patients are added to the trial more than 2 months after their initial questionnaire, they will be sent a new baseline questionnaire containing the measures outlined below alongside their pedometer and dietary recall invite. All measures will be repeated at 3-month and 6-month follow-ups (see table 1). All follow-up data will be entered by researchers blind to treatment allocation.
Measurement of variables within Advancing Survivorship Cancer Outcomes Trial (ASCOT)
Health behaviours
Measurement of the following health behaviours will contribute to the calculation of the primary outcome (CHBRI—see Calculating the primary outcome section below). Individual health behaviours will be explored as secondary outcomes.
Physical activity will be assessed using an Omron pedometer, which provides a valid and reliable assessment of step count.39 Researchers will mail out the pedometer to participants alongside a pedometer log book that contains instructions on correct wear protocol. The step count reader on the pedometers will be covered so that participants will be unable to see their step count (as this may act as an intervention itself40). Participants will be asked to record in the log book the time the monitor is put on in the morning and taken off in the evening before sleep. Participants will also record in the logbook any significant non-wear time during the day, for example, removed to go swimming or forgot to put on. Participants will be asked to wear the pedometer on their waist/in their pocket for 6 consecutive days, and to then return immediately with the logbook in a provided freepost envelope. At follow-ups, participants will be instructed to wear the pedometer the same way that they wore it at baseline (ie, if they wore it on their waist at baseline, they should wear it on their waist at follow-up).
Additionally, participants will complete the Godin Leisure-Time Exercise Questionnaire.41 This measure has demonstrated favourable validity and reliability against objective activity monitoring and measures of fitness42 and has been widely used in the oncology research context.42 Sedentary behaviour will be assessed (but will not contribute to the CHRBI) using a single item on sitting behaviour taken from the International Physical Activity Questionnaire (IPAQ)43 and two items on TV viewing taken from the English Longitudinal Study of Ageing.44 ,45
Diet will be assessed using repeated multiple pass dietary recalls completed online by the participant or by telephone. This is a standard retrospective, dietary assessment used to capture information on all food and drinks consumed in the preceding 24 hours. It has been used in previous dietary intervention trials with cancer survivors32 ,46 ,47 and is recommended for measuring diet in this population.48 Participants will also complete a self-report questionnaire with items adapted from the Dietary Instrument for Nutrition Education (DINE).49 This measure was chosen based on a review of validated food frequency questionnaires and a review of dietary assessments used in studies with cancer survivors. The DINE is a brief measure (minimising participant burden), which was adapted to ensure that it captured a range of ethnically diverse foods and where possible, included all foods in the WCRF guidelines.10
A review of questions in the National Diet and Nutrition Survey (NDNS) and the Low Income Diet and Nutrition Survey (LIDNS) was also conducted to ensure that the main components of the UK diet were included. The adapted DINE will include 12 questions to assess dietary fibre (eg, ‘About how many times a week do you eat a serving of pasta, rice, noodles or couscous?’ with response options: less than once a week or never/1–2 per week/3–5 per week/6 or more per week), and 19 questions to assess total fat (eg, ‘About how many times a week do you eat a serving of cheese (any except cottage cheese)?’ with response options: less than once a week or never/1–2 per week/3–5 per week/6 or more per week). Two further questions will assess sugar intake. The first measures the consumption of sugar-sweetened beverages (‘How often do you drink regular (ie, non-sugar-free) squash, cordials, fizzy drinks and juice drinks?’ with response options never or rarely/once a week/2–3 times a week/4–6 times a week/once a day/twice a day/3 or more times a day).50 The second question asks about added sugar (About how many rounded teaspoons of sugar, honey or syrup do you usually use in a day (eg, in coffee, tea, milk, bread, cereals, fruit)?). This is an open question where patients are asked to write the total number of teaspoons per day. This question was adapted from the National Health and Nutrition Examination Survey (NHANES) Dietary Screener Questionnaire.51 Fruit and vegetable intake will be assessed using a two-item dietary questionnaire.52 ,53 This measure has been shown to have sufficient validity when compared with objective biological measures of fruit and vegetable consumption.53
Tobacco usage will be assessed using a question adapted from those used in the Health Survey for England.54 Patients will be asked ‘Do you smoke/chew tobacco at all nowadays?’ (yes/no). This question was adapted to include tobacco chewing in order to align it with the WCRF guidelines.10
Alcohol will be assessed using an adapted version of the Alcohol Use Disorders Identification Test Consumption Questions (AUDIT-C), a three-item screening test for active alcohol abuse or dependence and/or heavy drinking.55 This measure has been found to perform better than the full length AUDIT questionnaire at identifying heavy drinkers who may benefit from brief primary care interventions. For this study, the questions on frequency (‘How often do you have a drink containing alcohol?’ with response options: never/monthly or less/2–4 times per month/2–3 times per week/4+ times per week) and quantity (‘How many units of alcohol do you drink on a typical day when you are drinking?’ with response options: 1–2/3–4/5–6/7–9/10+) will be used to calculate the number of alcoholic drinks consumed per day. The frequency question was adapted to include the option ‘every day’ for the purpose of calculating who was meeting the WCRF recommendations.10
Anthropometrics
At baseline, participants will be asked to report their height and weight (preferably weighing and measuring themselves that day). At 3-month and 6-month follow-ups, participants will be asked to record their weight again. This will allow for BMI to be calculated at each time point as a secondary outcome using the standard formula of weight (kg)/height (m)2.
Psychosocial measures
Psychosocial measures will be included as secondary outcomes to assess the broader impact of the intervention for patients in terms of its effects on their well-being. Quality of life will be assessed using the five-level EuroQol-5D questionnaire (EQ-5D-5L).56 Fatigue will be assessed using the 13-item fatigue subscale of the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) questionnaire.57 Sleep will be assessed using the Pittsburgh Sleep Quality Index, an 18-item questionnaire which assesses sleep quality and disturbances over a 1-month time interval.58
Intervention acceptability and compliance
Basic costs of the intervention will be recorded (printing of the booklet, phone and postage charges, staff time) to provide an indication of the likely expense of implementing this intervention more widely.
Compliance with the intervention, use of the accompanying website, and satisfaction with the materials will be assessed through a set of questions accompanying the mailed questionnaire at 3-month follow-up. These will include questions about which aspects of the booklet they read, reasons for not reading the booklet (if relevant), how useful each section, the phone call and tailored feedback were, if they used the action plans, if they set goals (and for which behaviours) and if they achieved their goals, things that prevented them from achieving their goals, if they made habits, and a measure of automaticity for each new habit, and use of the website. Responses will be further explored during qualitative interviews (see below). Participants will also be asked to return copies or photographs of their used action plans as an indication of how these are being used. Proportion of intervention calls completed and the duration of the calls will also be recorded.
Qualitative interviews
At 6 months, a selection of participants (n=20) who received the intervention will take part in qualitative interviews. Interviews will explore experiences of the intervention including barriers and facilitators to compliance, satisfaction and perceived effectiveness of the different elements of the interventions, and suggestions for improvement. All interviews will be audio recorded and transcribed.
Calculating the primary outcome
The primary outcome for this study is a CHBRI, which will be calculated based on patients' adherence to the nine target areas that they are encouraged to set goals around within the intervention. These behaviours will be measured as described above. Since a number of key health behaviours are being targeted within the intervention, rather than assess single behaviours the CHBRI assesses simultaneous overall change in more than one. Discussion with oncologists has also indicated that an overall health behaviour change score would be of more value than individual behaviours in convincing health professionals to introduce a lifestyle intervention into the care pathway.
Furthermore, the use of a composite score allows tailoring of the intervention to patient need and choice. This scoring system (a composite score based on adherence to the WCRF guidance vs not) was used previously in the Iowa Women's Cohort, and in 2017 cancer survivors was sensitive enough to show lower all-cause mortality in those with higher scores59 and to show, in cancer-free participants, that those who followed 0–1 vs 6–9 of the guidelines had significantly 35% increased risk of developing cancer.60 Additionally, using a composite score, each additional AICR/WCRF guideline met was associated with 5% reduced risk of developing cancer in the EPIC cohort.61 A CHBRI has also been successfully used in a previous lifestyle study in those at risk for colorectal cancer ‘Project PREVENT’ and was sensitive enough to detect change in response to a lifestyle intervention involving mailed materials.62
Details for the measurement of each behaviour are given above. All measurements are made using reliable and valid tools. Physical activity behaviours (recommendations 1 and 2) will be calculated from pedometer data, and from the Godin Leisure-Time Exercise Questionnaire if pedometer data are missing. Dietary and alcohol behaviours (recommendations 3–8) will be calculated from dietary recall data, and from self-report questionnaire measures if recall data are missing. Tobacco behaviour (recommendation 9) will be calculated from the self-report questions described above. Cut-offs for the target behaviours will be based on the WCRF recommendations (where available) or UK national guidelines. Participants will be classed as meeting the recommendations as follows:
Daily physical activity: physically active for at least 30 min a day or a daily average of 10 000 steps a day;
Fitness: two 30 min sessions of vigorous, aerobic exercise a week;
Fruit and vegetables: five a day or more;
Red meat: 500 g per week or less;
Processed meat: no processed meat;
High calorie foods and drinks: fat 33% or less of total energy intake, and total sugar ≤50 g per day for women, 70 g per day for men;
Fibre: 18 g per day or more;
Alcohol: two or more alcohol-free days a week, and average units per day of 2–3 for women, 3–4 for men;
Tobacco: non-smoker/non-tobacco consumer.
The nine individual behaviours will be equally weighted. To calculate CHBRI, at baseline participants will be assigned an individual score from 0 to 9 dependent on the number of WCRF guidelines met. The same will be calculated at 3 and 6 months follow-up. In addition to the composite score, change in each behaviour will be reported as secondary outcomes.
Sample size
This is a large behavioural outcomes trial aimed at determining whether the ‘Healthy Habits for Life’ brief intervention has an impact on health behaviours, in order to carry out a future trial including biomarkers and clinical outcomes. Based on previous lifestyle randomised trials that have used a CHBRI, the aim is to detect a modest increase in CHBRI of 0.2 SDs at 3 months, and with 80% power and 5% two-sided statistical significance, which will require around 700 participants (350 per group). This will allow for a modest effect size to be detected in an intention-to-treat analysis, to take into account people in the intervention group who do not follow the intervention, as well as those in the control group who change their habits (both of which would dilute the effect). Based on a previous study using the same measure,63 a modest-sized effect (namely, a difference of 0.2 SDs between the conditions) at 3 months would represent an increase of 0.24 on the CHBRI among participants who received the ‘Healthy Habits for Life’ intervention. In real terms, this would mean that these participants would be 24% closer to meeting an additional WCRF recommendation.
The recruitment target is 450 patients into each arm (there is no aim to recruit specific numbers of patients by cancer type). This will allow for drop-out, particularly at the 3-month and 6-month follow-ups. To minimise loss to follow-up, patients will receive two telephone call reminders over 6 weeks if they do not return their pedometers or questionnaires and/or do not complete their dietary recalls.
Data analysis
The primary end point (CHBRI at 3 months) will be analysed by a researcher blind to treatment allocation. Unblinding will occur after the primary data analysis is complete and has been checked and verified by a second researcher. A full data analysis plan will be developed and published prior to completion of data collection. Briefly, baseline characteristics will be reported by each arm using descriptive statistics. The primary analysis will be intention to treat. Linear regression analysis will be used to assess change in CHBRI at 3 months, with baseline CHBRI scores and treatment group as covariates. Repeated measures analyses (eg, mixed modelling) will be used to analyse the baseline, 3-month and 6-month CHBRI scores together. Missing data will be explored to see if they are missing at random, and various sensitivity analyses performed after making different assumptions about the missingness.
Other continuous factors (eg, individual behaviours) will be analysed using linear regression, and categorical factors using frequency tables and χ2 tests, and logistic regression. Exploratory subgroup analyses will be carried out to examine intervention interactions with gender, age, education/socioeconomic status, treatment and tumour type.
With respect to cost-effectiveness, costs associated with the intervention will be recorded (printing of the booklet, phone and postage charges, staff time). A full economic analysis will be conducted within a future, large-scale, RCT with cancer-relevant outcomes. For the qualitative data, thematic analysis will be used to identify the main themes that will form the basis of our results.
Limitations
This study has several limitations that should be noted. With the exception of pedometer and dietary recall data, the outcome measures for the present study will be self-reported and thus may introduce bias into the data collection process. For example, participants may under-report frequency of alcohol consumption on the AUDIT-C owing to fear of being judged on drinking habits. Participants may apply similar reporting strategies when completing other questions relating to health behaviour. However, all outcome measures have been developed using reliable and valid tools. For convenience, the study sample will be recruited from London and the surrounding areas, which may limit the representativeness of the sample to the rest of the UK. A further limitation is the use of research staff to deliver the intervention and the detailed assessment on which the tailored telephone call will be based. If this intervention is to be rolled out within the cancer care pathway, this assessment will need to be shortened. If the current trial demonstrates an effect of the intervention on health behaviours, a pragmatic trial will be needed to determine the effectiveness of this intervention if delivered by health professionals within the cancer care pathway. Future studies will also be required to explore the importance of the individual components of the intervention for promoting change. Finally, because of the nature of the intervention, it will not be possible to blind participants, but all follow-up data will be collected and entered by researchers blind to treatment allocation. Statistical analysis of the primary outcome will also be performed by a researcher blind to treatment allocation.
Strengths
The ‘Healthy Habits for Life’ intervention is a novel approach to improving the health behaviours of people diagnosed with cancer. Based on habit theory and providing evidence-based advice on a healthy lifestyle post diagnosis in a booklet format, it has the potential to meet an identified need for an intervention that can be delivered within the cancer care pathway without prohibitive costs. It is hoped the tailored discussion will encourage patient engagement and could be replicated by a health professional within the end of treatment discussion that patients currently receive as part of their standard care. This intervention could also be incorporated within the Living With and Beyond Cancer Programme introduced in 2014, which includes health and well-being clinics and cancer care review discussions with a general practitioner.
The results of this study will assess the impact of ‘Healthy Habits for Life’ on behaviour (an intermediate outcome) over 3 months and will provide information on whether any changes are sustained up to 6 months. If this brief intervention can promote sustained behaviour change, this will provide the basis for a definitive, large-scale, national, pragmatic RCT to examine effects on cancer outcomes of use of the programme in routine clinical care. Additional funding would be sought for such a trial from Cancer Research UK. If proven to be effective in this context, ‘Healthy Habits for Life’ could make a highly cost-effective contribution to improvements in the long-term survival of people diagnosed with cancer.
Ethical considerations and dissemination
NHS Research and Development approval has been obtained from all participating NHS Boards prior to the start of the trial. Potential protocol modifications will be formally approved by the Research Ethics Committee before being implemented. The amendments will be communicated to the trial registries and outlined at the dissemination of the trial.
Further advice and support on governance and Good Clinical Practice (GCP) issues will be provided by Cancer Research UK and University College London (UCL) Cancer Trials Centre, who provide Standard Operating Procedures for tasks such as obtaining consent, managing and archiving data, access to trial data, training and how to handle breaches of GCP. The trial was prospectively submitted to the International Standard Randomised Controlled Trials (13 November 2014) and allocated the number ISRCTN17421871.
UCL is the sponsor of this trial. The Joint Research Office will monitor and conduct random audits on a selection of studies in its clinical research portfolio. Monitoring and auditing will be conducted in accordance with the Department of Health Research Governance Framework for Health and Social Care,64 and in accordance with the Sponsor's monitoring and audit policies and procedures.
This study has been registered for Data Protection at UCL Records Office (Reference: Z6364106/2014/07/18). Standard procedures following Data Protection Act 1998, the NHS Code of Confidentiality and GCP will be implemented throughout the study. All investigators will have access to the final data set and a completely de-identified data set will be disseminated to a relevant data archive for sharing purposes no later than 3 years after the study close. Study-related documents will be archived at UCL and each participating site at the end of the study for 20 years and in line with all relevant legal and statutory requirements.
An external Trial Steering Committee will meet at regular intervals to oversee the trial. The committee, which is chaired by Dr Gill Hubbard, will include two other independent members, the site principal investigators, the trial co-investigators and a lay representative. Given the short length of the intervention, the low risk of harm and the short follow-up of the intervention, an external Data Monitoring Committee will not be needed and an interim analysis will not be performed. All potential adverse effects and unintended effects of the intervention will be reported to the Trial Steering Committee and Research Ethics Committee where appropriate.
Patients who express an interest to participate in the trial will be posted a consent form to sign and then return in a freepost envelope (see online supplementary material 4). On receipt, this form will be co-signed by a researcher and a copy returned to the participant for their records. Those who return their signed consent form will be randomised to the trial provided it is received before the cut-off date of the end of March 2017. Participants who return their consent forms after this date will not be included. All participants will be informed that they are free to withdraw at any time from the study without giving reasons and without prejudicing further treatment.
Supplementary material 4
The findings from this study will be disseminated to academic researchers and to policymakers through several mechanisms. First, we will employ the usual avenues for dissemination of academic research including conference presentations and journal articles. Second, we will disseminate the research via social media outlets such as the UCL—Health Behaviour Research Centre Twitter account. Third, the UCL and the Cancer Research UK press offices will coordinate press releases of key findings. Finally, key findings will also be fed back to all participating organisations and patients, and through London Cancer newsletters.
Acknowledgments
The authors would like to thank the Cancer Research UK (grant number C1418/A141) for funding this work, and the external members of the Trial Steering Committee for their invaluable input into the study.
References
Footnotes
↵† In memory of Professor Jane Wardle.
Contributors JW had the original idea for the study and obtained the funding. RJB, AF, HC and KW developed the trial protocol and recruitment approach and obtained the necessary permissions with support from AHa. HC is responsible for the dietary recalls. LS is responsible for the activity assessments. MH is in charge of recording patient data and liaising with sites. RR, JH, MM, MK, SC, AHi and KP-J are supporting the contact with patients and providing the necessary data for invitations. RJB drafted the initial manuscript and all authors contributed to edits and revisions. All authors have approved the final version.
Funding Cancer Research UK (grant number C1418/A141).
Competing interests None declared.
Patient consent Obtained.
Ethics approval NRES Committee South Central—Oxford B via IRAS (reference number 14/SC/1369, Approval granted 14 December 2014) with other participating centres providing site-specific approval as per normal IRAS procedures.
Provenance and peer review Not commissioned; externally peer reviewed.