Article Text

Abstract
Objectives To identify patient's views on the functionality required for personalised access to the secondary care electronic health record (EHR) and their priorities for development.
Design Quantitative analysis of a cross-sectional self-complete survey of patient views on required EHR functionality from a secondary care EHR, including a patient ranking of functionality.
Setting Secondary care patients attending a regional cystic fibrosis unit in the north of England.
Participants 201 adults (106 (52.7%) males), median age 29 years (range 17–58 years), entered and completed the study. Inclusion criteria are as follows: a confirmed diagnosis of cystic fibrosis, aged 16 years and over, at the time of clinical stability.
Outcome measures Quantitative responses within 4 themes; (1) value placed on aspects of the EHR; (2) access requirements to functions of the EHR; (3) views on information sent to the EHR and (4) patient feedback entered into the EHR. A ranked score for 15 functions of the EHR was obtained.
Results Highest ratings (% reporting item as very important/important) were reported for access to clinical measures (lung function (94%), C reactive protein (84%), sputum microbiology (81%) and blood results (80%)), medication changes (82%) and lists (83%) and sending repeat prescription (83%) and treatment requests (80%), while sending symptom diaries was less so (62%). Email contact with clinicians was the most valuable communication element of the EHR (84% very important/important). Of 15 features of the EHR (1=most desirable to 15=least desirable), patients identified ‘clinical measures’ (2.62 (CI 2.07 to 3.06)), and ‘access to medication lists’ (4.91 (CI 4.47 to 5.44)), as highest priority for development and the ability to comment on errors/omissions (11.0 (CI 10.6 to 11.5)) or experience of care (11.8 (CI 11.4 to 12.2)) as lowest.
Conclusions Patients want extensive personal access to their hospital EHR, placing high importance on the viewing of practical clinical measures and medication management. These influence routine day-to-day care and are priorities for development.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first UK study to examine patient views and preferences to underpin the future developments of personalised access to a hospital electronic healthcare record.
The strength of the study lies in its use of an informed, diverse patient population, familiar with the long-standing use of electronic health record (EHR) in their routine hospital care and able to provide views on a comprehensive range of access needs, sent information, communication and feedback requirements and ranking of priority areas for future development.
The population studied were selected from a single chronic disease group with generic and also condition-specific access needs to their EHR, which influenced the questionnaire design and the inclusion of certain clinical measures within this.
Introduction
Implementation of integrated electronic health record (EHR) across the National Health Service (NHS) remains a key priority as EHR has the potential to improve quality and efficiency of healthcare provision and support personalised healthcare.1 The EHR is defined as ‘an electronic record of health-related information on an individual that conforms to nationally recognised interoperability standards and that can be created, managed and consulted by authorised clinicians and staff across more than one healthcare organisation’.2 As well as providing substantial benefits to healthcare professionals and clinic practices, EHRs provide an opportunity for the development of personal online patient access to medical records and bidirectional data flow.3 The ambition in the NHS is that all individuals in the UK will be able to view their health records by 2018.4 This will include data from hospitals, community, mental health and social care services.4
Providing personalised online access to healthcare records is considered fundamental to patient-centred care and empowerment.5 ,6 To date it has been piloted in the UK but not fully adopted beyond requesting repeat prescriptions and arranging appointments. Studies within primary care have generally reported benefits associated with online access for individuals, including a feeling of increased control over their own health, greater understanding, improved adherence to care plans and medication,7 ,8 as well as greater transparency, improved multidisciplinary team (MDT) relationships and opportunities for shared decision-making and education.4 ,7 ,9 ,10 In contrast, an anxiety about the security, privacy and content of their patient data has highlighted the ambivalent views that can exist regarding access to the EHR6 and clinicians themselves have often been resistant, citing their own concerns about security, privacy and legal constraints.11 ,12
In contrast to the primary care environment, the evaluation of patient online access to their health records in hospital care has been more limited, partly due to poorer roll-out of EHR. Notable successes have been reported in the USA by Kaiser Permanente and The USA Veterans Association, where online appointment booking, email and test result retrieval have evaluated well.13 ,14 The much poorer implementation of EHR in hospital care within the UK generally has meant that evaluation of patient online access is lacking, with the exception of renal medicine where the implementation of specific features of online access such as the viewing of blood results (Renal Patient View) and the input of physiological measures has delivered some degree of success.15 Overall, however, progress has been delayed and there is a lack of systems that enable patient to view consultations and have comprehensive interactive online communication with their hospital team.
To achieve practical and user-friendly systems requires patient engagement and capturing of their views on functionality of the EHR systems from the outset. A participative approach with patients informing and evaluating health information technology has been suggested as essential.16 With respect to the development of an integrated personal and hospital EHR record, it also offers considerable potential for supporting and engaging patients with chronic disease,17 but it is an area currently lacking in evidence and research.18
Within the cystic fibrosis (CF) regional centre, Leeds, a comprehensive EHR, was developed in 2007 for hospital care, using CF as a chronic disease model.19 New planned, functionalities include full patient access to their personalised secondary care record as well as the ability to share a personalised patient-generated record. The ability for the EHR to incorporate different views, including current problems, current medication, test requests, letters, consultations, allergies and immunisations, is possible as is the linkage to the Apple Health app allowing patient-held data to be viewed from the secondary care systems. Rather than be monitored from a distance, the patient retains ultimate ownership and responsibility for their own health and data which can only be viewed with patient consent. In this programme of development, our aim was to underpin all stages of the process with an evidence-based approach to implementation that accounted for user views and preference.
The objectives of this study were twofold; first, to identify patient views on the tools and functionality that require development for personalised access to the secondary care EHR and, second, to identify patient-led priorities for functional development.
Methodology
Study and questionnaire design
We conducted a cross-sectional, self-complete questionnaire survey using purposive sampling to recruit consecutive attendees at a regional adult CF centre in Leeds, UK. Before administration, the questionnaire was designed using the existing evidence base for patient interaction with their healthcare record, input from EHR developers and detailed feedback obtained from piloting of the questionnaire with four patients. Final revision of the questionnaire was undertaken before use.
Setting and sampling
The prospective cross-sectional survey was conducted over 5 months from 5 October 2015 to 2 March 2016. Patients were recruited from outpatient and in-patient settings to minimise environmental bias. While developments are aimed to be generic and fully configurable for any disease, a CF population was chosen to test out the development of access to EHR within secondary care due to their regular contact with primary care, community pharmacy, home care delivery services as well as secondary care and also the presence of multiple comorbidities within this patient group. The regional unit also had an established EHR in use since 2007 with >400 codes accounting for all aspects of clinical care, which were registered under the systematised nomenclature of medicine clinical terms (SNOMED CT)19 ,20 and 9 years of digital data use. The technology was therefore robust, although providing unique digital data unavailable to other patient groups with chronic disease within the same hospital. This infrastructure offered the capability for delivering patient requirements and secure data sharing and a practical context for recruitment of this sample.
Participants and data collection
Study participants were invited to take part in the study by the specialist research nurse as they attended routine outpatient clinic appointments or ended their in-patient care, each at a time of clinical stability.
Eligibility criteria for participation were: (1) a diagnosis with CF, (2) attending the Adult Regional Unit for Cystic Fibrosis for routine care, (3) aged 16 years and over (4) and at a time of clinical stability, to minimise further respondent burden at a time of acute illness. No exclusion criteria were stipulated.
Study size
The study size was determined according to the following calculation, assuming a margin of error of 5% and a confidence level of 95%:
Sample size=(distribution of 50%)/(margin of error %/confidence level score)2=(0.5×(1–0.5))/(0.05/1.96)2=384.16.
A finite population correction was then applied for the total population sample of 420 patients: True sample=(sample size×population)/(sample size+population−1)=201.
Sample size=384.16×420/384.16+420–1=201 participants.
Patient characteristics
Participants were asked to record their age and gender. The number of in-patient admissions during the past year was also collated as was lung function (recorded as forced expiratory volume in 1 s (FEV1%)) and body mass index (kg/m2).
Patient views about personalised access to their EHR
Participants were asked their views regarding personalised access to their EHR across four themes, each containing a number of functions for which patients were asked to answer on a 6-point Likert rating scale: very important (1); important (2); slightly important (3); ordinary (4); not important (5); very unimportant (6), with the same scale used for each function within each of the four themes. In total, 58 questions were posed. The themes incorporated were:
Functionality considered valuable within the EHR;
Functions of the EHR patients would like to have access to;
The information patients wished to send to their EHR;
The communication and feedback patients wished to input into their EHR, including communication with clinicians, patient experience, comments on errors or omissions, and future wishes such as living wills and advanced directives.
Patients were then asked to rank 15 functions in the order of importance from 1 to 15 to inform priorities and development of the EHR. Functions were chosen according to their generalisabilities to other populations with chronic disease and limited to a number considered to be feasible for patients.
Data analysis
Patient characteristics were presented using descriptive analysis according to whether data were normally distributed (mean (SD)) or skewed (median (range)). Rated questions within each category were presented through proportion and cumulative percentages. Comparison of rating for each question was analysed using the χ2 goodness of fit. Forced rank scoring was presented as mean rank score (CI) for each list item. Where missing data were >3% of the item responses, only the available data were analysed. Where missing data were >3%, the data item was partitioned to compare whether population characteristics (age, gender or number of hospital admissions) differed between responders and non-responders. The impact of age on rating response was assessed using multinomial regression analysis, with age as a continuous variable and response as three categories: very important/important; quite important/ordinary; and not important/very unimportant.
Data were analysed using SPSS V.22.0 (Chicago, Illinois, USA) and results were classed as statistically significant when p<0.05.
Results
Of the 204 patients invited to participate in the study, a total of 201 patients (106 (52.7%) males) consented to participate and complete the questionnaire. Reasons given for declining participation in the study were current health worries that superseded taking part a perceived lack of understanding of computers and technology and lack of interest in the study. The median age was 29 years (17–58 years), and mean body mass index was 23.5 kg/m2 (±4.3). The patients attend routine two monthly appointments and were noted to have a wide range of disease severity, with mean FEV1 of 65.5% (±25.1), ranging from 15% to 120%, and at all stages of the disease spectrum and a median number hospital admissions within the previous year of 1 (range 0–8).
Owing to the small numbers within some of the six Likert categories, these were collapsed further to three categories prior to further analysis by combining the following: (very important/important; quite important/ordinary; not important/very unimportant). These categories were then used throughout the analysis.
Value placed on functionality within the EHR
The patients reported that the EHR had a particular value for relaying information on areas that influenced their immediate clinical management, but placed lower ratings on access to information and knowledge portals (table 1).
Patients rating of value they placed on items within an EHR according to functional categories of the questionnaire
Patient access to the EHR
The area that patients most wanted to access included physiological and anthropometric measures, changes in and list of medications and access to appointment reminders and consultation summaries (figure 1). Although >50% of respondents regarded each category as very important/important, vaccination information, genetic mutation, type and dates of intravenous antibiotic treatments and tracking of admissions and referral on to other departments were considered important by fewer respondents.

Response rates for functions of the EHR that patients wished to access according to functional category. χ2 goodness of fit indicated significance at <0.001 for all items. Missing values (n): lung function; change in medications; GP letters; Vitamins Allergies Genetics; dates of antibiotics; types of antibiotic; referral to other departments; consultation summary; sputum; blood results (n=1) List Medication; bone scan; date of admission; appointment reminder; appointment times (n=2); weight; CRP; date of vaccination (n=3); blood glucose (n=5). CRP, C reactive protein; EHR, electronic health record; GP, general practitioner.
Information sent to the EHR
Sending information to the EHR by the patient was differentiated into the four subcategories of physiological measures, patient-generated information and treatment/prescription and appointment scheduling information (figure 2). In total, 60% of patients responded that completion of a previsit clinic interview to highlight concerns prior to the appointment was very important/important, although fewer (50% or less of participants) considered that completing previsit data fields for food intake and exercise, or scales for quality of life, mood and pain was important.

Information and requests that patients would like to send to their EHR according to functional category. χ2 goodness of fit indicated significance at <0.001 for all items. Missing values (n): send lung function; weight; blood glucose measures; exercise diaries; food and enzyme diaries; mood and feeling scales; request for appointments (n=2); repeat prescriptions; oxygen saturations; blood pressure readings; weight; symptom diaries; pain scales; quality-of-life measures (n=3); pre-clinic interviews (n=4); send blood glucose measures (n=5); ordering of treatment (n=6). EHR, electronic health record.
Communication with the clinical team
More than 80% of respondents regarded direct email contact with the clinicians as high in importance (figure3). Feedback on drugs and treatment was also important as was sending questions to inform the basis of their next clinic appointment. Their longer-term care informed by advanced directives, feedback of their experience of care and organ donor wishes were more diverse in response (figure 3). The question regarding advanced directives was omitted by 7% respondents. They were not different in age (29.3 (±10.3) versus 30.3(±8.9) years, p=0.78), median number admissions (0 (range 0–4) versus 1 (range 0–8), p=0.75), nor proportion of male gender (42% male versus 53% male, χ2 (1)=0.6, p=0.58)) for non-completers compared to completers—therefore, only available data were analysed. Similarly, there were no differences for the 10 patients (5%) who did not complete the question for donor wishes.
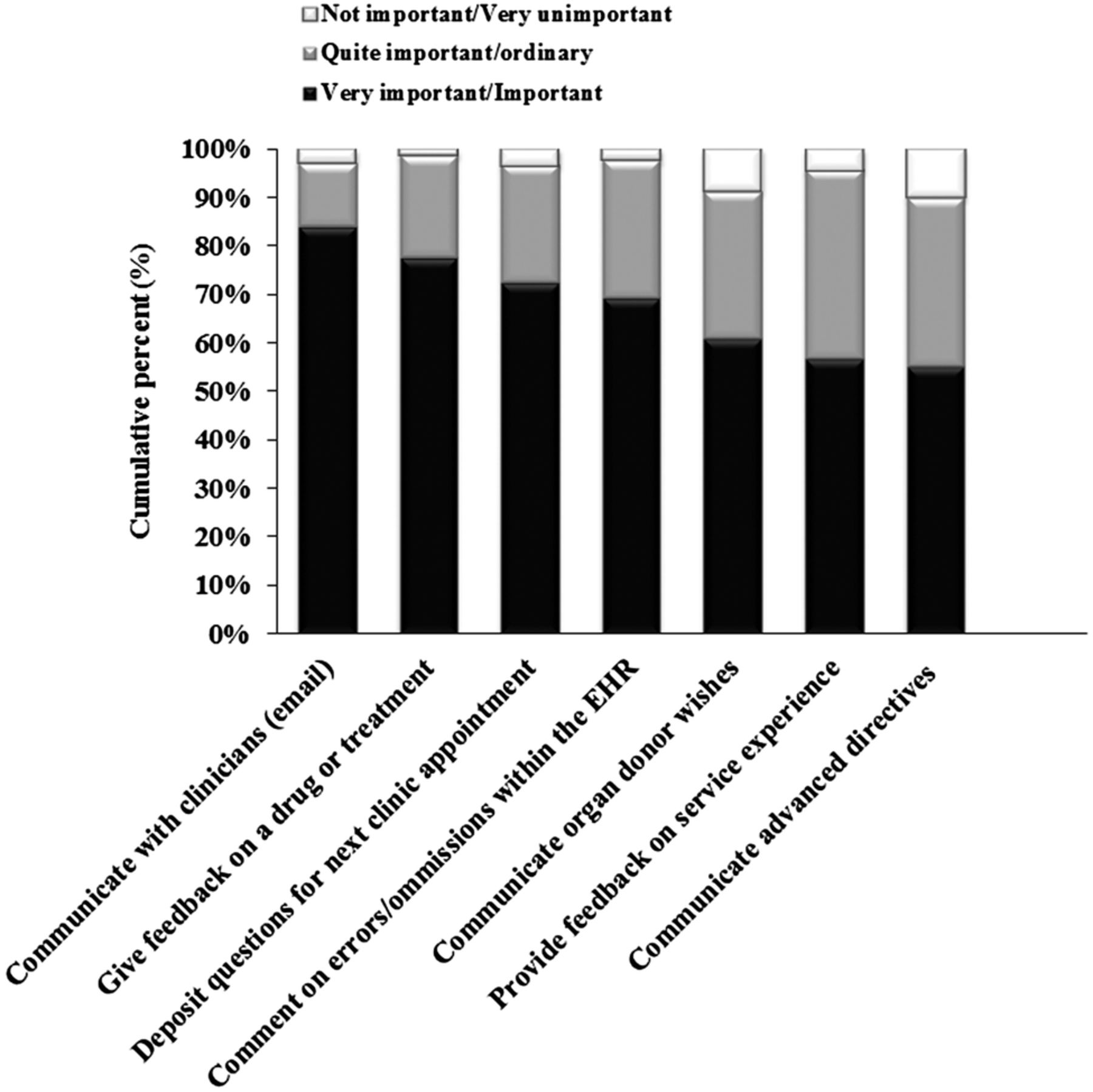
Communication and feedback through the EHR according to functional categories. χ2 goodness of fit indicated significance at <0.001 for all items. Missing values (n): communicate with clinicians by email; provide feedback on service experience; deposit questions for next clinic appointment; give feedback on a drug or treatment (n=3); comment on errors/omissions (n=4); communicate organ donor wishes (n=10); communicate advanced directives (n=14). EHR, electronic health record.
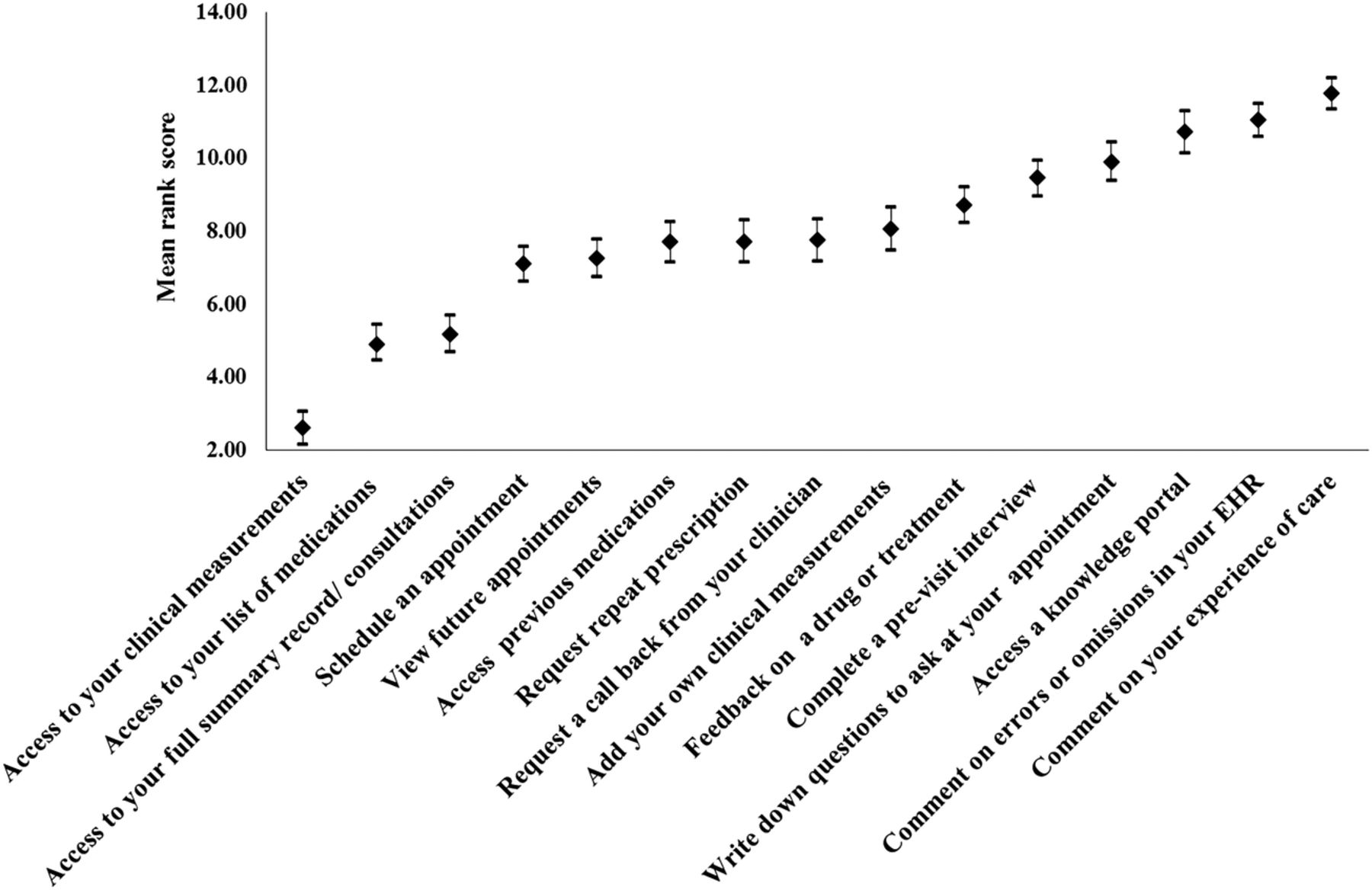
Ranked functionality of the EHR
Respondents ranked functionality from 1 to 15 across functions. Direct access to clinical measures was considered the most important as was access to list of medications (figure 4). In contrast, the ability to comment on experience of care and to comment on errors or omissions in the EHR were ranked lowest. In total, 7.5% of patients did not rank this section or had ‘spoiled’ scores due to inaccuracies (attributable to rating functions on a 1–15 scale rather than ranking these in order). They were not different in age (30.0 (±8.9) versus 33.3(±10.2) years, p=0.25), median number admissions (1 (range 0–8) versus 1 (range 0–4), p=0.97, p=0.97), nor proportion of male gender (47% male versus 49% male, χ2 (1)=0.2, p=0.79)) for non-completers compared to completers—therefore, only available data were analysed.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patients ranked function across 15 items of an EHR. Error bars indicate 95% CIs. Missing values (n=15).
The impact of age on rating of functionality was also examined using multinomial regression analysis (not important/very unimportant as the reference category). Age was not predictive of any rating for individual functions with the exception of sending food and enzyme, pain and also exercise diaries to the EHR. With increasing age, patients were less likely to consider it very important to send a food/enzyme diary to the EHR, compared to not important/very unimportant (OR 0.91 (CI 0.86 to 0.96, p<0.001). Similarly, for pain diaries (OR 0.94 (CI 0.89 to 0.99, p<0.02), and exercise diaries (OR 0.95 (CI 0.91 to 0.998, p<0.04), patients were less likely to respond that this was important compared to unimportant with increasing age. Finally, ANOVA was used to assess differences across age groups for ranking of function, with the only observed difference being the ability to request repeat prescriptions, where older patients >50 years ranked this significantly lower (and therefore of greater importance) than younger age groups (F4,181=3.89, p=0.005).
Discussion
This is the first UK study to examine patient views and preferences to underpin the future developments of personalised access to a hospital electronic care record. Overall the results demonstrated that patients want considerable interaction in terms of access to all aspects of the EHR, including results, clinical measures, engagement in sending and requesting information prior to appointments, viewing medication, requesting prescriptions and communicating by email with their doctor. These priorities align with the EHR services most used by patients within primary care,5 ,13 ,21 ,22 and are in agreement with studies that reveal that patients now require comprehensive functionality, which is greater than merely viewing their information.23–25
Four themes were included in the questionnaire: perceived value, access needs, sending of information to the EHR and communication and feedback. This choice was based on previous research which indicates that patients value novel content relevant to their immediate and ongoing care, place critical importance on access to information, including clinical measures and resources that help in management of their condition,23 and desire content which enables communication with clinicians and contains a high level of functionality.14 Other included functions were those already shown to be related to improvements in effectiveness and efficiency, including improved self-management associated with access to appointment scheduling and repeat prescriptions requests,14 improved rates of medication adjustment in chronic conditions associated with access to clinical data,26 enhanced patient safety through identifying medication list errors27 and increased patient satisfaction and experience of care facilitated by communication links within the EHR.14 This alignment with the evidence base contributed to relevant and robust questionnaire content.
The value placed by patients on functions within the EHR was heavily weighted towards practical measures that helped in their day-to-day management such as lung function, weight, sputum microbiology, blood results and medication lists. This was supported by their high ratings and preferences for accessing similar measures. A previous retrospective evaluation of ‘Renal Patient View’, which has enabled patients with kidney disease in the UK to view their results and input clinical measures online, has indicated similar findings,28 and that viewing of blood results attracts the greatest number of page views. Current findings have extended this further and indicate the broader access to consultation summaries, referral pathways, medication lists, vaccination and genetic information that patients with chronic disease also wish to engage with. This demonstrates that patients are focusing on practical measures which appear to be an important aspect of future personalised access.
User engagement in sending information through their personal healthcare record to the EHR is regarded as crucial to its longer-term success.29 The highest proportion of patients (83%) regarded the function of sending prescription requests as important/very important, supported by similar ratings for patients who wished to access their current list of medications (78%) and changes in medications (82%). Studies indicate that patients appreciate access to their medication record.30 This is especially true within chronic disease management, where the challenges associated with multiple changes in medication have resulted in positive patient feedback about the incorporation of individual medication schedules into list-based views.31 In terms of pharmacy management, using online repeat prescriptions offers further advantages to patients and clinicians alike. While repeat prescription ordering is already in place in primary care systems, the high cost therapies prescribed in hospital care linked to pharmacy systems enable an accurate audit of pick-up rates and can act as a trigger for patient reminders. By linking such data with secondary care, healthcare professionals would allow prescribers to adjust treatment according to patient need and trigger patient education and support to individuals struggling with treatment. These practical considerations of medication management apply across all chronic disease conditions and offer immediate advantages of EHR for drug safety, management and collaborative relationships between patients and clinicians.32 ,33 Patients have, therefore, placed particular importance on improving interaction with prescribing which may have important consequences for adherence.
In contrast, studies suggest that self-reporting of clinical and other data measures has generally been underused in EHRs.28 ,34 Fewer patients in the current study (40%) regarded the sending of information relating to food, activity, mood and quality-of-life measures as an important function of the EHR; all factors that can augment the diagnostic and therapeutic process through improved self-monitoring that can maintain clinical stability.35 The review of exercise, dietary intake and pancreatic enzyme replacement diaries are, therefore, important elements of care that aid monitoring of weight and lung function that are predictors of survival.36 ,37 With depression present in up to 33% of the adult population with CF, consensus guidance also advocates routine screening for anxiety and depression.38 Our study did not address the reasons why patients might rate these functions less favourably, but to engage patients more fully in their care, it is likely a variety of considerations should be addressed. Concise and validated scales such as the Patient Health Questionnaire (PHQ-9), General Anxiety and Depression Scale (GAD-7) and a number of pain scales have already been shown to be successful in patient management.39 ,40 They are simple measures that have the potential for integration into the EHR alongside an alert system for patients who might require early intervention ahead of clinic appointments. Finally, a qualitative study by Kerns et al23 has supported the view that the positive influence of their clinician plays a vital role in influencing patient engagement in all critical components of their EHR,23 ,34 suggesting that a consistent MDT approach is required throughout all phases of implementation. Currently, however, patients either perceive or place less importance on sending patient-reported outcome measures to the EHR.
In contrast, patients placed a high value on wanting to be able to communicate with their clinician by email through secure messaging; 82% responding this was an important function. While debate continues as to how this affects doctor–patient relationships, a recent systematic review has concluded that, within primary care settings, simple self-limiting conditions were easily managed although more complex problems were not.5 The monitoring and evaluation of how patients with a chronic disease communicate with their healthcare team will be crucial in determining its effect on workload, number of admission appointment attendances and overall adherence to therapies as the EHR system rolls out. It is promising that where EHR systems have been integrated across primary and secondary care, patients and healthcare professionals have endorsed its use; clinicians reporting that secure messaging has improved patient engagement and the relationships patients have with their healthcare team.34
In contrast to the rating of function that provides a measure of importance for each item, ranking enables patients to prioritise function, providing additional information that aids in development of the EHR. Patient knowledge and understanding helps to inform this process and it is therefore of note that while clinical measures and access to medication information ranked highest, access to a knowledge portal ranked in the bottom quartile of functionality for patients. This contrasts with other findings that have reported the benefits that patients perceive from the inclusion of links to personalised recommendations, resources and tools that help them to manage their condition,23 the positive impact on appointment attendance41 and the advantages offered through patient peer support.42 Although we did not evaluate further, one possible explanation is that our population is young, has had exposure to the EHR interface during clinical consultations for 9 years and the ability to gain familiarity with graphical presentations and lists of clinical measures at every appointment. In contrast, knowledge portals in CF are relatively new and there is limited evaluation of access and use, with one study indicating that only 35% of patients with CF report the internet to be a source of information.43 Age was noted to have a minimal impact across rated and ranked responses and may reflect an accepted integration of technology across the cohort. With the exception of repeat prescription requests that had lower priority in adults >50 years, no differences were observed in the ranking of individual functions across age groups in the study. Similarly, age had no influence on rating of responses, with the exception of symptom diary completion, where the ability to send pain, exercise and food and enzyme diaries was regarded as more important with age. Shown to enhance self-monitoring and maintain clinical status through early intervention,35 these can also be considered time consuming and burdensome. It suggests that with maturity, patients may acknowledge their value more.
The ability of ranked scores to inform future practice and policy recommendations remains important. Access to clinical measures, list of medications and full summary record were ranked highest by patients but require accurate interpretation to be of use.44 Health literacy and numeracy skills may serve as barriers to full utility of the patient portal, which suggests that clear lines of responsibility and dedicated resources are available to ensure that implementation of EHR is effective. This includes education on the safety and privacy mechanisms of the EHR to preserve confidentiality of data and the development of visual data that highlights normative limits and enables correct interpretation by patients. Addressing clinician workflow and training needs for the EHR will also be important. Contractual processes that provide defined training and ensure that quality standards are maintained have been described as essential.5 The reorganisation of workflow and practice to accommodate these areas will, therefore, require shifts in resource and working practice as EHR develops.
The study itself has inherent limitations. We have used a single chronic disease as a research sample, although it has multisystem involvement and is likely to reflect a number of individual factors that influence patient response, specifically in relation to clinical priorities, stage of illness, number of comorbidities and social support. These data were not collected, although we aimed to minimise these confounders by recruiting a representative patient sample from consecutive appointments and clinics and succeeded in recruitment of a broad age group, proportionate in gender, with a wide range of disease severity evidenced by lung function measures of 15–120% (FEV1). Although underpinning explanations for patient responses were absent, where qualitative responses may have offered greater depth and clarification, the use of a cross-sectional questionnaire enabled rapid feedback from an adequately powered sample of the clinic population. Importantly, the list of functionality is not generalisable to all populations. We concentrated on key measures that our population recognise and understand. However, many of our patients have multiple systemic complications relating to the disease. Up to 40% of our population have diabetes and, in this patient group, parameters such as blood glucose, renal function, blood results will be relevant and common to other diseases. It is also important to note that 7.5% of patients did not rank or had spoiled scores for the section on experience of care and on errors or omissions within. This was primarily due to the question format where patients attempted to rate rather than rank responses. Respondent burden is also an important consideration. Ranked function was reduced to 15 items, but fewer items may have proved more optimal. These observations are important in rationalising future questionnaire design.
The study also has a number of strengths. A high response rate of 98.5% was aided through long-term patient collaboration and familiarity with clinical research in our department. This was also an informed patient community who have observed the use of an EHR at all clinic appointments during the past 9 years; able to view graphical data of their lung function, weight, liver function, current medication lists and the incorporation of information on immunisations, procedures, lung microbiology, allergy and other significant components of their care. They are unusual in having had this available, and the opportunity to understand some of the functions of the EHR and how this information might be used collaboratively at clinic appointments. Their comment on aspects of the EHR they would like to access has therefore come from a more informed base. Involving patients in the design and functionality of new systems is considered crucial and is underpinned by the disparities observed between users and clinicians.45 The strength of this study is therefore in its collaborative approach to developing an EHR system.
In conclusion, patients have expressed their perspectives and preferences for functional access to their EHR. In a clinic population with chronic disease, and of predominantly younger adults, patients wanted comprehensive functionality within an EHR and prioritised access to clinical measures, medication lists and summary consultations as those functions most important to them. Increasing age had a minimal effect on rating or preference of function. The approach we have taken in integrating patient preferences and feedback at the earliest stage of development is endorsed by others.45 ,46 This study has, therefore, enabled us to establish those functions most important for patients, and has informed the preliminary design of an integrated hospital healthcare record for future testing and evaluation in a population with chronic disease.
References
Footnotes
Contributors HW involved in the conception, design, data analysis, interpretation, drafting/critical revision of the work and approved the final manuscript. LG involved in data acquisition and critical revision, and approved the final manuscript. AW involved in data acquisition and critical revision, and approved the final manuscript. DGP involved in conceptualisation, design, data interpretation and critical revision, and approved the final manuscript.
Funding This work was supported by Endeavour Charitable Health Trust.
Competing interests HW and DGP were funded by Endeavour Charitable Health Trust to undertake this study. DGP has undertaken development work for Egton Medical Information Systems.
Ethics approval This was deemed a research study by Leeds Teaching Hospitals Trust. The study was granted ethical approval from the National Research Ethics Service London and Hampstead REC Committee (REC No: 15/LO/1428).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Extra data can be accessed via the Dryad data repository at http://datadryad.org/ with the doi:10.5061/dryad.1pm91.