Article Text

Abstract
Objectives To test the feasibility of conducting a controlled trial into the effectiveness of a self-management programme integrated into stroke rehabilitation.
Design A feasibility cluster-randomised design was utilised with stroke rehabilitation teams as units of randomisation.
Setting Community-based stroke rehabilitation teams in London.
Participants 78 patients with a diagnosis of stroke requiring community based rehabilitation.
Intervention The intervention consisted of an individualised approach to self-management based on self-efficacy. Clinicians were trained to integrate defined self-management principles into scheduled rehabilitation sessions, supported by a patient-held workbook.
Main outcomes measures Patient measures of quality of life, mood, self-efficacy and functional capacity, and health and social care utilisation, were carried out by blinded assessors at baseline, 6 weeks and 12 weeks. Fidelity and acceptability of the delivery were evaluated by observation and interviews.
Results 4 community stroke rehabilitation teams were recruited, and received a total of 317 stroke referrals over 14 months. Of these, 138 met trial eligibility criteria and 78 participants were finally recruited (56.5%). Demographic and baseline outcome measures were similar between intervention and control arms, with the exception of age. All outcome measures were feasible to use and clinical data at 12 weeks were completed for 66/78 participants (85%; 95% CI 75% to 92%). There was no significant difference in any of the outcomes between the arms of the trial, but measures of functional capacity and self-efficacy showed responsiveness to the intervention. Observation and interview data confirmed acceptability and fidelity of delivery according to predetermined criteria. Costs varied by site.
Conclusions It was feasible to integrate a stroke self-management programme into community rehabilitation, using key principles. Some data were lost to follow-up, but overall results support the need for conducting further research in this area and provide data to support the design of a definitive trial.
Trial registration number ISRCTN42534180.
- REHABILITATION MEDICINE
- PUBLIC HEALTH
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first feasibility trial of an integrated approach to stroke self-management; study recruitment and findings support further research to test the intervention in a definitive trial.
Community stroke rehabilitation teams had a high turnover of staff, and training needs were higher than anticipated, but intervention fidelity was maintained.
The intervention requires some modification to be more accessible for those patients with cognitive and communication impairments, and for those having less than six sessions of rehabilitation.
Introduction
Significant improvements have been made in the quality and effectiveness of acute stroke care across the developed world.1–3 But variation in the availability of post-hospital rehabilitation and support for self-managed activities still exists,3 ,4 and the prevalence of mood disorders and social isolation post-stroke remains high.5–7 As the overall global burden of stroke increases,1 expenditure on the direct and indirect costs of stroke care is likely to rise, and in the UK this currently constitutes 5% of the total National Health Service (NHS) budget (£8 billion).8 Stroke and associated care models are still largely defined by acute medical ideologies and there is an inequity in attention to address long-term psychological and social sequelae.9–11 Arguably, unmet needs post-stroke could be exacerbated by care models that foster dependency on professional expertise in the acute stages, combined with a paucity of programmes to facilitate coping and self-management in the longer term.
One alternative to existing care models is the use of self-management programmes (SMPs) that build on growing evidence from systematic reviews in other long-term conditions.12–15 SMPs can be ‘provider-based’, delivered by healthcare professionals integrated into usual care, or ‘patient-based’, when supplied in addition to care through group or individual education.13–16 Broadly, self-management focuses on those actions individuals and others take to mitigate the effects of a long-term condition, and to maintain the best possible quality of life.12–14 The variation in programmes makes it difficult to compare outcomes, but effective SMPs can improve mental well-being and quality of life, and reduce hospital readmission rates.12–16
The UK National Stroke Strategy, in 2007, advocated self-management initiatives to address long-term unmet needs,17 and national guidance recommends that all patients be offered training in self-management skills.18 Research to develop and evaluate stroke SMPs mainly comprises feasibility and phase II trials of group-based programmes, which, while demonstrating some impact on function, mood and quality of life,9 ,19 ,20 will not be accessible for certain patients with communication and cognitive impairments.21 We hypothesised that an individualised stroke self-management intervention that can be integrated into existing rehabilitation may extend the reach to more patients.11 ,19 ,22
Following the Medical Research Council Framework for the Development and Evaluation of Complex Interventions,23 several studies have been conducted to inform the development of an individualised SMP.22 ,24 The Bridges stroke SMP is based on social cognition theory and self-efficacy,25 ,26 and incorporates a patient-held workbook used by rehabilitation professionals to support self-management skills. Studies have demonstrated preliminary proof of concept and feasibility when provided in addition to rehabilitation.22 ,24 However, an SMP delivered in addition to routine stroke rehabilitation has cost and time implications, especially when utilising an individualised approach. If the same programme could be integrated into existing rehabilitation, this may offer a solution that could be both clinically valuable and cost-effective.
The aim of the study was to test the feasibility of conducting a cluster-randomised controlled trial into the effectiveness of a stroke SMP (Bridges) integrated into community rehabilitation. We aimed to evaluate key trial parameters such as recruitment and retention of participants, randomisation, utility and sensitivity of outcome measures, levels of missing data and preliminary indications of effectiveness to inform calculation of a sample size for powering a full trial. An estimation of resources required to deliver the intervention and indications of likely cost-effectiveness were also investigated. Fidelity of the intervention delivery, training required and acceptability of the intervention to patients and clinicians were evaluated.
Methods
Design
A feasibility cluster-randomised design with a nested process evaluation was utilised with community stroke rehabilitation (CSR) teams as units of randomisation. Sites were eligible if they comprised multiprofessional teams with stroke specialist skills delivering post-hospital rehabilitation according to quality criteria set out in UK National Clinical Guidelines for Stroke.18 Current models of CSR in the UK provide rehabilitation by therapists (occupational therapists, physiotherapists and speech and language therapists) and non-professional support workers in patients’ homes.
Selection of sites
Twenty-one CSR teams from outer and inner London boroughs with ethnically and socially diverse populations were sent information about the study via a group email used for a pan-London Stroke Rehabilitation Network. Six teams agreed to take part and four teams were selected as they had not taken part in any previous self-management training in the previous 12 months, and met all other eligibility criteria. Team consent was obtained from the lead clinician acting as a cluster guardian.
Randomisation
Allocation of CSR teams to either an intervention or control cluster was carried out once teams had been recruited and given consent to participate by a local clinical trials unit via simple randomisation at 1:1 ratio without matching.
Intervention
Intervention site teams undertook training on theory, research and practical application of the Bridges SMP. Training delivery in intervention sites adhered to a predetermined protocol based on seven key principles of the SMP; these were developed through previous research and in consultation with key stakeholders (table 1).22 ,24
Seven key principles of the Bridges stroke self-management programme
The Bridges SMP aimed to be distinct from routine stroke rehabilitation provision in two main ways:
One-to-one rehabilitation sessions using seven principles integrated into each therapy session to support self-management activities.
A stroke workbook that included vignettes, activities, ideas and solutions from other stroke survivors for successful self-management, and space to record and reflect on goals and progress.
Recruitment
Consecutive patients with stroke referred for CSR were screened by the community rehabilitation teams, recruited within 2 weeks of referral to the CSR team and consented by research staff not blinded to allocation. Patients were eligible if they had a confirmed diagnosis of stroke and could follow a two-stage command such as close your eyes and nod your head, and read simple text and/or have a carer to assist. Criteria were informed by previous research.22 ,24
Stroke participants allocated to the intervention clusters were introduced to the stroke workbook and the seven key principles of self-management by the therapist integrated into existing CSR sessions. Participants in control sites received CSR as usual, which included access to physiotherapy, occupational therapy, and speech and language therapy, if required.
Sample size
As this was a feasibility study, a prospective sample size calculation was not conducted. We aimed to recruit 80 stroke participants across the four sites over 14 months, which appeared realistic given the teams’ referral rates.
Assessments
Data were collected in participants’ homes by research assessors blinded to group allocation. Clinical outcomes were collected at baseline (within 2 weeks from starting rehabilitation), 6 weeks and 12 weeks after baseline.
Feasibility, fidelity and acceptability
The feasibility of recruiting and retaining participants was assessed from study records, and characteristics of those who were not eligible, consent and completion rates were analysed. Participants’ age, sex, social support, socioeconomic status and medical history, were described and compared between groups, to test randomisation.
Fidelity and acceptability of the delivery of the intervention were determined by observing a proportion of rehabilitation sessions, using a checklist to record patient and professional activities and behaviours against each principle component of the SMP. The checklist was piloted to enable a method to compare self-management support delivered in intervention and control sites that could be used in a larger trial. Patients and clinicians were interviewed in each site, to compare their experiences and understanding of self-management; those in the intervention site were specifically asked about the feasibility and acceptability of using self-management strategies and workbook.
Clinical outcomes
Clinical measures found sensitive to change in previous self-management trials and validated in stroke populations were utilised,9 ,20 ,24 and included the Stroke and Aphasia Quality of Life (SAQOL) scale,27 Nottingham Extended Activities of Daily Living Scale (NEADL) of functional ability,28 Stroke Self-Efficacy Questionnaire (SSEQ),29 ,30 and Hospital Anxiety and Depression Scale (HAD).31 The Medical Outcomes Trust's Short Form 12 (SF-12) was included to provide a generic measure health-related quality of life.32 Ease of data capture and levels of missing data were assessed for each outcome measure.
Although the study was not powered, a statistical analysis was conducted to gain a preliminary indication of effectiveness and of the feasibility of such analysis. The analysis enabled an assessment of the sensitivity of different outcome measures and provided a basis for a sample size calculation for the full trial.
Statistical analysis
Considering feasibility, we compared levels of missing data between intervention and control sites using Fisher's exact test. In order to adjust for age, a multilevel regression model was fitted to each clinical outcome. This is a common approach to cluster-randomised clinical trials, and utilises all data, even if a participant is missing some. Group allocation was purely on the basis of site, forming an intention-to-treat analysis. Interparticipant variability was represented as a random intercept, and age, time and group allocation were included as fixed effects. Group differences were quantified at 6 and 12 weeks, and a composite null hypothesis that both were equal to zero was assessed by Wald tests. This represents no mean difference between groups in how the outcomes change over time. These analyses were conducted in Stata V.11.2 software (StataCorp, College Station, Texas, USA), using command ‘xtmixed’.
Sample size calculations for a future trial were calculated using Stata software (command ‘sampsi’), assuming SDs observed in this study for NEADL and SAQOL, 80% power requirement and a range of putative minimum clinically important differences (MCIDs): NEADL from 2 to 5 in steps of 0.1, and SAQOL from 0.1 to 0.5 in steps of 0.01.
Economic analysis
To estimate the resources involved in delivering stroke rehabilitation in each site, data were collected at individual patient level from therapist records on the number of CSR sessions, and face-to-face contact time in minutes. Physical resources were converted to costs using validated national unit costs, in British pounds, 2012.33 Costs associated with patient-related non-face-to-face time was calculated under three alternative assumptions. Total costs were compared across sites.
The feasibility of capturing health and social care utilisation from participants was assessed using a bespoke self-report questionnaire administered to participants at weeks 6 and 12. Items included contacts with general practitioner (GP), practice nurse or other professionals, social care, and help from family and friends. The purpose was to explore if use of SMP reduced demands on other services, compared with the control group. EuroQol (EQ-5D) health state utility weights, using a published transformation33 of the SF-12 profile measure of quality of life, was to be tested for deriving quality-adjusted life year (QALY) gains.
Results
Intervention fidelity and acceptability
Overall, 63 occupational therapists, physiotherapists, speech and language therapists, and rehabilitation support workers, received training. This number was higher than expected because of clinician turnover.
The feasibility of monitoring intervention fidelity was evaluated through observations of a consecutive sample of 14 participants (18%, control n=7, intervention n=7). The checklist was feasible to use and identified whether CSR incorporated behaviours and activities relating to core self-management principles. Clinicians in the intervention sites showed use of between five and seven self-management principles, whereas those in the control site showed evidence of using two or less.
A consecutive sample of patients (n=23) were interviewed and focus groups were carried out with all clinicians (n=34) including occupational therapists, physiotherapists, speech and language therapists, and rehabilitation support workers across sites, at the end of the trial, to explore intervention feasibility and acceptability. Findings showed shared understanding of self-management in patients and clinicians within the intervention clusters, which reflected the underlying principles of the SMP and will be reported more fully elsewhere.
Feasibility
Recruitment rates: Four sites were recruited from six CSR teams in London that expressed an interest and were eligible; excluded sites had either previously taken part in self-management training or were likely to undergo significant reorganisation during the trial period of 22 months. Participant recruitment occurred between July 2012 and August 2013, 138/317 patients (44%) were eligible to participate across four sites. Recruitment took 14 months, which was longer than the anticipated 10 months. This was due to restructuring of some community services and a requirement for further training for new staff. Of those eligible and invited to participate, 78/138 (56%) consented and were recruited to the trial (at a rate of 5.57/month). Control sites recruited n=38 compared with n=40 in intervention sites. The main reason for non-eligibility was patients not requiring six rehabilitation sessions or more (58%), and patients with cognitive and communication impairments (17%). The latter were excluded as a certain minimum level of cognitive and communication ability (ie, ability to follow a verbal or non-verbal two-stage command) was required for the intervention, which is based on cognitive interaction between practitioner and stroke survivor.
Completion rates
The research protocol was successfully delivered and outcome assessors remained blinded to the intervention throughout the duration of the trial. Figure 1 shows rates of completion varied slightly between control and intervention sites. Thirty-nine participants (98%) completed baseline measures and 36 participants completed week 12 outcome measures (90%) in intervention sites, compared with 35 (92%) completing baseline outcomes and 30 (79%) completing week 12 outcomes measures in control sites. Reasons for withdrawal included ill health and change in family circumstances, with only three cases of withdrawal due to burden of outcome measurement (nature of the questions (n=1) and the volume of questions (n=2)).
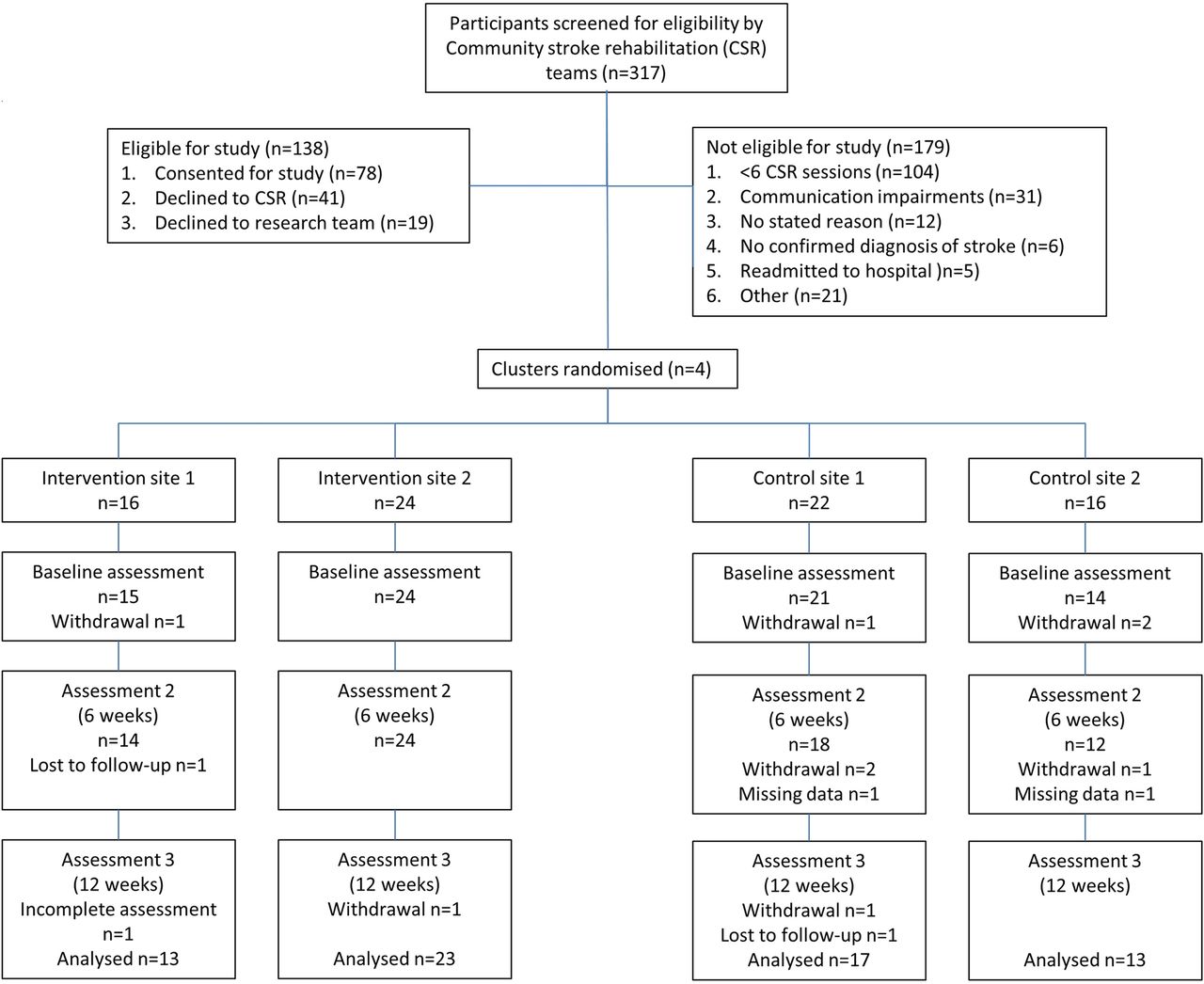
{kind=link}
Study flow diagram.
Randomisation
Participant characteristics
Table 2 shows an even distribution of men and women in intervention sites, but more men took part in the control sites. Days post-stroke data were missing in 8/78 participants. Of note is the wide variation in the length of time since stroke onset. Demographic variables including ethnicity and social circumstances were comparable between intervention and control sites, with the exception of age. Baseline data were complete for 74 (95%) out of 78 participants (95% CI 87% to 99%), with no significant difference between study arms (98% intervention vs 92% control, p=0.35, Fisher's exact test).
Characteristics of study participants
Clinical outcomes
Table 3 shows means and SDs for all outcomes at each time point (baseline, 6 weeks and 12 weeks). Table 3 shows clinical data at 12 weeks completed for 66/78 participants (83%; 95% CI 75% to 92%), and there was no significant difference in outcomes between the arms of the trial for this (p=0.22, Fisher's exact test). The modelling revealed no significant difference between intervention and controls on any outcome that was tested, although the intervention sites showed more consistent improvement in self-efficacy (SSEQ) and functional capacity (NEADL) than did control sites (table 4). If the intervention is aimed at changing self-efficacy and confidence to self-manage, then functional capacity, which measures actual performance, could be a feasible clinical endpoint in a future fully powered trial.
Means and SDs of outcomes at all time points
Outcomes analysis
Sample size calculation for a definitive study
A sample size calculation for a future cluster-randomised controlled trial can be based on the NEADL at 12 weeks with MCIDs suggested as 6.1. The mean (SD) for NEADL was 35.5 (16.86) in the intervention group and 32.1 (19.05) in the control group, and Pearson correlation between baseline and 12-week follow-up NEADL was 0.78. Sites in this study were similar for NEADL apart from one site, which had a lower mean (but this seems to have been driven by just two participants); therefore, we are not able to make a precise estimate of intraclass correlation for future studies, though it appears to be small. If we assume intraclass correlation of zero in the sample size calculation, this effectively uses a calculation for parallel-arms randomised controlled trials, and the MCID for NEADL would require 137 in each arm.34 Assuming a pessimistic completion rate at 12 weeks of 75%, the lower end of the CI from this study's data, this requires consenting 183 participants per arm for NEADL, which implies allocating nine sites per arm for NEADL alone.
Resources and costs of the intervention
Rehabilitation records were available for 73 patients. Total rehabilitation inputs were similar in the two control sites (24 therapy hours per patient). However, a difference was found between the two intervention sites (20.1 vs 50.7 therapy hours). Intervention sites reported a proportionately higher use of therapy assistants than control site (table 5). Costs of patient-facing time ranged from £600 in the low resource use intervention site to £1667 in the high resource use intervention site. The costs of the two control sites were similar (£754 and £763). Total costs for control sites (mean of two sites) ranged from £930 to £1459, depending on the assumptions made about the ratios of patient-facing to patient-related non-face-to-face costs. The equivalent range for the low resource use intervention site was £721–£1103, and for the high resource use intervention site it was £1987–£3012 (table 5).
Resources and costs* used in delivering rehabilitation in the four sites
Patient level use of other health and social services at 6-week and 12-week follow-up were available for 63 of the 73 (88%) participants; the remainder were either lost to follow-up or withdrew. There were relatively few missing data items. The only services used by more than 10% of respondents were GPs, nurses, and hospital outpatient and emergency departments (data not shown); all other services, including social care, were not accessed by more than 90% of participants. Comparisons between sites of total costs of other service utilisation revealed no significant differences between any pair of sites. However, when only stroke-related service use was considered, the other health and social service costs of patients in the low-cost intervention site were higher than in all the other sites (£1291 vs £514 in the high cost intervention site, and £529 and £898 in the two control sites).
Discussion
This is the first study to test the feasibility of conducting a cluster-randomised controlled trial into the effectiveness of a stroke SMP integrated into post-hospital rehabilitation. Overall, the design, using a nested process evaluation, was found to be feasible and the intervention was delivered according to predetermined markers of fidelity.
Recruitment rate at 25% was higher than previous research (18%).24 But patients who required fewer than six sessions were the main reason for exclusion (58%). This is a limitation of this study and our previous research, but was chosen following discussion with CSR teams based on the premise that patients requiring less than six sessions would be less likely to have ongoing rehabilitation needs and would usually be managed by assessment and one-off advice. However, further research to adapt self-management interventions to be delivered in fewer number of sessions while delivering the same impact, such as that developed by Harwood et al, are now warranted.35 Participants with aphasia and other cognitive impairments were also recruited at a lower rate and previous research using provider-based stroke SMPs has included low numbers of people with aphasia.9 Participants were also excluded due to low mood, not engaging in therapy and social issues, and 12 potential participants were excluded with no clear reason other than they were less compliant or more challenging. We suspect there were issues of potential gate keeping and selection of ‘model’ participants for the trials illustrated in another study,36 which highlights the need for training to include methods and practical solutions of extending the SMP to more patients.
Outcomes measuring functional capacity (NEADL) and self-efficacy (SSEQ) showed most sensitivity to change in the intervention compared with control sites. This provides some validation of the aims of Bridges stroke SMP, which uses self-efficacy principles to facilitate a change in functional capacity and self-management. Functional capacity and mood have been shown to be closely associated with self-efficacy post-stroke, but the causal relationship has not been established.11 ,37 However, we suggest a measure of functional capacity such as the NEADL as a primary outcome with secondary measures of mood, quality of life and self-efficacy, is warranted in future self-management trials. At least 18 clusters would be required recruiting 20 participants per site to evaluate effectiveness of this stroke SMP in a full trial.
A number of economic findings were relevant to a full trial. In particular, the resource implications of the intervention appeared very different in the two sites. The composition of teams, particularly the ratio of professional to support staff also require further evaluation. The tool for collecting data on other service use worked well, but the burden on participants might have been reduced by concentrating on services (including GP, nurse, A&E, nurse inpatient) used most frequently, and only on those that were stroke-related. The SF-12 scores were not significantly different between groups, so QALYs were not calculated, although a larger trial may identify differences.
The quality of training given to clinicians in the intervention sites was central to the delivery of the SMP as intended, but was more labour intensive than expected due to high staff turnover. However, compared with recent large-scale trials of provider-based SMPs,38–40 clinicians from the intervention sites engaged in training, and enacted behaviours aligned with predetermined markers of self-management support. Nonetheless, training costs are a major consideration for SMP implementation, and less costly methods of training, such as online resources and peer learning utilising SMP champions, could be employed in a full trial.
Overall, the study was completed with minimal data lost to follow-up, and the trial design could be replicated in a larger definitive trial. By reducing the number of sessions required, addressing accessibility of the workbook and adapting the intervention for people with cognitive impairments, recruitment rates could increase further. Given these recommendations, our results support the need for conducting further research in this area, and provide data to support the design of a definitive trial.
Acknowledgments
The authors acknowledge the input from our stakeholder reference and expert advisory groups; support from the Collaboration for Leadership in Applied Health Research and Care (CLAHRC) South London; Professor Charles Wolfe for his help with early drafts of this paper, and Dr Stefan Tino Kulnik for his help with final drafting.
References
Footnotes
Contributors All the authors designed the study. FJ, RG, HG and ML performed data analysis. FJ and ML wrote the initial draft and all the authors commented on the manuscript.
Funding This report presents independent research funded by the National Institute for Health Research (Research for Patient Benefit Programme; Grant Number: PB-PG-0610–22276).
Disclaimer The views expressed in the publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health. Additional financial support for the study was provided by London (South) Comprehensive Research Network.
Competing interests FJ is the founder and director of the social enterprise Bridges self-management.
Patient consent Obtained.
Ethics approval The London Surrey Borders National Research Ethics Committee gave ethical approval for this study (11/LO/1450), with local Research and Development approval granted from each of the cluster sites.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Request for analyses of de-identified data from this trial should be directed to the corresponding author.