Article Text

Abstract
Objectives This study aims to test the hypothesis that gallstone disease (GSD) is a risk factor for the development of idiopathic sudden sensorineural hearing loss (ISSNHL). Research has shown risks of cardiovascular and cerebrovascular events in patients with GSD; however, well-conducted English studies on the association between GSD and the development of ISSNHL are lacking.
Design and setting Retrospective cohort study using the Taiwan Longitudinal Health Insurance Database.
Participants We compared 26 449 patients diagnosed with GSD between 1 January 2001 and 31 December 2007, with 52 898 age-matched, gender-matched and comorbidities propensity scores-matched controls.
Outcome measured We followed each patient until the end of 2011 and evaluated the incidence of ISSNHL for at least 4 years after the initial GSD diagnosis.
Results The incidence of ISSNHL was 1.42 times higher in the GS cohort than in the non-GS cohort (9.27 vs 6.52/10 000 person-years). Using Cox proportional hazard regressions, the adjusted HR was 1.44 (95% CI 1.19 to 1.74). In the cohort of patients with GSD who needed a cholecystectomy, 37 patients suffered from ISSNHL. Among those patients, 31 (83.7%) patients sustained ISSNHL before cholecystectomy and 6 (16.2%) patients sustained ISSNHL after cholecystectomy.
Conclusions A diagnosis of GSD may be an independent risk for ISSNHL. This finding suggests that an underlying vascular and inflammatory mechanism may contribute to the development of ISSNHL. Physicians may want to counsel patients with GSD to seek medical attention if they have hearing impairments, because patients may be at an increased risk of developing ISSNHL.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The present study, with the strength of its large sample size, shows that patients with gallstone disease (GSD)[+]have a greater risk of developing idiopathic sudden sensorineural hearing loss (ISSNHL) than do patients with GSD[−]. The large nationwide insurance claims data set allowed us to examine the risk factors for developing ISSNHL with a low chance of selection bias. The large sample size increased our statistical power, as well as the precision of our risk appraisal.
This study has some limitations. First, several suspected risk factors for ISSNHL were not available from the National Health Insurance Research Database (NHIRD); for example, patient body mass indexes and personal histories of smoking might have caused some bias.
Second, the database did not include information about the severity of hearing loss or other laboratory test results related to nutrition status.
Introduction
Gallstones are a common condition reported to affect 10–15% of white adults in developed countries.1 In the USA, ethnic differences abound: gallstones are highly prevalent in American Indians but less frequent in black Americans and in East Asian Americans. The overall prevalence of gallstone disease (GSD), cholelithiasis (the production of gallstones), is 5.0% for the adult population in Taiwan.2 High prevalence of GSD in the USA has led to 325 000 hospitalisations in 2005.3 In the UK, approximately 5.5 million people have gallstones and over 50 000 cholecystectomies are performed each year.4 Metabolic syndrome, including comorbid cardiovascular diseases and diabetes, is thought to be a strong risk factor for GSD.5–7 Furthermore, this higher risk has been attributed to the presence of lithogenic bile, which is a consequence of the excessive synthesis of cholesterol.8 ,9
Idiopathic sudden sensorineural hearing loss (ISSNHL) is often a surprising and disquieting experience for patients. Various conditions may precipitate ISSNHL, including vascular disorders, viral infections, autoimmune disorders, neurological disorders, neoplasms and ototoxic drugs. Several studies10–14 have discussed the presence of risk factors for metabolic syndrome in patients with ISSNHL. Among the cardiovascular risk factors, hypercholesterolaemia (Hch) is one of the most widely known.15 ,16 In one nationwide cohort study,17 Hch was associated with a greater risk of ISSNHL. The fact that GSD and ISSNHL are associated with metabolic syndrome prompted us to examine the potential biological linkage between GSD and ISSNHL. If such a relationship exists, it would add evidence to the theory that an underlying vascular and inflammatory mechanism contributes to the development of ISSNHL.
Methods
Data sources
Taiwan launched a universal compulsory national health insurance programme in March 1995. It covers 99% of the country's 23.3 million people.18 Our data are from the National Health Insurance Research Database (NHIRD), which contains all the claims information from 1996 to 2011, from past and present beneficiaries, one million of which had been randomly selected by the Bureau of National Health Insurance (BNHI) for a nationally representative research database with no significant differences in age, gender or healthcare costs between the sample cohort and the other enrollees. The database contains encrypted patient identification numbers, ICD-9-CM (International Classification of Diseases, Ninth Revision, Clinical Modification) codes for diagnoses and procedures, prescription drug details, dates of admission and discharge, and basic sociodemographic information, including gender and birth date. Since the BNHI is the sole payer in Taiwan, the BNHI data set was assumedly the most comprehensive and reliable data source for the study. The BNHI registry database also contains contracted medical facilities and board-certified physicians as well as monthly summaries for all inpatient claims.
Study design
This historical prospective cohort study enrolled a GSD[+] cohort (patients with GSD) and a matched GSD[−] cohort (patients without GSD). We employed a study method that was applied in our previous works.17 ,19 We identified potential cases at risk for GSD and ISSNHL. The database between 1996 and 2000 was used to ensure that the included patients had not contracted GSD or ISSNHL before 2001. In this study, we defined GSD as the presence of stones in the gallbladder (cholelithiasis) or in the ducts (choledolithiasis). Information that identified patients with GSD (ICD-9 code 574.0–574.9) and ISSNHL (ICD-9 code 388.2) was based on a minimum of three hospital visits and a corresponding diagnosis provided by referral teaching hospitals and tertiary referral medical centres. The GSD[+] cohort was composed of patients with a first-time diagnosis of GSD. The GSD[−] (comparison) cohort comprised patients without an ISSNHL-related medical claim, but matched for gender, age, index date, and one or more comorbidities (hypertension (HTN), diabetes mellitus (DM) or Hch). Propensity-score matching, which can bundle many confounding covariates that may be present in an observational study with this number of variables, was used to reduce any selection bias in our hypothesis.20 Score-matching identified the predicted probability of obtaining one patient with GSD[+]versus one patient with GSD[−]from the logistic regression model using the baseline covariates of age, gender and the comorbidities of DM, HTN and Hch. The index date for the patients in the GSD[+] cohort was defined as the date of their first instance of GSD. The index date for the GSD[−] cohort was defined by matching the year of the index date to the GSD[+] cohort. Other comorbidities presented before the index date were DM (ICD-9 code 250), HTN (ICD-9 code 401–405) and Hch (ICD-9 code 272.0–272.1). Patients with comorbidities of HTN, DM and Hch before the index date were defined as having metabolic syndrome. A routine peer review is carried out within the Taiwan Health Insurance Bureau to maintain consistency in medical diagnoses in every referral teaching hospital and tertiary referral medical centre. Despite the study being retrospective, the data were analysed to project possible future outcomes. Patients in both cohorts were assessed to determine the incidence of ISSNHL (ICD-9 code 388.2) until the end of 2011 or until the patient died. According to the regulations, enrolment of NHI is mandatory for the whole population, and enrolment must be withdrawn within 30 days after decease. We determined the vital status via an indirect way because the National Death Registry was not available for our study. Participants who withdrew the NHI enrollment within 30 days after discharge from the last hospitalisation were presumed dead. The discharge dates of those who withdrew were assigned as the dates of death. The identification numbers of all individuals in the NHIRD are encrypted for confidentiality. The study was approved by the Institutional Review Boards of Chi Mei Medical Center and Taipei Medical University.
Statistical analysis
Descriptive statistical analyses with Pearson χ2 tests were used to compare differences in sociodemographic characteristics and comorbidities between the GSD[+] and GSD[−] cohorts. The incidence rate was calculated as the number of ISSNHL incidents identified during patient follow-up divided by the total number of person-years for each cohort by gender, age and years of follow-up. The risk of developing ISSNHL was compared between the cohorts by using Poisson regression to estimate the incidence rate ratio. Cox proportional hazard models were used to assess the risks for developing ISSNHL in association with the comorbidities of DM, HTN and Hch. Cox proportional hazard regression analyses and Kaplan-Meier analyses were used to determine the cumulative incidence rates of ISSNHL in the two cohorts. A log-rank test was used to analyse differences in the survival curves between the two cohorts. To meet the proportional hazards assumption, each dichotomous variable in the model was tested for proportionality using investigative, diagnostic log-log survival plots. SAS 9.2 for Windows (SAS Institute, Cary, North Carolina, USA) was used for all analyses. Significance was set at p<0.05 (two tailed).
Results
Incidence of ISSNHL by patient characteristics
We enrolled 26 449 patients with GSD[+]and 52 898 age-matched, gender-matched and comorbidities propensity-score matched comparison cohort patients with GSD[−] who met the eligibility criteria for this study (table 1). There were no significant baseline differences in the prevalence of DM, HTN or Hch, nor between the annual incomes or geographic distributions of the cohorts (table 1).
Demographic characteristics and comorbid medical disorders of cohort patients
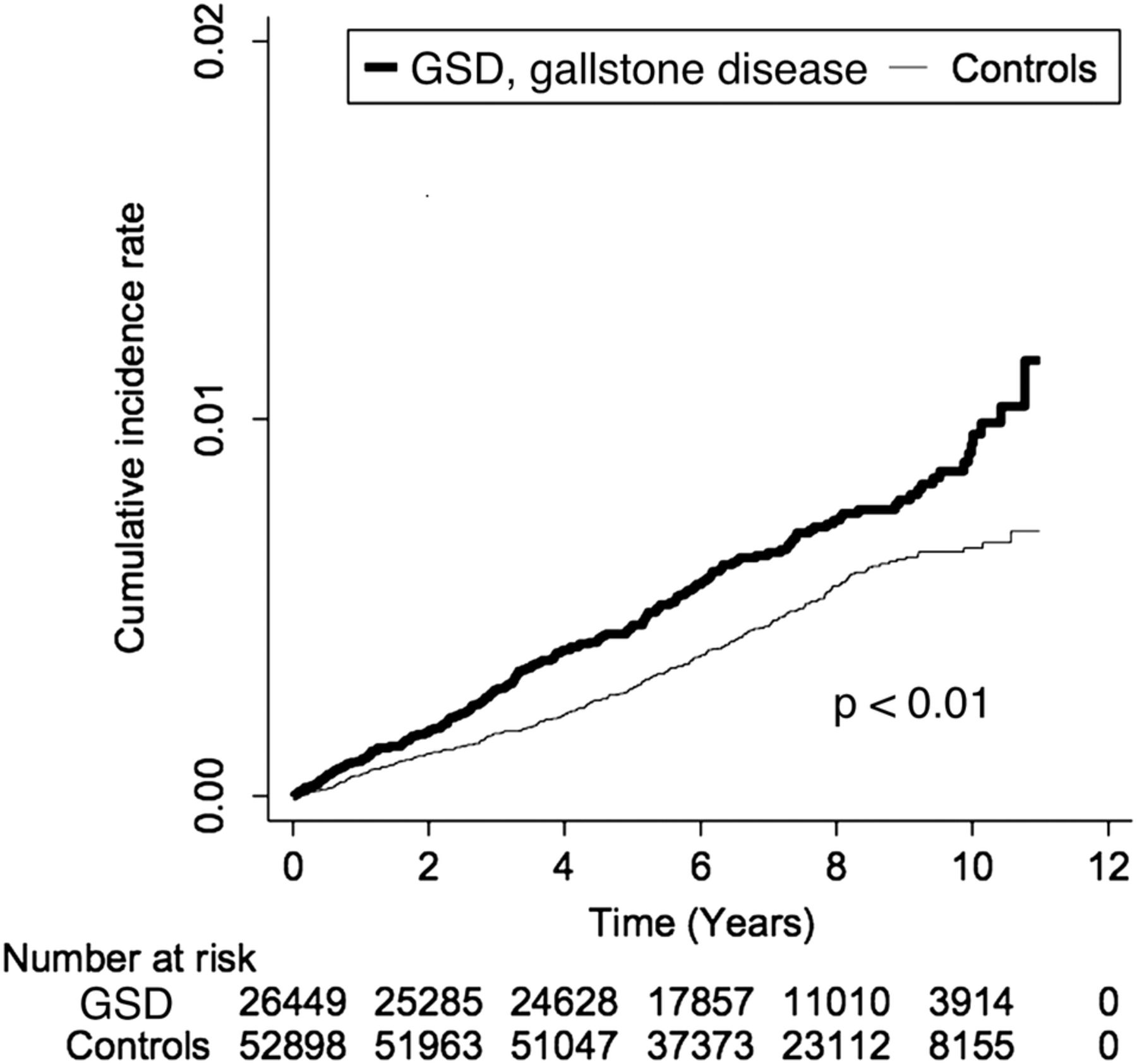
A comparison of differences between the cohorts by gender, age and number of years of follow-up showed that patients with newly diagnosed GSD had an incidence of ISSNHL 1.42 times higher than that of patients with GSD[−] (table 2). By the end of the follow-up period, the incidence of ISSNHL was significantly (p<0.01) higher in the GSD[+] cohort than in the GSD[−] cohort (figure 1). In the GSD[+] cohort, patients aged 50–64 years had the highest incidence (13.97/10 000 person-years) of ISSNHL, but in the GSD[+] cohort, patients aged 35–49 years had a higher incidence rate ratio (IRR=1.67, 95% CI 1.14 to 2.44) than did age-matched patients in the GSD[−] cohort (table 2). The ISSNHL incidence was also significantly different in male patients (p<0.01) with follow-up durations of 1–3 years (p<0.01) in the two cohorts (table 2).
Risk of idiopathic sudden sensorineural hearing loss for cohort patients
{kind=link}
The cumulative incidence rates of idiopathic sudden sensorineural hearing loss (ISSNHL) in Taiwanese patients with (GSD[+]) and without (GSD[−]) gallstone disease (GSD) (2000–2011).
A stratified analysis of the follow-up period showed that the highest incidence of ISSNHL was after 5 years, and that the IRR was highest between the second and third years (IRR=1.76, 95% CI 1.20 to 2.59) in patients with GSD[+].
ISSNHL was associated with comorbidities
Owing to the differential effect of GSD stratified for some of these matching variables, the matching had to be retained in the analyses. A multivariate Cox proportional hazards regression analysis of both cohorts, stratified for gender, age and potential confounding comorbidities, showed an adjusted HR (AHR) of 1.44 (95% CI 1.19 to 1.74) for ISSNHL in patients with GSD[+]compared to that in patients with GSD[−] (table 3). Overall, the AHR increased with age: it peaked in patients aged between 50 and 64 years, and then fell in patients ≥65 years. Gender was not a significant risk for ISSNHL (AHR=0.84 (95% CI 0.70 to 1.02) for females, but DM (AHR=1.72; 95% CI 1.32 to 2.24) was an independent risk factor for ISSNHL in both cohorts (table 3). The IRR of the overall study between the GSD[+] cohort and the GSD[−] cohort was 1.62 (p<0.01); however, the IRR was not significantly different for the comorbidity subgroups of DM, HTN and Hch (table 2).
Crude and adjusted HRs of Cox proportional hazard regressions and 95% CIs for the development of idiopathic sudden sensorineural hearing loss for study cohorts
The incidence of metabolic syndrome was not significantly different between the GSD[+] cohort and the GSD[−] cohort (1.38 vs 1.42, p=0.64). In the GSD[+] cohort, there was no significant difference between patients with ISSNHL and those without ISSNHL for the incidence of metabolic syndrome (2.27 vs 1.37, p=0.74) (table 4).
Prevalence of metabolic syndrome in study cohorts
Severity of GSD relative to the risk of developing ISSNHL
The incidence of developing ISSNHL for patients with GSD[+]who did not need a cholecystectomy was 8.99/10 000 person-years, and it was higher—10.55/10 000 person-years—for the patients with GSD[+]who did need one. In the cohort of patients with GSD[+]who needed a cholecystectomy, 37 suffered from ISSNHL. Among those patients, 31 (83.7%) sustained ISSNHL before cholecystectomy and 6 (16.2%) sustained ISSNHL after cholecystectomy. However, the risks of developing ISSNHL were not significantly different between patients with GSD[+]who needed a cholecystectomy (AHR=1.52, 95% CI 1.08 to 2.15) and patients with GSD[+]who did not (AHR=1.42, 95% CI 1.15 to 1.74) (table 5).
Cox proportional hazard regressions and 95% CIs of sudden hearing loss associated with surgery of newly diagnosed comorbidities for patients with gallstones
Discussion
This is, to the best of our knowledge, the first nationwide cohort study that examines the risk of ISSNHL in patients with GSD. Rather than analysing the association between the risk factors of metabolic syndrome and ISSNHL, as many other studies have done, our study directly assessed the incidence of subsequent ISSNHL in patients diagnosed with GSD.
It is important to know that in patients with GSD who later developed ISSNHL, 13.6% of the ISSNHL events occurred within the first year after a GSD diagnosis, 27.3% occurred between 1 and 3 years, 23.3% occurred between 3–5 years, and 35.8% occurred more than 5 years after the diagnosis: more than 85% of the ISSNHL events occurred more than 1 year after the Hch diagnosis. This finding suggests that constant efforts to detect ISSNHL should not be ignored, even a year after the initial Hch diagnosis.
Income differences may lead to different dietary habits and then to different risk factors for developing metabolic syndrome. Therefore, the monthly incomes differences were matched for the GSD[+] and GSD[−] cohorts in our study. The geographic distribution of the residences of the patients maybe also be associated with different cultures, lifestyles and dietary habits, all of which may be related to the risk of metabolic syndrome. Thus, the geographic location of the residence of the patients was included in propensity-score matching for our cohorts.
Higher risk of ISSNHL in patients with GSD[+]with comorbid DM
An association between a history of HTN and ISSNHL has consistently been reported.21 ,22 We previously reported12 that the incidence of acute myocardial infarction increased significantly in patients with ISSNHL, especially for those with a history of HTN. Microangiopathy is one of the suggested mechanisms for the development of ISSNHL. Nevertheless, we found that HTN was not an independent risk factor for developing ISSNHL, and that the risk for developing ISSNHL was not significantly higher in the HTN subgroup. This finding could indicate that the association between GSD and ISSNHL is not attributable to comorbid HTN.
The biological link between metabolic syndrome and GSD has been attributed noticeably to Hch.23 ,24 cholic acid,9 the pronucleating proteins of IgM,25 and T-cell function26 have been presumed to be critical in the development of Hch; and gallstones have also been reported. Moreover, Hch, a common cardiovascular risk factor, might be associated with ISSNHL.13 ,17 Hch alone can induce profound oedema in the strial marginal layer, and slight oedema in the outer hair cells, primarily in the basal turn of the cochlea, which will cause chronic auditory dysfunction if dietary cholesterol levels remain high for a long time.27 It is therefore reasonable to expect comorbid Hch to contribute to the incidence of ISSNHL. Consequently, we matched the prevalence of comorbid Hch between the GSD[+] and GSD[−] cohorts. There was no significant difference in the incidence rate of ISSNHL between these two cohorts.
Other studies14 ,21 ,28 ,29 have claimed that comorbid DM was an independent risk factor for developing ISSNHL. For example, Aimoni et al21 reported that the prevalence of diabetes was significantly higher in the SSNHL group (15.6%) than in controls (8.5%, p=0.03).21 Lin et al14 found a significantly higher risk of ISSNHL in the DM[+] group than in the DM[−]group (1.29 vs 0.78/1000 person-years, p<0.01). Several studies30–32 have reported a consistent association between microangiopathy and SSNHL. Human temporal bone studies have consistently reported that cochlear microangiopathy occurs in diabetes.33 Consistent with the above literature, we found that comorbid DM was an independent risk factor for the development of ISSNHL in our cohorts. However, in the subgroup with comorbid DM, there was no significant difference in the IRR for developing ISSNHL between patients with GSD[+] and patients with GSD[−]. Therefore, we cannot attribute the higher risk of ISSNHL in patients with GSD[+]to comorbid DM in this study.
The possible confounders of HTN and DM were matched in this study. In addition, we found a dilution effect in the IRR between the Hch[+] cohort and the Hch[−] cohort in the subgroups with comorbid DM and HTN. Chronic kidney disease (CKD), coronary artery disease (CAD) and stroke, however, were not independent risk factors for developing ISSNHL. The comorbidity subgroup analysis yielded corresponding results. Therefore, in this study, the underlying mechanism connecting Hch and ISSNHL cannot be attributed to HTN-associated, DM-associated, CKD-associated, CAD-associated or stroke-associated mechanisms.
The underlying mechanism of ISSNHL in patients with GSD[+]
The mechanism underlying the association between GSD and the subsequent development of ISSNHL remains unclear. Although the aetiology of SSNHL in the majority of patients remains idiopathic, multiple causes have been identified: viral infection, vascular impairment, autoimmune disease, inner ear pathology and central nervous system anomalies. Several studies have claimed a higher risk of ISSNHL in patients with some of the conditions of metabolic syndrome, namely DM,14 HTN12 and Hch.15 ,17 ISSNHL has also been attributed to a persistent inflammation secondary to chronic infections and autoimmune diseases.34 ,35
GSD is thought to have a complex aetiology as well. The pathophysiology of GSD in humans has been attributed to a defective conversion of cholesterol to bile acids, a large flux of cholesterol, decreases in the circulation of bile acids due to a low caloric intake for body weight control, and a low volume of biliary secretion.24 The immune system is also important in the development of gallstones. For example, IgM and possibly IgA are presumed to be the pronucleating proteins of cholesterol crystals.25 ,36 ,37 Both in mouse and human studies, gallstones form because of inflammation, defective gallbladder contractility and impaired gallbladder epithelium transport.23 ,24 ,36 ,38
Both GSD and ISSNHL can be attributed to persistent inflammation. A systemic inflammation itself may be the trigger for the pathological activation of nuclear factor-κB and aberrant cellular stress pathways within the cochlea that result in ISSNHL.39 ,40 Thus, we speculate that GSD may contribute to the risk of ISSNHL because it activates the immune system and possibly the subsequent inflammatory pathways.
Microvascular conditions are another possible mechanism of the association between GSD and ISSNHL. Most other studies7 ,41 ,42 have reported higher risks of cardiovascular diseases in patients with GSD[+]. Likewise, a vascular compromise is thought to be one of the major causes of ISSNHL.10 ,12 ,21 The inner ear is specifically sensitive to transient ischaemia because of its high metabolic requirements and lack of collateral blood supply.43–45 Other studies10 ,11 ,46 have also reported that impaired cochlear blood perfusion and microvascular damage are important aetiopathogenetic events in the development of ISSNHL.10 ,11 ,46 Given that there is a biological linkage between GSD and ISSNHL, we hypothesise an underlying vascular mechanism in the development of ISSNHL.
This study, with the strength of its large sample size, shows that patients with GSD[+]have a greater risk of developing ISSNHL than do patients with GSD[−]. The large nationwide insurance claims data set allowed us to examine the risk factors for developing ISSNHL with a low chance of selection bias. The large sample size increased our statistical power, as well as the precision of our risk appraisal.18
Knowledge about a patient's elevated risk for developing ISSNHL after a diagnosis of GSD could prompt early detection and treatment of ISSNHL. In addition, particular emphasis could be placed on preventing ISSNHL in patients with GSD who underwent surgery for GSD. With early detection and timely treatment, the prognosis of ISSNHL is often promising.47–49
Our study has some limitations. First, several suspected risk factors for ISSNHL were not available from the NHIRD; for example, patient body mass indexes and personal histories of smoking might have caused some bias. Second, the database did not include information about the severity of hearing loss or other laboratory test results related to nutrition status. Other chronic inflammatory conditions have not been completely excluded in this claim data analysis. Although patients in the GSD[−] cohort had never been diagnosed with GSD, not all of them had been examined for GSD. Misclassifying patients with undiagnosed GSD as GSD[−] will bias the results towards the null. Regarding the effect of comorbid Hch, not all of the enrolled patients had been examined for the cholesterol level. However, by using a large national sample, we can dilute the effect of patients with comorbid Hch who are included in the Hch[−] group because they did not have a mandatory cholesterol test. Third, it is possible that patients with GSD will frequently visit physicians and thus have their hearing changes easily detected. The effect of this limitation might be minimal in Taiwan. This is because of the easy access to adequate medical care provided by Taiwan's national health insurance system; patients with GSD[−]ISSNHL[+] also have a good chance of being diagnosed with ISSNHL.
Conclusion
We found that Taiwanese patients with GSD[+] had a higher risk of developing ISSNHL than did patients with matched GSD[−]. This finding adds evidence to the hypothesis that inflammation and underlying vascular mechanism are risk factors for developing ISSNHL. Physicians may want to counsel patients with GSD[+]to seek medical attention if they experience hearing impairments.
References
Footnotes
Contributors Y-SL had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Y-SL and C-CC were involved in the study concept and design. Y-SL was involved in the drafting of the manuscript. S-FW and C-CC were involved in the statistical analysis. C-CC and Y-SL were involved in the administrative, technical and material support. Y-SL was involved in the study supervision.
Funding Chi Mei Medical Center Research Fund, CMH 10404-E06.
Competing interests None declared.
Ethics approval Chi Mei Medical Center IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.