Article Text

Abstract
Objectives The incidence of non-alcoholic fatty liver disease (NAFLD) is significant in hepatitis C virus (HCV) carriers due to multiple mechanisms, and this worsens the progression of chronic liver diseases, such as cirrhosis and hepatocellular carcinoma, and death. The purpose of this study was to examine whether the alanine aminotransferase/aspartate aminotransferase (ALT/AST) ratio correlates with the status of hepatosteatosis.
Design A cross-sectional observational study.
Setting Community-based annual examination in northern Taiwan.
Participants A total of 1354 participants (age 20 years or over) were enrolled after excluding participants with HCV seronegative, laboratory or questionnaires loss, moderate alcohol consumption, liver cirrhosis, tumours and postlobectomy.
Outcome measures Fatty liver was diagnosed according to echogenic findings. NAFLD included grades 1–3 fatty liver and high-degree NAFLD defined grades 2–3 fatty liver.
Results 580 males and 774 females with a mean age of 47.2 (SD=16.1) years were cross-sectionally studied. The participants with NAFLD have significantly higher levels of ALT/AST ratio, fasting glucose, triglyceride and systolic/diastolic blood pressure than non-NAFLD participants. The association between NAFLD and ALT/AST was significant even when adjusting for the metabolic syndrome (aOR 1.90; 95% CI 1.37 to 2.65; p<0.001). In patients with a high degree of NAFLD, the ALT/AST ratio was still a significant predictor for hepatosteatosis (aOR 2.44; 95% CI 1.58 to 3.77; p<0.001).
Conclusions The ALT/AST ratio could be a strong risk of hepatosteatosis in patients with chronic HCV infection.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to reveal a strong relationship between the alanine aminotransferase/aspartate aminotransferase ratio and hepatosteatosis in patients with non-genotype 3 hepatitis C virus.
This test could be easy to perform during regular health examinations, and a higher ratio may be strongly associated with significant steatosis.
Cofactors, including metabolic syndrome (MetS) and hyperuricaemia, are also present in high-degree NAFLD, and therefore we emphasise the impact of the alanine aminotransferase/aspartate aminotransferase (ALT/AST) ratio on systemic and hepatic inflammatory pathogenesis in patients with chronic hepatitis C virus (HCV) infection and steatosis.
Introduction
HCV infection is one of the most serious health issues in the world, with an estimated global prevalence of around 2.8–3.0% (180 million patients).1 Southern Taiwan is an HCV hyperendemic area with a high prevalence of up to 57.9%.2 Most deaths are associated with viral hepatitis-related complications such as cirrhosis or hepatocellular carcinoma (HCC); however, residual mortality is due to cardiovascular death associated with extrahepatic issues.3
The possible mechanism for HCV-related cardiovascular death may be due to insulin resistance and systemic atherosclerosis. Patients with hepatitis C have been reported to have significantly higher levels of insulin resistance compared with uninfected controls and a higher incidence of diabetes,4 even compared with hepatitis B virus (HBV)-infected controls.5 Hepatocyte steatosis, defined as the accumulation of fat droplets and an increased level of intrahepatic triglycerides (TGs) in hepatocytes, is the main cause of insulin resistance.6 Associated aetiologies include both metabolic disorders and alcohol consumption, and also chronic hepatitis C and drug-induced liver disease.7 Non-alcoholic fatty liver disease (NAFLD) has been reported to contribute to insulin resistance,8 type 2 diabetes9 and further cardiovascular events.10 The prevalence of NAFLD was estimated to be between 20% and 30% in the general population.11 Moreover, those HCV participants had a higher prevalence of NAFLD of around 30–50% with incidence of steatohepatitis of up to 10%.12
NAFLD is a critical problem as it can progress to severe liver disease, including hepatosteatosis, fibrosis,13 hepatocellular cancer14 and a lower likelihood of achieving sustained virological response after antiviral therapy for HCV.15 However, most cases of NAFLD are discovered incidentally, and the majority of NAFLD cases ‘silently’ coexist with asymptomatic hepatitis C. γ-Glutamyl transferase (GGT), ALT and AST are liver injury-related markers and they may fluctuate in participants with NAFLD.16 The AST/ALT ratio is a marker of liver cirrhosis17 and advanced alcoholic liver disease.18 In addition, a reverse AST/ALT ratio is also a surrogate marker for insulin resistance19 and silent MetS;20 however, the link between ALT/AST ratio and NAFLD has yet to be elucidated.
The purpose of this study was to investigate the value of the ALT/AST ratio as an independent factor for hepatosteatosis in an HCV seropositive population.
Methods
Study participants and design
The study participants were selected from a community-based annual check-up programme in a rural town located in Yunlin County, Taiwan, where there is a high prevalence of hepatitis C infection from December 2012 to September 2013. A total of 12 348 participants who took part in the health examination programme were evaluated. Participants over 20 years of age who were HCV seropositive were included in this study. The exclusion criteria included those with incomplete questionnaires, and those with no data on body weight, waist circumference, body height and blood pressure (BP). In addition, participants without laboratory data on anti-HCV antibodies and hepatitis B surface antigen(HBsAg), those with liver tumours and liver cirrhosis and those who consumed alcohol were also excluded. Finally, a total of 1354 participants were enrolled in the analysis (figure 1).
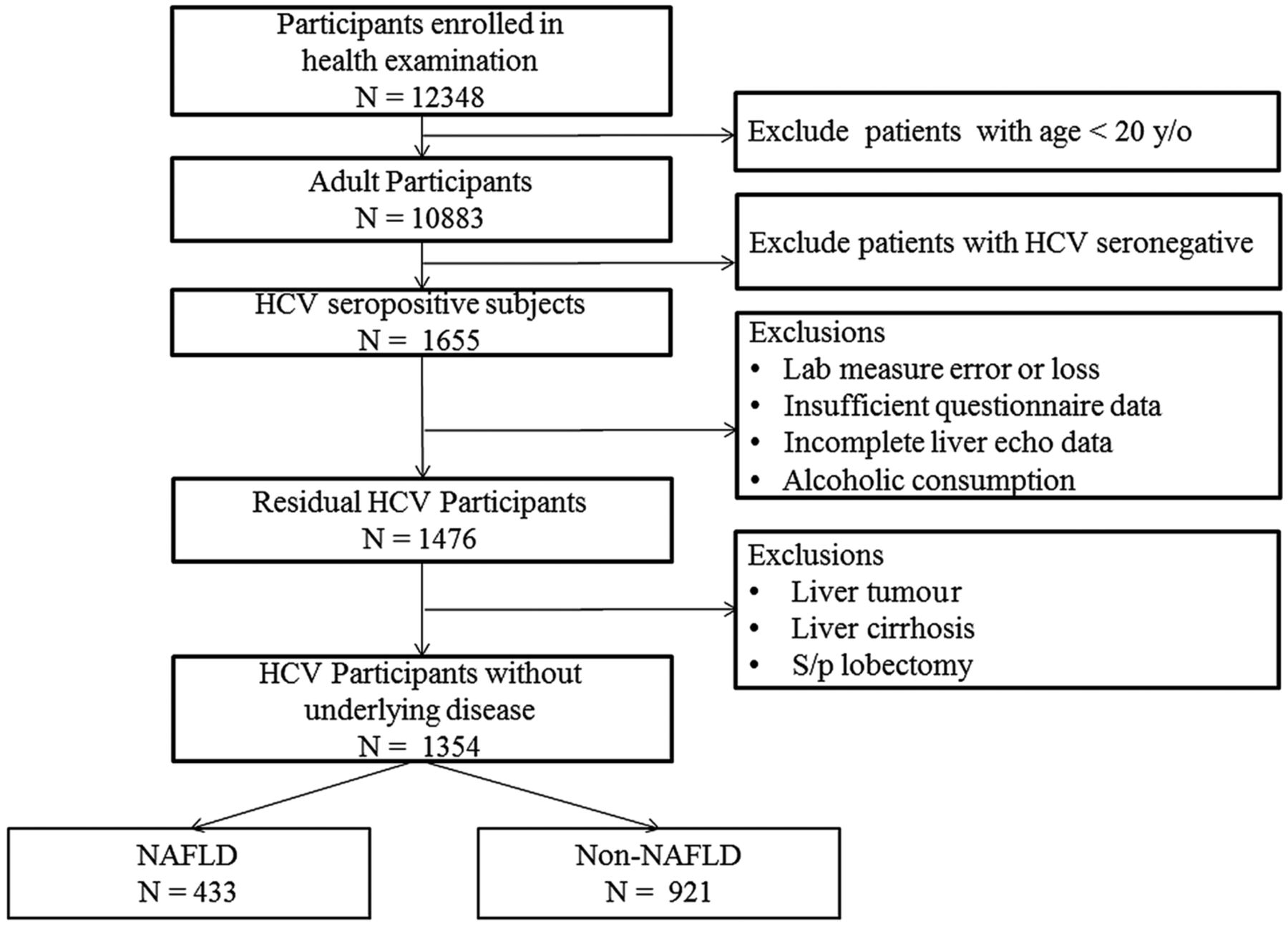
Enrolment flow chart for and participant selection. HCV, hepatitis C virus; NAFLD, non-alcoholic fatty liver disease.
Anthropometric and BP measurements
Waist circumference was measured using a standard meter with an accuracy of 0.5 cm at the midpoint between the lowest rib and the iliac crest, after the patient had exhaled while standing without shoes, with both feet touching, and arms hanging freely. Body weight was measured in kilograms and included clothing but not shoes or heavy accessories. Waist circumference was measured at the bending point and at the narrowest point. Hip circumference was measured at the iliac crest and at the largest point.
BP was measured according to the Hypertension Detection and Follow-up Program protocol using a standard electronic sphygmomanometer after the patient had been sitting comfortably with their back supported for at least 5 min. BP values were reported in millimetres of mercury (mm Hg).
Biochemical measurements and hepatitis virus screening
The serum collected in the morning was measured by the Hitachi 7600 Automatic Biochemical Analyzer to detect fasting sugar, uric acid, creatinine, ALT, AST, serum TGs, total cholesterol, high-density lipoprotein (HDL) cholesterol and low-density lipoprotein (LDL) cholesterol. Seropositivity of antibodies to HCV was assessed using an electrochemiluminescence immunoassay (Elecsys; Cobas Analyzer; Roche Diagnostics Corp), and seropositivity to HBV was assessed according to the semiquantitative determination of HBsAg using a sandwich radioimmunoassay (Elecsys; Cobas analyzer; Roche Diagnostics Corp). Diagnoses of hepatitis B and hepatitis C seropositivity were made if the patients were seropositive for HBsAg and anti-HCV antibodies, respectively.
Medical and personal history check-up
A checklist of the history of baseline diseases and lifestyle habits was completed by each participant and rechecked by the examining interviewers. Diabetes was defined as the presence of type 2 diabetes diagnosed by a physician or the current usage of related medications. Hypertension was defined as physician-diagnosed high BP or the current use of antihypertensive medications. Prescribed and non-prescribed medications used by the participants in the month before their clinic visit were recorded and verified by a nurse. Personal habitual behaviours included alcohol drinking, cigarette smoking and betel nut chewing habits. Participants were classified as ‘non-users’ if they had never drunk alcohol or smoked or chewed betel nut for 1 year, and as ‘current users’ if they were currently drinking or smoking or chewing.
Abdominal echography
Right upper quadrant ultrasound was performed on one of three units: Aloka SSD 4000 (Hitachi Aloka Medical Ltd, Tokyo, Japan) with a UST-979-3.5 curved array transducer; CGM OPUS 5000 (Chang Gung Medical Technology Co, Ltd, Taipei, Taiwan) with a CLA35 curved array transducer; and the Acuson S2000 Ultrasound System (Siemens) using a C4–1 MHz curved array transducer. Examinations were performed by 1 of 10 sonographers with 5–10 years of experience. Technical parameters were adjusted for each patient using the standard protocol for a right upper quadrant ultrasound examination. The liver was considered normal if the echotexture was homogeneous with no acoustic attenuation, the portal veins were visible, the diaphragm was well visualised and echogenicity was similar or slightly higher than that of the renal parenchyma. The diagnosis of fatty liver was based on the brightness of the liver on ultrasound compared with the kidney, vascular blurring of the hepatic vein trunk and deep attenuation in the right hepatic lobe. The severity of fatty liver change was classified according to standardised ultrasonographic criteria: grade 0, normal liver, a normal echotexture and absence of fatty change; grade 1, mild fatty liver change, a mild increase in fine echoes in the parenchyma with slightly impaired visualisation of intrahepatic vessels and diaphragm; grade 2, medium grade diffuse increase in hepatic echogenicity, mild deterioration in the image of the diaphragm and intrahepatic vessels; grade 3, moderate to severe fatty liver change, marked increase in fine echoes in the parenchyma with poor or non-visualisation of the intrahepatic vessel borders, diaphragm and posterior right lobe of the liver. The criteria for ‘severe’ fatty liver change were therefore obvious and unambiguous.21 All images were reviewed on a Centricity PACS system (GE Health-care, Allendale, New Jersey, USA).
Definition of NAFLD
We defined NAFLD as (1) evidence of hepatic steatosis by echogenic imaging, and (2) no causes of secondary hepatic fat accumulation such as significant alcohol consumption, use of steatogenic medication or hereditary disorders. Study I compared the participants with NAFLD (grades 1–3) to those without NAFLD, and study II compared the participants with a high degree of NAFLD (moderate to severe fatty liver, grades 2–3) to those with a low degree of NAFLD (grades 0–1).
Definition of MetS
The criteria used to define the MetS were those of the National Cholesterol Education Program-Adult Treatment Panel-III in 2006, and were defined as the presence of three or more of the following: fasting plasma glucose ≥110 mg/dL (5.6 mmol/L) or the use of medication for hyperglycaemia, serum TGs ≥150 mg/dL, serum HDL-cholesterol <40 in men and <50 mg/dL in women, BP ≥130/85 mm Hg, or waist circumference >102 in men and >88 cm in women. An elevated BP was considered to be ≥130/85 mm Hg or the use of medication for hypertension.
Statistical analysis
The participants were divided into two groups based on whether or not they had fatty liver disease according to echogenic features. Distribution of baseline characteristics between these two groups was compared using χ2 test for categorical variables and using an independent sample t test or Mann-Whitney U test for continuous variables where appropriate. Values of categorical variables were expressed as the number and proportion and those of continuous variables were expressed as mean±SD. However, several variables (including fasting glucose, ALT, AST, GGT and TG) did not follow normal distribution, and therefore the original values were expressed as the median (25th centile, 75th centile) and the values were also log transformed. The independent contribution of variables to hepatosteatosis as NAFLD and a high degree of NAFLD was examined using hierarchical multivariate logistic regression analysis in various adjustment models. All statistical analyses were performed using IBM SPSS Statistics V.19 (SPSS, Inc, Chicago, Illinois, USA).
Results
Study I: Clinical characteristics of the participants with NAFLD
In total, 1354 participants were enrolled with a mean age of 47.2 years (SD=16.1), including 433 with NAFLD and 921 without NAFLD (table 1). There were more females in the NAFLD group, and a higher systolic (138.1±19.9 vs 135.2±20.8 mm Hg; p=0.016) and diastolic (82.2±13.5 vs 80.5±14.8 mm Hg; p=0.034) BP. The prevalence of diabetes and hypertension was higher in the NAFLD group (p=0.001). With regard to laboratory data, the NAFLD group had a higher prevalence of the MetS (37.0% vs 25.8%; p<0.001) with a higher log-transformed fasting glucose level (4.70±0.25 vs 4.65±0.23; p<0.001), log-transformed lower HDL level (mean 49.1±12.2 vs 51.8±13.9 mg/dL; p=0.001) and higher log-transformed TG level (4.72±0.49 vs 4.54±0.46; p<0.001) than the group without NAFLD. Interestingly, the ALT/AST ratio was significantly higher in the NAFLD group (1.2±0.4 vs 1.1±0.4; p<0.001).
Baseline characteristics of the patients with HCV with or without NAFLD
Study II: Clinical characteristics of the participants with a high degree of NAFLD
In the high-degree NAFLD group, there were more females, a higher systolic BP (142.0±17.9 vs 135.2±20.8 mm Hg; p<0.001), diastolic BP (84.4±12.0 vs 80.5±14.6 mm Hg; p=0.001), pulse pressure (57.6±12.9 vs 54.7±13.9 mm Hg; p=0.010), and higher prevalence rates of diabetes and hypertension (p=0.001; table 2). With regard to laboratory data, the high-degree NAFLD group had a higher ALT/AST ratio (1.2±0.4 vs 1.1±0.4; p<0.001). Those participants with a high degree of NAFLD had a significantly higher incidence of MetS (45.8% vs 26.9%; p<0.001) with higher levels of log-transformed fasting glucose (4.73±0.25 vs 4.66±0.23; p<0.001), log-transformed uric acid (6.5±1.7 vs 6.0±1.6 mg/dL; p<0.001), log-transformed TG (4.84±0.51 vs 4.56±0.46; p<0.001) and a lower HDL level (47.0±11.3 vs 51.5±13.6 mg/dL; p<0.001) than those with a low degree of NAFLD. The incidence of NAFLD or high-degree NAFLD was higher in the participants with MetS (40.2% vs 28.6%; p<0.001) and (20.6% vs 10.1%; p<0.001; figure 2). In addition, higher scores of MetS were also significant in high-degree NAFLD (p<0.001; figure 3).
Baseline characteristics of the patients with HCV with or without a high degree of NAFLD

The incidence of non-alcoholic fatty liver disease (NAFLD) and high-degree hepatosteatosis in patients with and without metabolic syndrome (MetS).
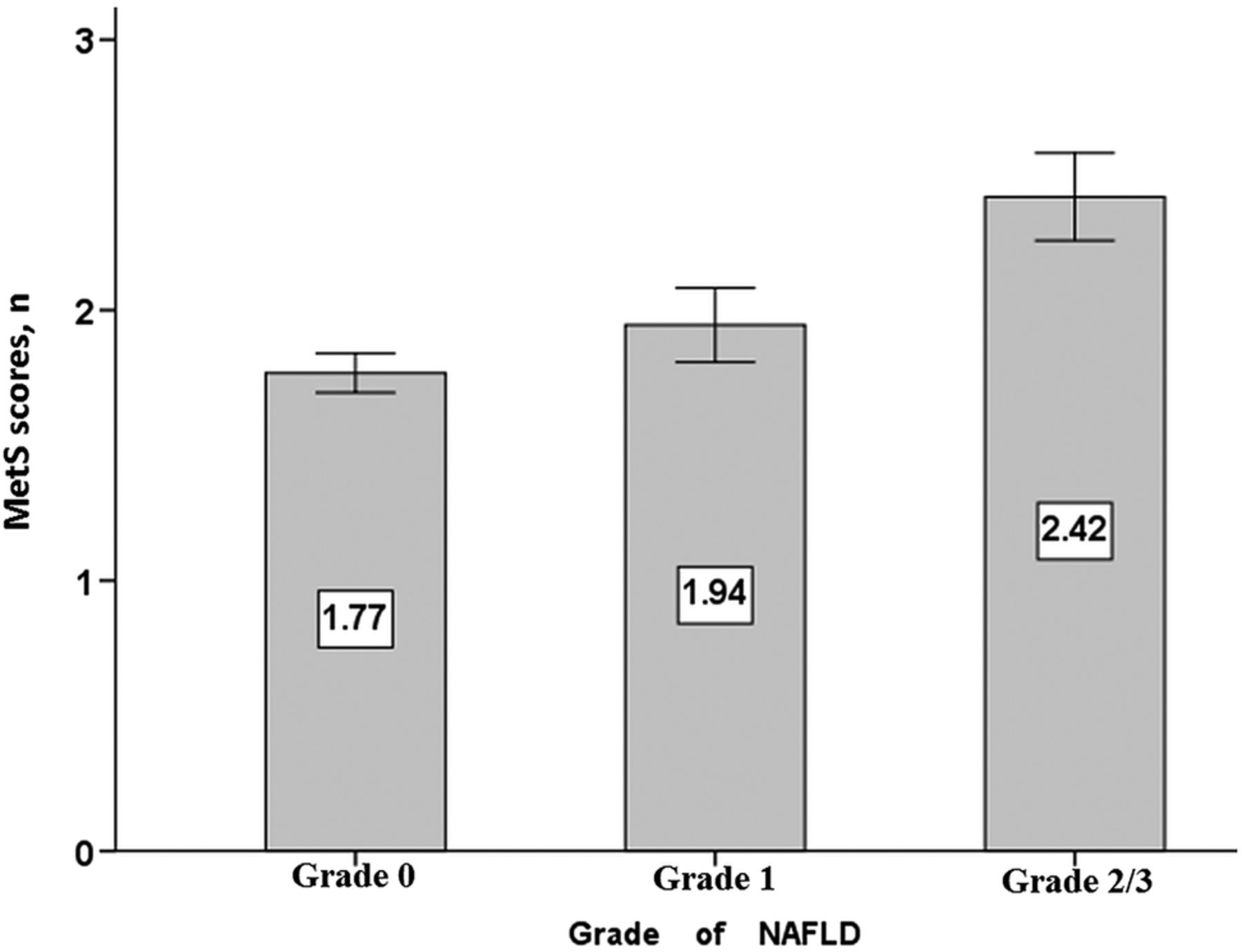
Comparison of metabolic syndrome (MetS) scores was analysed by analysis of variance and expressed as mean and 95% CI. The MetS scores among different grade non-alcoholic fatty liver disease (NAFLD) were significantly different.
Liver enzymes and hepatosteatosis
Finally, all variables were evaluated to predict the risks for NAFLD and significant hepatosteatosis as shown in figure 4. The ALT/AST ratio was significantly independently associated with NAFLD (OR 1.90; 95% CI 1.37 to 2.65; p<0.001) and high-degree NAFLD (OR 2.44; 95% CI 1.58 to 3.77; p<0.001) with adjustments (figure 4A,B). The ALT/AST ratio was still significantly associated with NAFLD (OR 1.77; 95% CI 1.27 to 2.48; p=0.001) and a high degree of NAFLD (OR 1.95; 95% CI 1.25 to 3.04; p=0.003) in hierarchical multivariate regression analysis (table 3).
Association of aminotransferase ratio with fatty liver diagnosis in various adjustment models (hierarchical multiple logistic regression)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Multivariate logistic regression of factors associated with non-alcoholic fatty liver disease (NAFLD). (B) Multivariate logistic regression of factors associated with a high degree of NAFLD. Adjusted for variables including age, gender, body mass index, metabolic syndrome (MetS), waist/hip ratio, alanine aminotransferase/aspartate aminotransferase (ALT/AST) ratio, γ-glutamyl transferase, hepatitis B virus, creatinine, uric acid, cholesterol, low-density lipoprotein, betel nut chewing and smoking.
Discussion
This is the first study to reveal a strong relationship between the ALT/AST ratio and NAFLD in patients with HCV, and the ALT/AST ratio was also an independent risk factor apart from the conventional risk factors for hepatosteatosis including the MetS, LDL, TC, waist/hip ratio and body mass index. The patients with a higher ALT/AST ratio had a 1.9-fold higher risk of NAFLD (95% CI 1.37 to 2.65; p<0.001) and a 2.44-fold higher risk of a high degree of NAFLD (95% CI 1.58 to 3.77; p<0.001).
Steatosis, MetS and HCV triangulation: genotype dependence
In the current study, the prevalence of NAFLD was 31.9%, and 19.6% of the participants had moderate to severe hepatosteatosis. The MetS and insulin resistance were the major risk factors for hepatosteatosis in this study. Such hepatic steatosis is considered to be a hepatic manifestation of the MetS where insulin resistance is the underlying factor, with diabetes mellitus, obesity and hypertriglyceridaemia-prominent clinical sequelae. In this study, the incidence of MetS was 29.4%, and higher prevalence rates of NAFLD and high-degree hepatosteatosis were considered to be contributing factors (figure 2). In addition, those participants with steatosis had more features of MetS, including higher BP, fasting sugar, TG and lower HDL level. The prevalence of hepatosteatosis in chronic hepatitis C infection has been reported of up to 31–72%, which is significantly higher than that in participants with other chronic liver disease such as hepatitis B or autoimmune hepatitis, suggesting a direct effect of HCV replication in the development of excess fat accumulation in the liver.22 ,23 The underestimation of hepatosteatosis in our study may also be related to echogenic limitations including a lower sensitivity and interoperative dependences.
The relationship between chronic hepatitis C and hepatosteatosis has been reported to have a strong genotype dependence, to correlate with viral load, and to disappear in cases of successful genotype 3 therapy.24 Two mechanisms have been reported due to differences in the genotype in hepatosteatosis. First, the viral type of steatosis in HCV-3-infected patients seems to be directly triggered by a virus without any other steatogenic cofactors.25 Genotype 3 is a teratogenic virus, and the severity of hepatic steatosis is related to a high viral load; however, steatosis usually resolves with successful antiviral therapy. The HCV genotype 3 core proteins have viral effects including a decrease in adiponectin level, and changes to hepatic lipid metabolism that lead to TG accumulation. The second is a metabolic type of steatosis that is associated with increased body mass index, obesity, hyperlipidaemia and insulin resistance in non-genotype 3 HCV-infected patients.26 These mechanisms are similar to those of classical NAFLD, and act mainly through insulin resistance. Previous studies have reported that the HOMA (Homeostasis Model Assessment) score is higher in patients with HCV genotypes 1 and 4, and lowest in patients with genotype 3.27 ,28 In Taiwan, the major genotypes of HCV are types 1 and 2, and the MetS with higher metabolic scores was also associated with steatosis in our study. Insulin resistance as noted by a higher fasting glucose level was seen in our participants with NAFLD, and other components of the MetS (hypertension, HDL and TG) were also significant risk factors for the development of hepatosteatosis (table 1).
On the other hand, insulin resistance may be strongly associated with body mass index, hepatic steatosis, tumour necrosis factor-α (TNF-α) and hepatic iron concentration in patients with non-genotype 3 HCV infection.29 It has been estimated that approximately 20% of individuals infected with HCV are obese, and that obesity in these individuals is associated with steatosis and the progression of fibrosis. Eguchi et al30 demonstrated the possible mechanisms that progression of visceral obesity may be related to increasing production of the extracellular matrix and HCV-induced insulin resistance. Those obese HCV participants with diabetes mellitus had poor response to interferon-α therapy and progressive fibrosis of hepatocarcinogenesis contributing to higher incidence of HCC.31 Moreover, insulin resistance was not associated with viral factors but was associated with visceral fat accumulation, which means that host factors may influence insulin resistance more strongly than viral factors.
Inflammatory markers and the impact on steatosis and disease progression
Hepatic inflammation due to fatty liver has been associated with glucose metabolism and the prevalence of diabetes.32 ,33 Non-alcoholic steatohepatitis describes a subtype of NAFLD in which hepatic steatosis is associated with hepatocyte injury (ballooning degeneration, parenchymal inflammation, Mallory bodies and fibrosis). Some patients with non-alcoholic steatohepatitis progress to cirrhosis or end-stage liver disease, and a meta-analysis found that the severity of hepatic steatosis was strongly associated with insulin resistance and hepatic necroinflammation.24
Serum ALT activity has long been used as an inflammatory marker to assess liver injury related to multiple aetiologies including hepatitis, tumours, liver cirrhosis and alcohol consumption. We excluded patients who consumed alcohol and those with major hepatic lesions including tumours and liver cirrhosis in this study. In addition, general parameters including ALT, AST, GGT, ALP and uric acid were included in this study to evaluate inflammation. Many reports have also shown that serum ALT activity is higher in males than in females; however, this effect may have been reduced due to the female predominance of our study participants with steatosis.
Insulin resistance and improper transports of fat have all been implicated in the progression of NAFLD, which may be fuelled by further inflammation and oxidative stress. As previously discussed, HCV core proteins also promote insulin resistance and hepatic steatosis by inducing oxidative stress via elevation of proinflammatory cytokines such as TNF-α, upregulation of SOCS-3, activation of Kupffer cells and increasing levels of reactive oxygen species, resulting in further inhibition of very-LDL secretion. On the other hand, hyperinsulinaemia and a chronic inflammatory state contribute synergistically to the severity and progression of liver damage. Therefore, it seems that metabolic factors enhance the liver damage caused by immunological reactions to HCV.
ALT and GGT are independent markers of the activation of systemic inflammation and increased oxidative stress, independent of their relationship to the MetS, and the presence of the MetS and elevations of both of these liver enzymes may additively worsen the atherogenic state.34 ,35 In this study, we found that a higher serum ALT/AST ratio in the HCV-infected patients was strongly associated with hepatic inflammation, in addition to showing an association with MetS. Thus, serum ALT/AST is better than serum AST or GGT in reflecting liver fat accumulation in adults. A higher ALT/AST ratio implies more advanced inflammation due to insulin resistance, steatohepatitis and HCV viral replication. On the other hand, chronic inflammatory processes in HCV infection reflect higher insulin resistance, hepatosteatosis with hepatitis, advance viral hepatitis and systemic atherosclerosis, resulting in an increased risk of cardiovascular disease in the general population.36 In this study, we also found that a higher uric acid level was associated with a high degree of steatosis, suggesting that a complex of metabolic and inflammatory processes may be involved in hepatosteatosis. Therefore, a higher ALT/AST ratio may also be a significant marker for systemic inflammatory diseases other than hepatosteatosis.
Study limitations
There are several important limitations to this study. First, confirmatory HCV testing such as HCV RNA, HCV core antigen or biopsy was not performed, and HCV antibodies assay to define HCV seropositivity may have resulted in a less accurate characterisation of whether the participants were carriers and corrected false-positive results. Second, liver biopsy remains the gold standard for NAFLD; however, this procedure is costly, and has operational complexity in terms of the potential adverse effects of bleeding or death. Furthermore, utilisation of liver biopsies in population-based studies is infeasible. Imaging by CT and MR can detect liver fat; however, these techniques cannot differentiate simple steatosis from non-alcoholic steatohepatitis. Third, based on the cross-sectional study design, the present findings are inherently limited in the ability to eliminate causal relationships between the ALT/AST ratio and NAFLD. The coefficients of variability are unavailable due to the unrepeatable check-up in the annular health examination. Fourth, since some of the study population had several risk factors, including hypertension and dyslipidaemia, we could not eliminate the possible effect of underlying diseases on the present findings. Further prospective population-based studies are needed to investigate the mechanisms in order to answer these questions.
Conclusion
Despite some limitations, this study demonstrated that the ALT/AST ratio is associated with fatty liver in patients with HCV, especially for those without genotype 3. To the best of our knowledge, this is the first study to show that hepatic inflammation, as measured by the serum aminotransferase ratio, and metabolic factors are associated with hepatosteatosis in patients with chronic hepatitis C infection. The ability to identify individuals with hepatosteatosis may help healthcare professionals to implement lifestyle interventions.
References
Footnotes
Contributors MSL, HSL, CMC, YSL, MYC and TJH were involved in the study concept and design. PHC, JCH and WNC were involved in the field study and data acquisition. MSL, HSL, PHC, JCH and WNC were involved in the analysis and interpretation of the data. MSL was involved in the drafting of the manuscript. MYC, CMC and TJH were involved in the critical revision of the manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethical approval was given by the university and hospital ethics review board (IRB number: 103-6854B).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.