Article Text

Abstract
Objectives To assess geographic and socioeconomic gradients in sodium and potassium intake in Italy.
Setting Cross-sectional survey in Italy.
Participants 3857 men and women, aged 39–79 years, randomly sampled in 20 regions (as part of a National cardiovascular survey of 8714 men and women).
Primary outcome measures Participants’ dietary sodium and potassium intakes were measured by 24 h urinary sodium and potassium excretions. 2 indicators measured socioeconomic status: education and occupation. Bayesian geoadditive models were used to assess spatial and socioeconomic patterns of sodium and potassium intakes accounting for sociodemographic, anthropometric and behavioural confounders.
Results There was a significant north-south pattern of sodium excretion in Italy. Participants living in southern Italy (eg, Calabria, Basilicata and Puglia >180 mmol/24 h) had a significantly higher sodium excretion than elsewhere (eg, Val d'Aosta and Trentino-Alto Adige <140 mmol/24 h; p<0.001). There was a linear association between occupation and sodium excretion (p<0.001). When compared with occupation I (top managerial), occupations III and IV had a 6.5% higher sodium excretion (coefficients: 0.054 (90% credible levels 0.014, 0.093) and 0.064 (0.024, 0.104), respectively). A similar relationship was found between educational attainment and sodium excretion (p<0.0001). When compared with those with a university degree, participants with primary and junior school education had a 5.9% higher urinary sodium (coefficients: 0.074 (0.031, 0.116) and 0.038 (0.001, 0.075), respectively). The socioeconomic gradient explained the spatial variation. Potassium excretion was higher in central regions and in some southern regions. Those in occupation V (low-skill workers) showed a 3% lower potassium excretion compared with those in occupation I. However, the socioeconomic gradient only partially explained the spatial variation.
Conclusions Salt intake in Italy is significantly higher in less advantaged social groups. This gradient is independent of confounders and explains the geographical variation.
- EPIDEMIOLOGY
- NUTRITION & DIETETICS
- PREVENTIVE MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The MINISAL-GIRCSI survey is a population-based study designed specifically to assess sodium and potassium intake.
The dietary assessment was carried out using the gold standard biomarker of 24 h urinary excretion of sodium and potassium, strictly following recent guidelines from the WHO.
The geographic proportional sampling from all regions of Italy for both sexes offers national generalisability to the findings.
The choice of the analytical method of a Bayesian geoadditive model allows the simultaneous assessment of spatial (geographic) variations, socioeconomic status (SES) variations, and the linear and non-linear effects of measured and unmeasured confounders.
A limitation is the unavailable dietary assessment of sources of sodium and potassium so that, for sodium in particular, we cannot attribute the differences in salt intake to discretionary or dietary sources.
Also, definitions of SES were based on the head of the household's occupation and participant's educational attainment.
The possibility of residual confounding cannot be categorically ruled out.
Background
Health inequalities by socioeconomic status (SES) are common. The Marmot Review in the UK1 and the work of the Commission on Social Determinants of Health of the WHO2 have highlighted the presence of a social gradient in health inequalities both within and between countries. People of poorer background die sooner and also spend more of their lives with disabilities. Health inequalities are the result of complex interactions of many factors, one of which is poor diet and nutrition. Inequalities in nutrition and SES translate ultimately into inequalities in health.3 In particular, cardiovascular disease is more prevalent in socioeconomically deprived people and groups, including a high risk of stroke, renal failure and hypertension.3 The latter is the most common attributable cause of cardiovascular death and disability.4
Nutritional factors have been causally related to high blood pressure (BP) and, among these, dietary electrolyte intake.5 In particular, epidemiological, clinical and experimental evidence supports a causal relationship between dietary sodium (Na) chloride (salt) intake and high BP.6 The INTERSALT Study showed a direct association between average population salt intake and the increase of BP with age.7 Randomised controlled clinical trials of reductions in Na intake have documented a significant BP lowering effect in hypertensive and non-hypertensive individuals.8 Population-based prospective studies also show that a 5 g/day higher salt intake is associated with a 23% greater risk of stroke.8 ,9
Habitual dietary potassium (K) intake has also been associated with improved cardiovascular health. In prospective studies, a 1.6 g/day higher habitual K intake was associated with a 21% lower risk of stroke.10 Protection against stroke is attributable to the favourable effect of K on BP, as indicated by numerous studies, including the Dietary Approaches to Stop Hypertension (DASH) trial11 and a 1-year long randomised controlled trial showing satisfactory BP control with significantly lower drug consumption in hypertensive patients given a fruit and vegetable K-rich diet compared with a control group.12
There is evidence for SES gradients of habitual Na and K intake in the USA.13 In Britain, in the 2000–2001 National Dietary and Nutrition Survey, salt intake was higher in low socioeconomic groups after allowing for geographic gradients.14 Crucially, after a 8-year salt reduction programme, while dietary as well as total (dietary plus discretionary) salt consumptions have decreased by 0.9 and 1.5 g/day, respectively, social inequalities remained.15 The collection of data on SES gradients in different countries of Europe and their monitoring during policy implementation of salt reduction strategies are important to ensure that the gaps are corrected or at least not inadvertently widened.16
The present study exploits the findings of the MINISAL-GIRCSI programme, a national survey of habitual Na and K intake recently carried out in Italy17 to address the question of whether social inequalities affect electrolyte intake, independent of geographic variations.
Data and methods
Population data
Between 2008 and 2012, the Italian National Institute of Health (ISS) in collaboration with the National Association of Hospital Cardiologists (ANMCO) carried out a Cardiovascular Epidemiology/Health Examination Survey (OEC/HES) and investigated randomly selected age-specific and sex-specific samples of 220 men and women per 1.5 million residents of 17 Italian regions (Friuli Venezia Giulia, Molise, Sicilia, Emilia Romagna, Calabria, Basilicata, Piemonte, Sardegna, Marche, Veneto, Lazio, Umbria, Campania, Liguria, Puglia, Trentino-Alto Adige and Lombardia). A further survey was performed with identical criteria within the framework of the Meno Sale Più Salute Programme in Val d’Aosta, Toscana and Abruzzo, for a total of 20 regions and a final overall study population of 4368 men and 4346 women, aged 35–79 years.18
For the purposes of the MINISAL-GIRCSI and Meno Sale Più Salute studies, a randomly selected subsample of 100 men and 100 women stratified by age and sex was used for each region, based on the WHO recommendation that a sample of 100–200 individuals is required to estimate sodium intake with a 95% CI about the mean of consumption of ±12 mmol/day using a single 24 h urine collection.19
In addition to a 24 h urine collection, this subproject contained a questionnaire covering sociodemographic information (age, sex, level of education, occupation), lifestyles (physical activity at work, alcohol consumption, smoking habit) and anthropometric and BP measurements. Anthropometric measurements were performed in underwear: height by stadiometer, rounded to the nearest centimetre, weight was measured by a balance beam scale recorded in kilogram and rounded to the nearest 200 g. Body mass index (BMI) was calculated on the basis of height and weight (weight (kg)/height(m2)). BP was measured three times on the right arm in sitting position, after 5 min rest, with a mercury sphygmomanometer, and their average was recorded. Hypertension was defined if the participant was on hypertension medication, or had BP ≥140/90 mm Hg. Participants’ smoking habit was coded as current smoker, former smoker and never smoked. Daily alcohol consumption was reported in grams.
Each participant's marital status was described by one of the following categories: married/cohabited, single, separated/divorced, and widowed. SES was measured by two indicators: education and occupation. By answering the question of educational attainment, participants were coded as university degree, high school, junior high school, or primary school or equivalent. The occupation of the participants was coded into eight occupational categories: top managerial occupations, white collars or civil servants, low managerial occupations, high-skill workers, low-skill workers and others (including student, housewife, unemployed, disabled and those temporarily laid off). Since housewives accounted for more than 10% of the total study population, these participants were grouped as ‘housewife’ in the occupation variable. The rest in the ‘others’, where the majority did not provide information of occupation, were treated as missing values.
Each participant's physical activity during work was measured by four levels: work performed mainly sitting at a desk and generally without the need to walk (inactive), work that implies standing and walking for a long time (mildly active), work that implies a lot of walking and handling heavy weights (moderately active), and hard manual work, with great efforts and lifting and handling heavy weights (vigorously active). For the retired participants, the physical activity information was based on their last job. Twenty-four-hour urinary Na and K excretions were derived from the product of the urinary Na and K concentrations and urine volume. Any urine collections less than 500 mL or with a creatinine excretion lower than the population mean minus two SDs were discarded to ensure the completeness of the collection.20 The final sample of this subproject was 3857, that is, the subject of the present report. Other methodological features of the survey have been detailed elsewhere.17 ,20
Statistical methods
Preliminary analysis was performed in SPSS (V.22, Armonk, New York, USA: IBM Corp). The Kruskal-Wallis test was used to compare 24 h urinary Na and K excretions across all regions. The model estimation was performed in BayesX (V.2.1).21 Bayesian geoadditive mixed models were used to assess the spatial effect, SES pattern and non-linear effects of covariates of Na and K excretion.21 ,22 Briefly, the overall spatial effect consists of a correlated spatial effect and an uncorrelated (ie, random) spatial effect, which represent an underlying spatial structure and a locally present effect, respectively. Based on the Markov Chain Monte Carlo (MCMC) simulation, this class of models provides a unified framework for modelling linear and non-linear effects simultaneously, as well as the underlying spatial process. A more detailed introduction has been described elsewhere.14 ,15 A reference level was specified for each categorical factor: sex (reference=female), smoking habit (never smoked), education (university degree), occupation (top managerial occupations), marital status (married/cohabited), physical activity (inactive) and hypertension (no hypertension).
To adjust for different factors and covariates, as well as linear, non-linear and spatial effects, six models were built and compared for both 24 h Na and K. The model with lower deviance information criterion (DIC) was preferred. Models 1–4 included spatial and linear effects only. In model 4, occupation was first included (model 4a) and then replaced by education (model 4b). This was to assess and compare different SES effects on Na and K by different SES measurements. Twenty-four-hour urinary Na and K excretions were log-transformed to be normally distributed. The details of models’ definition and DIC results are presented in online supplementary appendix S1. The Bayesian inference calculates the probability of different values of the measured parameter ‘given’ the data. This probability distribution is called the ‘a posteriori probability’ or simply the ‘posterior’. Bayesian approaches can summarise their uncertainty by giving a range of values on the posterior probability distribution that includes 95% of the probability—this is called a ‘95% credibility interval’.
Spatial boundaries
Participants were recruited from 20 administrative regions (table 1). Sicilia and Sardegna do not share any land border with other regions. To include them in the analysis, neighbouring regions were defined for each region using R (R2 BayesX package).21 Hence, Calabria was considered as the only neighbour to Sicilia, and Lazio, Liguria and Toscana were considered neighbours to Sardegna. Alternative sets of neighbours of Sardegna, that is, Lazio and Toscana or Lazio only, were used in the models to test the sensitivity of the neighbour definition.
Basic characteristics of the Italian observatory epidemiological cardiovascular/Health Examination Survey 2008–2012 (N=3857)
Results
Basic characteristics
The characteristics of the participants are presented in table 1. In total, 1894 women and 1963 men, aged from 39 to 79 years, were included in the analysis. Aside from the 14.6% university degree holders, there was an increasing trend of educational attainment from the primary school to high school certificates. High-skill workers, white collars/civil servants and low-skill workers were the top three occupations. The median 24 h urinary Na excretion was 154.1 mmol/day (approximately 9 g of salt per day, 1 g salt=17.1 mmol Na). The median 24 h urinary K excretion was 57.6 mmol/day (approximately 2.25 g of K per day, 1 mmol=39 mg of K). The median 24 h urinary Na and K excretion varied significantly across all regions (p<0.001 for both; table 2).
Twenty-four-hour urinary sodium and potassium excretions by region and equivalent dietary salt and potassium intake
Three neighbouring southern regions, Calabria, Basilicata and Puglia, had the highest level of urinary Na excretion (figure 1 and table 2) and Friuli Venezia Giulia had the lowest level of K excretion (table 2). The map suggests an increasing north-south pattern of 24 h urinary Na excretion and a higher urinary K excretion in the central regions.

Observed median 24 h urinary sodium (left) and potassium (right) excretion by region. Red (green) indicates a high (low) level of 24 h urinary sodium (left) and potassium (right) excretion.
By comparing the (DIC) values of the models, model 4a performed the best (see online supplementary appendix S2). However, both models 4a and 4b will be presented here to show the effects of both SES indicators on 24 h urinary Na and K excretion.
Determinants of sodium excretion
As the Bayesian models do not produce any p values, statistical significance for the fixed Na effect was determined by the position of the overall 90% credible intervals (table 3). Age, sex and BMI were significantly associated with 24 h urinary Na excretion. Men, younger participants or those with higher BMI were more likely to have a higher Na intake (table 3).
Estimated posterior means and 90% credible intervals of fixed factors for sodium excretion by occupation and educational attainment
Although model 4a performed better than model 4b, both SES indicators, occupation and education, showed a significant independent association with 24 h urinary Na excretion. With the exclusion of housewives, those in occupations III and IV had higher 24 h urinary Na excretion (reflecting higher salt intake) compared with occupations I and II (figure 2, top left panel; p for linear trend <0.001; F=16.5; df=4). When compared with occupation I (white collars and civil servants), occupations III and IV had, on average, a 5.6% and 6.6% higher salt intake, respectively. Likewise, those with a lower level of education (occupations III and IV) had higher salt intake compared with those with the highest level of education (figure 2, top right panel; p for linear trend <0.0001; F=8.5; df=3). When compared with those with a university degree, those with primary and junior school education had, on average, a 3.9% and 7.7% higher salt intake, respectively.
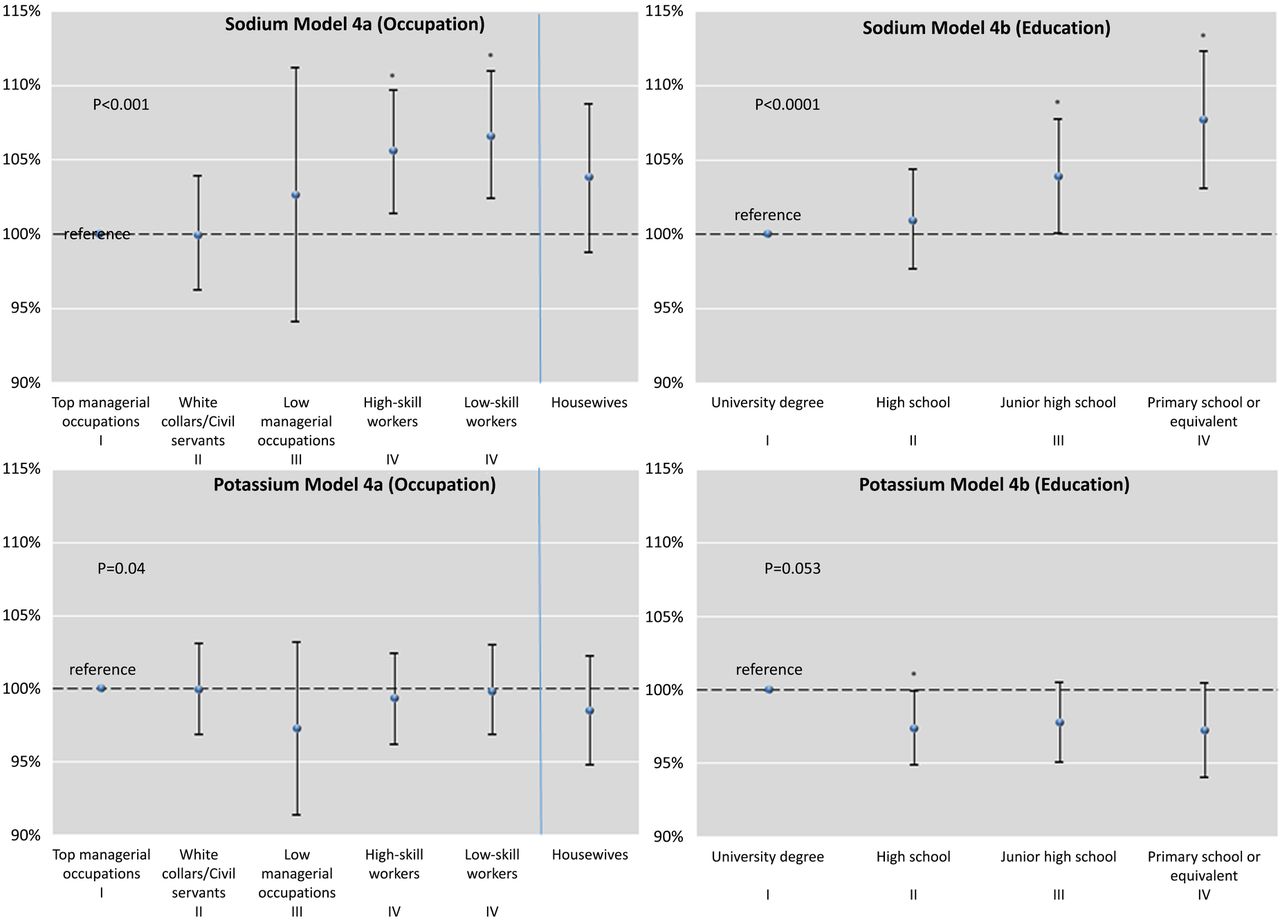
Effects of socioeconomic status by occupation (left panels) and by education (right panels) for sodium (top) and potassium (bottom) excretion. Note: Values are back log-transformed. Top managerial occupations and university degree were the reference levels for occupation and education, respectively. *Significant effect compared with the reference level at p<0.05. p For linear trends reported in the panels (excluding housewives).
Determinants of potassium excretion
K excretion did not vary by age; however, sex, BMI and alcohol consumption were significantly associated with 24 h urinary K excretion (table 4). Men, those with higher BMI and who were drinking more were more likely to have a higher K intake. Hypertensive individuals had a lower K excretion. There was no consistent association between K excretion and SES (p for linear trend=0.04 and 0.053 for occupation and educational attainment, respectively; figure 2, bottom panels); however, participants with primary and junior school education had significantly lower K compared with those with a university degree (figure 2, bottom right panel). The difference was 2.6%.
Estimated posterior means and 90% credible intervals of fixed factors for potassium excretion by occupation and educational attainment
Spatial map of 24 h urinary sodium excretion
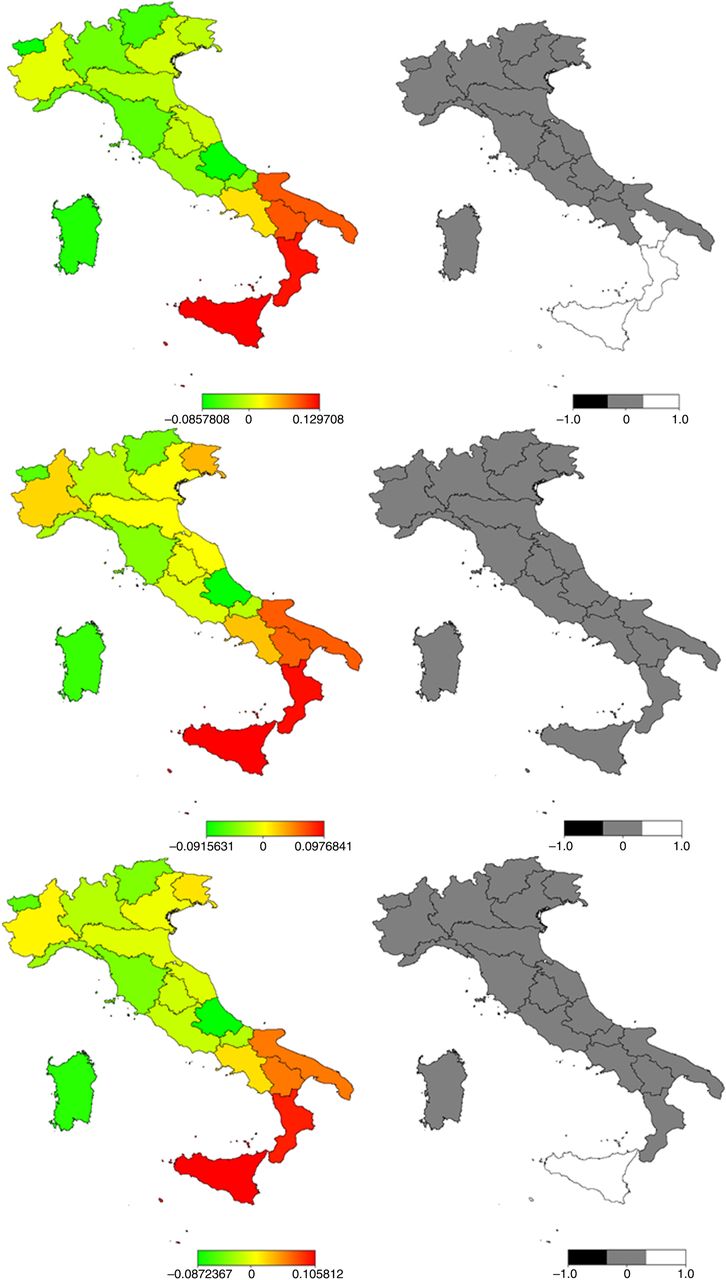
Model 1 only accounted for the spatial effect. Figure 3 (top panel) shows the estimated mean effect map (left) and the probability map of the structured spatial effect (right). Twenty-four-hour urinary Na was higher in the south and lower in the central and northern regions. In particular, the probability map suggested a significantly higher Na level in three southern regions (shown as white colour).

{kind=link}
{kind=link}
{kind=link}
Estimated mean maps (left) and 90% probability maps (right) of log-transformed 24 h urinary sodium excretion. Top panel shows the maps using model 1 with spatial effect only; the middle and bottom panels show results using models 4a and 4b with occupation and education, respectively. In the mean map, red (green) indicates a high (low) level of 24 h urinary sodium excretion. In the probability map, grey indicates a non-significant spatial effect, and white (black) indicates a significantly positive (negative) spatial effect at 90% credible level.
Although the posterior means still showed a higher level of Na in the southern regions for models 4a and 4b, the probability map suggested no significant spatial variation after controlling for SES variables (figure 3, middle and bottom panels). In other words, geographic variations in salt intake across Italy are explained by SES variations and are attenuated or disappear once this relationship is taken into account.
Spatial map of 24 h urinary potassium
There was no significant spatial variation of K intake in Italy based on the results of model 1, although the central and southern regions showed higher salt intake than other regions (see online supplementary appendix S3). After controlling for the SES variables, the models 4a and 4b of 24 h urinary K showed a different spatial distribution, compared with the Na estimated mean maps. The central and southern regions had higher K excretions. The spatial effect difference between the occupation and education models suggests that education may explain some of the spatial variation.
Discussion
This study shows in a representative sample of Italian men and women that salt intake—estimated using 24 h urinary Na excretion—varies across Italy, being higher in the South. Crucially, the study shows for the first time that salt intake is significantly higher in less advantaged social groups (both by occupation and by level of educational attainment). This social gradient is independent of age, sex, BMI, hypertension and other behavioural variables. Finally, the social gradient explains the geographical variation seen in unadjusted models. The study also describes the geographic and SES variations in K excretion, a biomarker of K intake23 and a close indicator of fruit and vegetable intake.23 K intake, an effective protective factor for high BP24 and stroke,10 ,24 is higher in the central and southern regions and lower in those with lower education attainment.
Strengths and limitations
The study has a number of strengths. The MINISAL-GIRCSI survey is a population-based study17 designed specifically to assess Na and K intake using the gold standard biomarker of 24 h urinary excretion of Na and K, strictly following recent guidelines from the WHO.19 ,25 These estimates approximate very closely the total consumption of Na and K and they allow the most reliable assessment of population averages—particularly for Na—compared with other methods.26 ,27 Na intake is a combined sum of Na present in natural food (approximately 10%), Na added by the consumer when cooking and at the table (approximately 36%) and that present in processed food as added by the manufacturing process (approximately 54%).28 Hence, dietary assessments would tend to grossly underestimate total salt intake. The geographic proportional sampling from all regions of Italy for both sexes offers national generalisability to the findings. The choice of the analytical method of a Bayesian geoadditive model allows the simultaneous assessment of spatial (geographic) variations, SES variations, and the linear and non-linear effects of measured and unmeasured confounders. One limitation is the unavailable dietary assessment of sources of Na and K so that, for Na in particular, we cannot attribute the differences in salt intake to discretionary or dietary sources of Na. Also, definitions of SES were based on the head of the household's occupation and participant's educational attainment. While limited,29 ,30 these measures have been consistently used in Italian national surveys.31 They are also consistent with measures in other studies.14 ,15 Finally, the possibility of residual confounding cannot be categorically ruled out.
Context
The results of the MINISAL-GIRCSI survey confirm high levels of dietary salt intake in Italy when compared with the targets set by the WHO.19 ,25 Furthermore, there is substantial geographic variation, mostly accounted for by SES variations. For K intake, the average levels are also lower than recommended by the WHO32 with both geographic and SES variation. These results are of interest since the Mediterranean diet of southern Italy, as described in the Seven Countries study, has been traditionally considered as very close to if not the ideal diet.33 At the time, however, the salt content of food had not been considered, and emphasis was placed on the good balance between saturated fat and fruit and vegetables. Things have changed since the 1960s and 1970s socioeconomically. On the one hand, we document a high salt intake, higher in the more deprived regions of the south, and a lower than expected K intake, reflecting a reduced consumption of fruit and vegetables. The increasing prevalence of obesity in the southern regions, critical among the younger age groups,34 ,35 would support the notion that there has been an increase in the use of convenience food, likely to be higher in salt and with reduced K,34 in addition to the documented increase in calorie intake and physical inactivity. This study was carried out as part of a wider national initiative to increase awareness about the high salt intake of the Italian people,36–38 to engage with bread manufacturers to reduce the salt content of bread,39 a major source of salt in the Italian diet, to initiate discussions with food manufacturers on voluntary reformulations and to monitor the population salt intake in the years to come to implement an effective surveillance system and policy evaluation.40
Implications for policy
The detection of an SES gradient in salt intake is important for policymakers. An attempt to change individual behaviour through healthy eating campaigns, while useful to increase awareness and reinforce consumer choice, is unlikely to bring about the changes necessary to achieve the recommended targets for salt intake.40 They may also widen inequalities.41 ,42 Indeed, the diet of socioeconomically disadvantaged groups in Italy, as well as in other European countries, comprises low-quality, salt-dense, high-fat, high-calorie and inexpensive foods.3 ,43–46 A greater consumption of bread and other baking products, which, according to the chemical analysis of the national diet performed by the Italian Institute of Nutrition in 1994–1996, is the main source of non-discretionary salt in Italy,47 may contribute to the higher salt intake by the lower SES groups. The access to, and consumption of, healthy foods depend on socioeconomic factors.1 Data from the Moli-sani study in Italy suggest that the quality of the diet worsens during a period of economic hardship.48 On the other hand, a ‘downstream’ approach of reformulation and, if necessary, regulation would be expected to reduce inequalities.41 ,49 ,50 It is of interest that in Britain, SES inequalities are still detectable 8 years after a national programme that has achieved overall a 15% reduction in average salt intake.15 The programme was originally based on three waves of awareness campaigns, followed by a voluntary agreement with the food industry leading to reformulation of some foods and, more recently, emphasis being given to individual behavioural change through the Responsibility Deal.51 The fragmented approach may have resulted in a less effective impact on those who needed to reduce salt intake the most, that is, the low socioeconomic groups.
Conclusions
Social inequalities in Na and, to a lesser extent, in K intake are present in Italy. It is crucial that the SES patterns of salt intake be taken into account and monitored in the implementation of salt reduction programmes in Italy. In addition, the finding of a surprisingly low dietary K intake points to the decline of the traditional Mediterranean dietary model with insufficient fruit and vegetable intake, which is coupled with excess consumption of processed and salty foods, especially among the lower socioeconomic groups.
Acknowledgments
This analysis was carried out under the terms of reference of the WHO Collaborating Centre for Nutrition of the University of Warwick.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
FPC and CJ contributed equally.
Contributors FPC developed the idea, supervised and obtained funding for the analysis, and drafted the manuscript. CJ jointly developed the analytical approach to data handling, carried out the analysis and drafted the analytical part of the manuscript. FPC and CJ contributed equally. SG is the principal investigator (PI) of Progetto Cuore and PS is the PI of MINISAL-GIRCSI. They designed the population studies, obtained funding, supervised the field work and checked the results. CD, LP, RI and DV were directly involved in data collection in different regions, also providing quality control. All authors contributed to the final version of the manuscript. FPC is the guarantor.
Funding This work was supported by the National Centre for Prevention and Disease Control (CCM) of the Italian Ministry of Health (MINISAL-GIRCSI and Meno Sale Più Salute, Osservatorio Epidemiologico Cardiovascolare/Health Examination Survey within the Progetto CUORE coordinated by the Istituto Superiore di Sanità) and The Bupa Foundation (MR-12-002).
Competing interests FPC is an unpaid member of CASH, WASH, the UK National Forum, the UK Public Health NACD; unpaid technical advisor to NICE, the WHO Geneva and Office for Europe, EMRO Region and the Pan American Health Organization; and Trustee of the Student Heart Health Charity. PS is an unpaid member of WASH.
Ethics approval Ethics Committee of the Federico II University of Naples.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.