Article Text

Abstract
Objectives To assess the association between secondhand smoke exposure and blood lead and cadmium concentration in women in South Korea.
Design Population-based cross-sectional study.
Setting South Korea (Korea National Health and Nutrition Examination Survey V).
Participants 1490 non-smoking women who took part in the fifth Korea National Health and Nutrition Examination Survey (2010–2012), in which blood levels of lead and cadmium were measured.
Primary outcome measures The primary outcome was blood levels of lead and cadmium in accordance with the duration of secondhand smoke exposure.
Results The adjusted mean level of blood cadmium in women who were never exposed to secondhand smoke was 1.21 (0.02) µg/L. Among women who were exposed less than 1 h/day, the mean cadmium level was 1.13 (0.03) µg/L, and for those exposed for more than 1 h, the mean level was 1.46 (0.06) µg/L. In particular, there was a significant association between duration of secondhand smoke exposure at the workplace and blood cadmium concentration. The adjusted mean level of blood cadmium concentration in the never exposed women's group was less than that in the 1 h and more exposed group, and the 1 h and more at workplace exposed group: 1.20, 1.24 and 1.50 µg/L, respectively. We could not find any association between lead concentration in the blood and secondhand smoke exposure status.
Conclusions This study showed that exposure to secondhand smoke and blood cadmium levels are associated. Especially, there was a significant association at the workplace. Therefore, social and political efforts for reducing the exposure to secondhand smoke at the workplace are needed in order to promote a healthier working environment for women.
- TOXICOLOGY
- OCCUPATIONAL & INDUSTRIAL MEDICINE
- PRIMARY CARE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to show that women have elevated blood cadmium levels with increased exposure level to secondhand smoke (SHS), and there is a correlation between blood cadmium levels and the exposure level to SHS at work.
We evaluated a nationally representative sample so that the results of our study would reflect characteristics of the general non-smoking female population in South Korea.
We compared the exposure between home and workplace, which has not been evaluated concurrently in previous studies.
Out study has several weaknesses: First, people who work in areas with higher chance of exposure to lead and cadmium were not considered. However, the number of women who work in such areas is very low in South Korea, so it is unlikely to have an effect on the research. Second, the survey was not conducted on metal intake through the consumption of food. However, daily exposure to cadmium and lead through food is low in South Korea.
Introduction
Exposures to secondhand smok (SHS) has been a major public health concern as it is causally linked to lung cancer, stroke, coronary heart disease, nasal irritation and harmful reproductive effects in women.1 There has been significant progress to reduce SHS exposure. However, nearly half (46.4%) the non-smokers in the USA remain exposed.1 In South Korea, 4.9% of men and 16.7% of women were exposed to SHS at home and 55.2% of men and 37.2% of women were exposed to SHS at the workplace in 2011.2 ,3 Overall, more than 30% of non-smoking adults and adolescents were still exposed to SHS in 2014.4 Smoke-free policies have shown incremental progress since 1995, but smoking is still permitted in many indoor public places.4
Cigarette smoke consists of mainstream smoke from the mouth during puffing and sidestream smoke from the lit end of the cigarettes between puffs. The sidestream smoke can reach deeper areas in the lung because the size and concentration of the particles are smaller and higher, respectively, than those of mainstream smoke. SHS is a mixture of sidestream smoke and exhaled mainstream smoke,5 and contains more than 4000 chemical compounds known to cause diseases, including nitrosamines, polycyclic aromatic hydrocarbons, cadmium, chromium, lead and nickel.5 ,6 Lead and cadmium have been particular concerns due to their carcinogenicity, tendency to accumulate in the body and their potential toxicity to the developing fetus.7 ,8
There are strong associations between the blood lead levels and active smoking, as well as between blood cadmium levels and active smoking.9–11 Also, Leroyer et al,12 and Lee and Ha,13 have proven the existence of a dose–response relationship in these associations, providing strong evidence that active smoking increases blood lead and cadmium levels. Richter et al14 found that urine lead levels among adults with high SHS exposure were similar to those of smokers, but the study was not considered, as it was based on the results from data adjusted only for creatinine and other various covariates, which might have influenced the results. Furthermore, there have only been a few studies that have revealed an association between SHS exposure and blood lead and cadmium, thus far.
This study was conducted to examine the association between SHS and blood lead and cadmium concentration while considering the possible confounding factors and to demonstrate how SHS at home and in the workplace can influence blood lead and cadmium levels differently in South Korean women.
Methods
Materials and methods
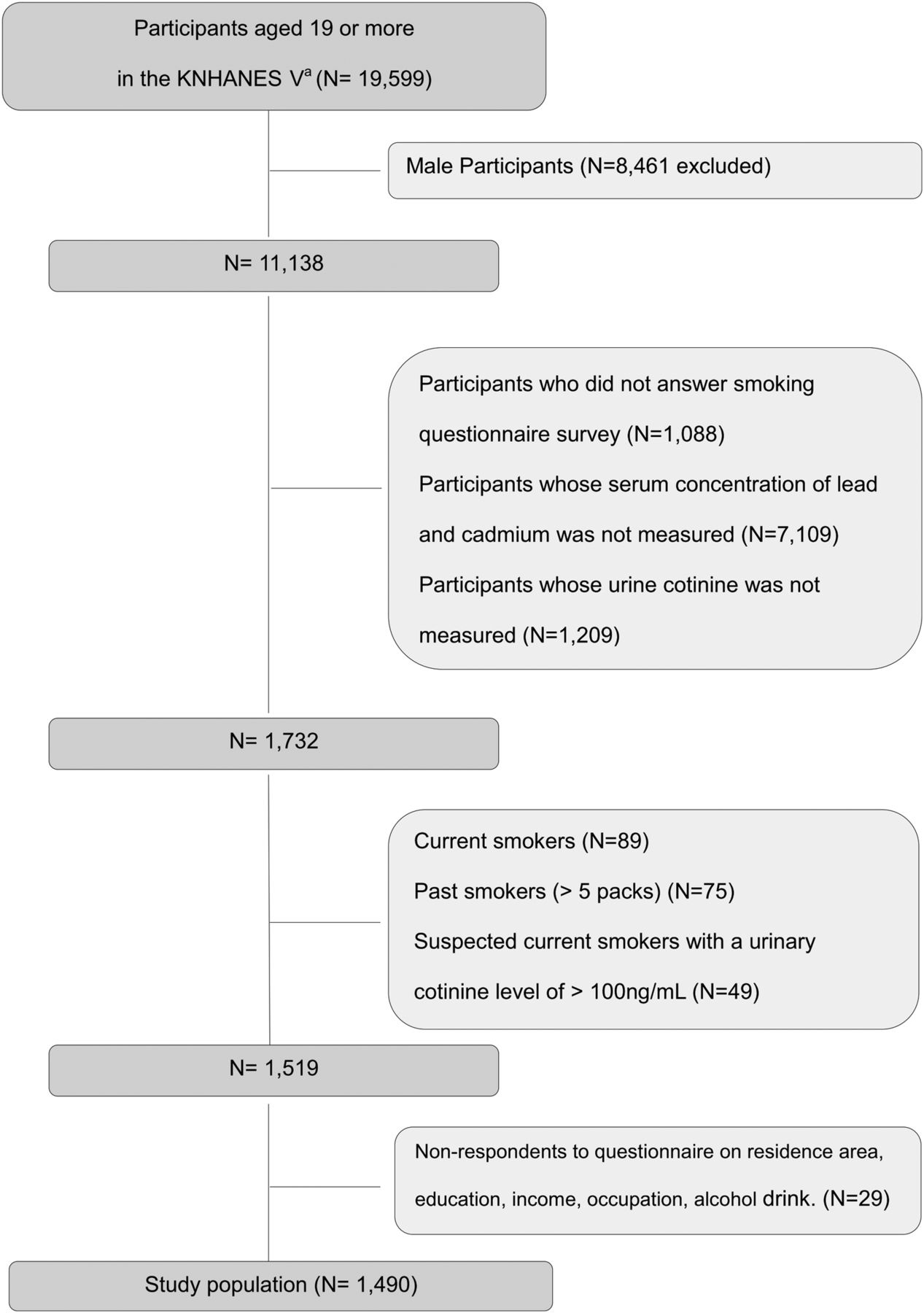
Eligible participants are listed in figure 1. The Korea National Health and Nutrition Examination Survey V (KNHANES V; 2010–2012) was a nationwide survey representing the general South Korean population and included comprehensive information on the health status, health behaviours and sociodemographic characteristics of 25 533 participants. A total of 1490 participants were included in this study in accordance with the eligibility criteria. The KNHANES V used a stratified multistage probability sampling so that the sampled population accurately represents the general population of South Korea. A total of 1490 participants represented the South Korean population of 9 600 000. Since the survey data analysed are publicly available, this study was exempt from review by the Institutional Review Board.

{kind=link}
Study population (KNHANES V, Korea National Health and Nutrition Examination Survey V).
SHS status was assessed among lifetime never-smokers, via a self-reported questionnaire. Then the participants were categorised into each group according to the duration of total exposure during a 1 day period (0, >0 to <1, and ≥1 h), the duration of exposure at home (0, >0 to <1 and ≥1 h) and the duration of exposure at the workplace (0, >0 to <1 and ≥1 h). The participants were also asked if they had cohabiting family members who actively smoked (yes/no).
The urinary cotinine excretion is an index that reflects the degree of exposure to SHS as well as direct smoking. For the Korean National Health and Nutrition Examination Survey, urinary cotinine excretion was analysed using a gas chromatograph/mass spectrometer from PerkinElmer Clarus 600 T (PerkinElmer/Finland), which has a detection threshold of 0.28 ng/mL. While a previous study has proposed a urinary cotinine level of 50 ng/mL as the cut-off value to differentiate between active smokers and non-smokers,15 this value has not been validated for Asians. Kang et al16 suggested that a urinary cotinine level of ≥100 ng/mL was an optimal value to distinguish never-smokers from active smokers in the South Korean population. The sensitivity and specificity of the criteria were 94.4% and 100%, respectively. Kim and Jung17 supposed that a urinary cotinine level of ≥164 ng/mL also could be used to separate never-smokers from active smokers. The sensitivity and the specificity ranged from 87.1% to 93.8% and from 82.9% to 94.9%, respectively. In our study, it was important to detect the association of SHS with lead and cadmium concentrations in the blood that were only influenced by SHS. Therefore, participants with a urinary cotinine level of ≥100 ng/mL were classified as current smokers due to the criteria having a higher specificity. In this study, current and past smokers were excluded through interviews and suspected current smokers, whose urinary cotinine concentration was above 100 ng/mL, were also excluded.
Blood samples were obtained through a venipuncture, and lead and cadmium levels in the blood were measured by Graphite furnace atomic absorption spectrometry (GFAAS, AAnalyst AAS-600, Zeeman correction, Perkin Elmer, Singapore) performed by the Neodin Medical Institute. The laboratory equipment to detect blood lead and cadmium was controlled by using standard reference material from Whole Blood Metals Control (BIO-RAD, USA) for internal quality assurance, and the coefficient of variation for lead and cadmium levels was kept within 10%. Additionally, external quality assurance satisfied G-EQUAS (German External Quality Assessment Scheme), which is a standard protocol to detect the presence of low dose chemicals. The detection limits of blood lead and cadmium levels from the equipment were 0.0223 and 0.087 µg/dL, respectively, and all values detected were kept within the detection limit.18
The age of the participants was limited to 19 years and older. The residential area was classified based on Dong (city) and Eup (rural area) of the administrative district. Occupation was divided into three broad categories: non-employed, blue collar workers and other workers. Other workers included agriculture, forestry and fishery workers, machine-operating assembly line workers and simple labourers, among others. Household income was divided into quartiles. Education was divided into four levels: below elementary school level, middle school graduate, high school graduate and college graduate or higher. Average daily alcohol consumption was calculated based on the total quantity per occasion and frequency of drinking in the past year, and divided into three categories: no alcohol intake, 0–9 g of alcohol and intake of 10 g or more. Alcohol intake frequency questions (alcohol intake frequency per month and the amount of alcohol consumption per occasion) were not open answer questions so the average value for each range was applied. We converted the amount of alcohol intake to pure alcohol content (1 glass=approximately 10 g).
Statistical analysis
All analyses were performed using STATA statistical software V.13.0 (Stata Corp, College Station, Texas, USA). The differences in clinical characteristics according to SHS status were assessed using unpaired t tests for the continuous variables and χ2 test for the discrete variables. We obtained a p value for trend across categorical variables.
We assessed the associations between self-reported SHS status and urinary cotinine concentration to evaluate whether significant discrepancies existed between them. We used an analysis of variance model to determine the statistical differences in mean urinary cotinine according to each SHS status.
We conducted multiple linear regression analyses to calculate the adjusted means of lead and cadmium. We used the following covariates: age, residential area (rural/urban), education level, household income, alcohol intake and occupation. Lee and Ha13 proved that lead and cadmium concentrations increased with age and alcohol intake in the South Korean population. Shin et al19 showed that occupational class, family income and educational level could influence lead and cadmium concentrations in the blood for the South Korean population.
All analyses were weighted to the South Korean standard population from 2010 to 2012, which had reflected weights to the response rate, weights to sampling and weights to the population structure of the KNHANES parent study. A p value <0.05 was considered significant, and we also displayed 95% CI.
Results
Baseline characteristics
The sociodemographic characteristics and urinary cotinine concentration of the participants are presented in table 1.
Characteristics of study participants according to self-reported secondhand smoke (SHS) exposure (n=1490, N=9.6e+06)
Among the total number of participants, 31.9% had been exposed to SHS. The mean age of the SHS-exposed group was significantly lower than that of the SHS-non-exposed group (p<0.001). The mean urinary cotinine concentration of the SHS-exposed group was significantly higher than that of the SHS-non-exposed group (p<0.001). Residential area was not statistically different between the two groups. There were no consistent trends between educational level or family income and increased exposure to SHS. However, compared to participants with an educational level of elementary school or with the first quartile of family income, participants with an educational level of high school or with the third quartile of family income had higher tendency to be exposed to SHS with statistical significance (OR 1.84, p value 0.004 and OR 1.84, p value 0.013 respectively). We found a consistent increase of SHS exposure as the amount of daily alcohol intake increased (p<0.001). Compared to participants who were not employed, blue-collar workers and non-blue-collar workers had higher tendency to be exposed to SHS with statistical significance.
Urinary cotinine concentration and self-reported SHS status
Table 2 shows the total duration of SHS exposure was related to urinary cotinine (p<0.001).
Urinary cotinine concentration in relation to self-reported SHS environment
The duration of exposure, both at work and at home, was related to urinary cotinine (p=0.007 for at work; p=0.005 for at home). Participants with cohabiting family members who actively smoked had a higher mean urinary cotinine concentration (9.02 ng/mL) than that of controls (5.65 ng/mL), with statistical significance.
Lead and cadmium concentration according to self-reported SHS status
Table 3 shows lead and cadmium concentrations in the blood compared to the duration of exposure to SHS.
Association between self-reported SHS exposure and blood concentration of lead/cadmium in never-smokers
No difference was observed in lead concentration according to SHS status, which was classified by the duration of exposure at workplace, exposure at home and total exposure. However, cadmium concentration in the blood differed depending on the exposure status. Compared to participants who were never exposed to SHS, participants who were exposed to SHS longer than 1 h at work or home, and total exposure, demonstrated higher cadmium concentration (1.20 vs 1.50 with p value 0.001; 1.21 vs 1.45 with p value 0.04; 1.21 vs 1.46 with p value <0.0001). We found a consistent increase in cadmium concentration as the time of SHS exposure at work increased (1.20, 1.24 and 1.50 µg/L, p=0.005). No difference was found in lead and cadmium concentrations between participants living with active smokers, and participants not living with active smokers (p=0.79 for lead and p=0.43 for cadmium after adjusted for covariates).
Discussion
In this study, we have demonstrated a significant association between blood cadmium concentration and SHS exposure in a large nationally representative sample. From an adjusted analysis, we found a consistent increase of blood cadmium concentration among participants who were exposed to SHS at workplaces. Additionally, we found that participants who were exposed to SHS for a longer duration than 1 h at home and at total exposure had higher blood cadmium concentration compared with participants who were never exposed to SHS. After adjusting for confounding factors that could influence blood concentration of the metals, we confirmed that regression coefficients of linear regression models were increased with statistical significance in the analyses of cadmium concentration of total SHS exposure and SHS exposure at workplaces. (Before adjustment, regression coefficient was 0.034 with p=0.313. After adjustment, regression coefficient was 0.084 with p=0.006; before adjustment, regression coefficient was 0.042 with p=0.30. After adjustment, regression coefficient was 0.11 with p=0.005.) That means the effects of exposure to SHS on cadmium concentration in the blood became more obvious after adjusting for confounders. No significant difference was found in the levels of lead and cadmium between participants living with smokers and those not living with smokers. (For lead p=0.79 after adjustment, for cadmium p=0.43 after adjustment.) Given the general circumstances in South Korea, having cohabiting smokers does not always suggest that participants will be exposed to SHS at home, as South Korean smokers usually smoke outdoors, usually on balconies, or in gardens or public outdoor spaces near home, and not indoors. Therefore, despite having cohabitants who are active smokers, participants might not be exposed to a significant amount of SHS in South Korea.
Several previous studies support the results of this work. Tobacco is well known as a notable source of cadmium and lead.20 Exposure to cigarette smoke via active and passive smoking was found to increase blood cadmium concentration among 158 workers in Israel.21 It was reported that urinary lead concentration was found to be increased according to SHS status in the US adult population.14 In Sweden, urinary cadmium concentration correlated with urinary cotinine concentration among 23 children with asthma.22
Studies on the relationship between SHS and lead concentrations in the blood have mainly been conducted with the participation of children as research subjects. It was found that lead concentrations in the blood increased as the number of smokers at home increased.23 Richter et al24 analysed blood lead level using NHANES 1999–2008 and found that higher exposure to SHS resulted in higher blood lead concentration. However, the result was more prominent in children and adolescents than in adults. In our study, we could not find any association between lead concentration in the blood and SHS exposure status. This may owe to the age range of our study population (44.71 years for those who were never exposed to SHS; 50.15 years for those who were exposed to SHS) being greater than the age range of adolescents or children. This can be explained by the fact that lead exposure comes largely from the general environment, including ambient air, diets and daily life activities.25
Cadmium can enter the body through ingestion, inhalation and the skin. Between 10% and 50% of inhaled cadmium can be absorbed, and between 5% and 10% of ingested cadmium can be absorbed. The absorption of cadmium through the skin is negligible. The average cadmium concentration in the blood is twice as high in smokers as that in non-smokers.25 South Korean FDA (Food and Drug Administration) investigated the concentration of metals in foods available in South Korea. It announced that the total cadmium intake through all available foods was 10.4 μg/day, which was 22.7% of PTMI (Provisional Tolerable Weekly Intake). Grain was attributed most to cadmium concentration, which was 22.9% of the total cadmium intake. Daily intake of cadmium in South Korea was similar to that in the USA, Britain, France and Germany, but lower than that in Japan, Australia and New Zealand.26 In South Korea, cadmium exposure of those over the age of 10 years was lower than the level recommended by Center for Disease Control, Commission on Human Biological Monitoring (CHBM), WHO and Environmental Protection Agency (EPA).27 Therefore, additional exposure to cadmium, by direct or passive smoking, is critical because it can increase the risk in disease processes caused by the metal, which could be preventable. Cadmium is classified as a human carcinogen by the Interactional Agency for Research on Cancer. Cadmium may be one of the risk factors for cardiovascular mortality and the deterioration of renal function. Moreover, the level of cadmium is critical for postmenopausal and premenopausal women because osteoporosis, osteomalacia and bone fracture caused by cadmium occur mainly among postmenopausal women, in addition to potential teratogenicity.25 ,28
South Korea has not yet implemented the comprehensive ban on indoor smoking in public places and workplaces recommended in the FCTC (Framework Convention on Tobacco Control) Guidelines. Smoking indoors in workplaces has decreased from 47% of smokers in 2005 to 32% in 2010. However, the decrease was less significant compared with other countries where smoking in workplaces has decreased to less than 10% after implementation of the ban on indoor smoking. The level of observed smoking in indoor workplaces was higher than other high-income ITC (International Tobacco Control) countries such as the USA, France, Canada, Ireland and Australia, and higher than middle-income ITC countries such as Mexico, Malaysia and Brazil.29 Furthermore, a ban on smoking in homes has been significantly less implemented in South Korea than in the USA.30 Cadmium is especially harmful to women due to its potential catastrophic effects to the fetus. Thus, emphasis must be placed on a social dimension regarding the dangers of SHS in order not only to prevent cancer, cardiovascular diseases and respiratory diseases, but also to prevent increased concentration of cadmium in the blood.
Limitations
Our study has several limitations. First, people who work in areas with higher chance of exposure to lead and cadmium were not considered. However, the number of women who work in such areas is very low in South Korea, so it is unlikely to have an effect on the research. Second, the accumulation of metals in the blood is a long-term process. Variables such as exposure to SHS used in this study are evaluated at the present time. This can bias the results. Third, the study was based on a self-administered questionnaire about the exposure to SHS used as a proxy variable reflecting the SHS exposure status. This can lead to biased results. Lastly, the survey was not conducted on metal intake through the consumption of food. Although daily exposure to cadmium and lead through food is low in South Korea, further studies are needed to show their exact relationships.
Despite these limitations, our study has several strengths. We evaluated a nationally representative sample so the results of our study would reflect characteristics of the general non-smoking female population in South Korea. Additionally, we compared the exposure between home and workplace, which has not been evaluated concurrently in previous studies.
Conclusions
In this study, we showed that women had elevated blood cadmium levels after increased exposure to SHS, and there was a correlation between blood cadmium levels and the exposure level to SHS at work. This suggests that we need to further evaluate the effect of reduced exposure to SHS on the levels of cadmium in the blood. Even low blood levels of accumulated metals can be harmful to the human body. This study suggests the need for social and political efforts to reduce SHS exposure to promote healthy workplaces for women.
Acknowledgments
The authors would like to thank the members of the Korea Institute for Health and Social Affairs, who conducted the national survey, and all those who contributed to this project and Medical Research Collaborating Center (MRCC) at Seoul National University Bundang Hospital.
References
Footnotes
SYJ and SuK are first authors and contributed equally.
Contributors SYJ and SuK designed the study, analysed the data and drafted the manuscript as first authors. JYK, WKB, KL, J-SH and SaK contributed to the discussion and reviewed the manuscript. KL supervised the study as the corresponding author.
Funding This study was supported by a grant (number 02-2013-094) from the Seoul National University Bundang Hospital Research Fund.
Competing interests None declared.
Ethics approval Institutional Review Board of Seoul National University Bundang Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement KNHANES V dataset is publicly available in South Korea and any requests for analyses will be received on the website: https://knhanes.cdc.go.kr/knhanes/index.do.