Article Text

Abstract
Objectives Although the short-term outcome of therapist-guided internet-based cognitive–behavioural therapy (ICBT) for treating social anxiety disorder (SAD) has been well studied, little research has been undertaken on the sustainability of treatment gains, especially under clinically representative conditions. Further, there is some debate whether delivering psychological treatment via the internet may be suitable for more severely ill patients.
Design Longitudinal multilevel growth-modelling of long-term (1–4 years) follow-up cohort data.
Setting An outpatient psychiatric clinic specialised in internet interventions.
Participants 446 adults having been treated for SAD.
Primary and secondary outcome measures Primary outcomes were estimated improvement rate and Cohen's d effect size on the self-rated Liebowitz Social Anxiety Disorder Scale. Secondary outcome measures were change in comorbid depressive symptoms and health-related quality of life.
Results A large treatment effect was observed on the primary outcome measure after treatment (d=0.8 (95% CI 0.7 to 0.9)), with continued long-term improvements (d=1.2 (95% CI 1.0 to 1.3)). However, the rate of change varied significantly between individuals over time. A faster rate of improvement was observed among patients with higher illness severity, whereas having a family history of social anxiety was related to worse response. Long-term improvements were also observed in comorbid depressive symptoms (d=0.7 (95% CI 0.5 to 0.8)) and health-related quality of life (d=−0.3 (95% CI −0.4 to −0.1)).
Conclusions These findings provide evidence for the long-term effectiveness of ICBT for SAD in routine clinical practice, even for more severe cases.
- PSYCHIATRY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study was conducted in a naturalistic setting and had a relatively large sample size, which increases the likelihood that these findings could extrapolate to patients at other clinics.
A multilevel statistical framework allowed the simultaneous analysis of repeated measurements and higher level predictors.
Includes reporting of adverse effects of treatment.
No comparison group.
Introduction
Social anxiety disorder (SAD) is one of the most common anxiety disorders1 which often follows a chronic course if untreated.2 The core of SAD is a debilitating fear of negative evaluation causing considerable distress in social situations, reduced quality of life and functional impairment for affected individuals.3 Conventional face-to-face cognitive –behavioural therapies (CBT) are among the most established and well researched psychological treatments for SAD.4 However, there are a number of barriers to treatment such as limited availability of trained therapists, stigma, costs of treatment and practical difficulties of attending treatment (eg, taking time off work and geographical distance from treatment facility).5
To increase accessibility, therapist-guided internet-based CBT (ICBT) has been shown to be a promising method of delivering evidence-based psychological treatments. This format of delivering CBT may also be particularly advantageous in the treatment of SAD because of the nature of the disorder, especially for patients presenting with greater illness severity who might fear face-to-face interactions with a therapist.5 ,6 ICBT may, in such cases, be preferable for those who might otherwise avoid seeking help. It has demonstrated efficacy in reducing symptoms and with effect sizes comparable to conventional face-to-face CBT.7 A review of 21 studies reported large within-group effect sizes for both guided and unguided internet-based interventions for SAD.8 Although sustained effects of ICBT have been reported for up to 5 years after treatment, these results are reported from clinical trials.9–11 Although there is evidence that ICBT may also be equally effective as group CBT for SAD under clinically representative conditions,12–14 more knowledge on the long-term effectiveness of ICBT for SAD in naturalistic settings (ie, when delivered as part of routine clinical practice) is needed, since the context of routine care may differ significantly from the context of controlled trials with respect to factors such as selection criteria, monitoring of patients and staff motivation.15
Identifying factors that can predict non-responders or explain individual differences in long-term improvement is an important addition to the knowledge of how ICBT works in the treatment of SAD within a routine clinical context. Indeed, knowledge about predictors can be of high value to the clinician when making treatment recommendations. For example, the level of baseline illness severity has frequently been linked to higher post-treatment symptom levels after face-to-face CBT16 or after ICBT17 and less response to pharmacotherapy or face-to-face CBT.18 Further, both treatment credibility and adherence appear to be relatively stable predictors of greater short-term response to ICBT,19 ,19a but little is known about whether these factors can predict long-term effects as well. Finally, having a family history of social anxiety has been linked to lower probability of symptomatic improvement after ICBT.17 Investigating the long-term prognostic value of these factors would increase our understanding on how ICBT works in naturalistic settings for different subgroups of patients.
The main objective of this study was to evaluate the long-term effectiveness of ICBT for SAD in a cohort of consecutively recruited patients treated within routine psychiatric care. Long-term effects on quality of life and comorbid depressive symptoms were also studied. A secondary aim was to test the prognostic value of illness severity, adherence, treatment credibility and the influence of having a family history of social anxiety.
Methods
Participants
This was a longitudinal study investigating adult patients (N=446) who had a principal diagnosis of SAD and had been treated for SAD as part of routine care. In general, patients had to meet the following criteria at the time of inclusion: (1) fulfilling Diagnostic and Statistical Manual of Mental Disorders (DSM) IV criteria of social anxiety disorder, (2) agreeing not to undergo concurrent psychological treatments for the duration of ICBT, (3) having a stabilised dose of psychotropic medication for 4 weeks if on medication, (4) be ≥18 years old and (5) having access to a computer or other device with an internet connection. In general, exclusion from ICBT was based on the following criteria: (1) patients with severe depression (clinician rated Montgomery Åsberg Depression Rating Scale (MADRS) ≥35) and/or moderate to high risk of suicide where monitoring is required, (2) patients with low motivation, severe apathy or difficulty concentrating, (3) patients with psychosis, (4) patients with untreated drug or alcohol problems that may pose barriers to treatment, (5) reading and/or writing difficulties, including language difficulties, and (6) patients residing outside the city county.
Procedure and design
Treatment and data collection were performed within the context of a government-funded psychiatric clinic specialised in providing therapist-guided CBT using the internet as the mode of treatment delivery. As such, no conventional face-to-face treatments were offered. The treatment centre was part of the Karolinska University Hospital, managed by the Stockholm County Council, and operated as a conventional psychiatric outpatient clinic. The majority of those seeking treatment were self-referrals, but could also be referred by their general practitioner. In either case, all patients had to complete an online screening battery of self-report measures after which they were invited to the clinic to undergo a structured face-to-face diagnostic interview conducted by a psychiatrist or a resident physician. For those who were offered ICBT, treatment would typically be initiated within 48 h. The duration of the active psychotherapeutic intervention was 12 weeks, during which patients were guided online by licensed psychologists who had training in CBT. After treatment, patients were invited to the clinic for a post-treatment face-to-face follow-up visit; those who showed insufficient improvement could therefore be referred elsewhere for additional treatment.
The intervention was based on a manual developed by Andersson and colleagues with previously documented effects,6 ,20 and followed a protocol initially developed for individual therapy of SAD.21 When delivered as an internet-based intervention within the context of routine psychiatric care, it has been shown to be non-inferior to conventional CBT.13 The content of the treatment was accessible in the form of web-based text modules (similar to chapters in a self-help treatment manual) which were administered in a sequential manner. As therapists regularly provided feedback on homework associated with each module, they could monitor each patient's progress and provide individual support throughout treatment. In addition, there were weekly online self-assessments of both social anxiety and depressive symptoms.
Patients who had been discharged between October 2010 and June 2013 were informed of the study and invited to complete a long-term follow-up assessment battery online, which has previously been documented as a valid administration format.22 In total, the study comprised four measurement occasions: (1) pretreatment, (2) post-treatment, (3) 6-month follow-up and (4) long-term follow-up spanning a period of approximately 1–4 years after treatment. The study, including its consent procedure, was approved by the Regional Ethical Review Board in Stockholm, Sweden (no 2011/2091-31/3).
Outcome measures
Social anxiety
The self-report version of the Liebowitz Social Anxiety Disorder Scale—Self-Report (LSAS-SR)23 was used as the primary outcome measure. The LSAS-SR is a 24-item scale measuring both fear and avoidance in performance and social situations as separate subscales. The instrument has a high level of internal consistency (Cronbach's α=0.95) as well as a high 12-week test-retest reliability (r=0.83).23 ,24 At baseline, the LSAS-SR α for the present sample was 0.95. The LSAS-SR has shown strong convergent validity with other common self-report measures of social anxiety such as the Social Interaction Anxiety Scale and the Social Phobia Scale25 with correlation coefficients of 0.71 and 0.61, respectively.26 A cut-off score of 30 or less on the LSAS-SR has been suggested as indicative of probable absence from social anxiety disorder.27 Therefore, LSAS-SR ≤30 was used as a threshold value for calculating the remission rate throughout the study.
Comorbid depression
The Montgomery Åsberg Depression Rating Scale Self-Rated28 (MADRS-S) was used to assess change in depressive symptoms as a secondary outcome measure. MADRS-S measures nine clinical characteristics of depression with a total score range of 0–54. The test-retest reliability of MADRS-S has been shown to be high (r=0.80–0.94).28 Cronbach's α for the sample at baseline was 0.87. A cut-off score of 13 or higher has been used to distinguish depressed patients from non-depressed patients.29 The MADRS-S has been shown to have a high correlation with the commonly used Beck Depression Inventory (r=0.87).30
Potential prognostic variables
Baseline illness severity was rated by clinicians on a seven-point scale with the Clinical Global Impression—Severity Scale (CGI-S).33 A treatment credibility scale, originally proposed by Borkovec and Nau,34 assessed patients’ level of confidence in the treatment. This was operationalised as the total score (0–50) of five items (eg, ‘How much improvement do you expect from this treatment?’) measured on a continuous VAS from 0 to 10 (0=no improvement at all to 10=completely recovered/free from symptoms) after the first week of the treatment. Treatment adherence was defined as the number of modules that the patient had been able to work with during therapy as part of the treatment programme, and was therefore measured at post-treatment. Finally, having a family history of social anxiety was coded as a categorical variable during the diagnostic interview conducted by a clinician prior to treatment.
Adverse events
Data on adverse events were collected at follow-up in order to identify whether ICBT might have provided any short-term or long-term side effects. An adverse event was operationalised as any negative experience that a patient subjectively attributed to the ICBT intervention. Therefore, patients were asked to report these events as part of the online assessment battery, and were provided with an option to describe these in free text. Also, they were asked to rate the degree (on a four-point Likert scale) to which these adverse events affected their well-being (1) when they occurred and (2) to what degree they still affected their well-being.
Statistical analyses
Symptomatic change was analysed using longitudinal multilevel modelling. This approach has the benefit of taking into account the hierarchical nature of repeated measurements (ie, the dependency of observations of outcome scores clustered within each patient who provided repeated data). Two separate multilevel models were estimated: (1) a longitudinal growth model investigating the overall symptomatic change over time and (2) a longitudinal growth model investigating individual differences in the rate of change (ie, the effect of potential prognostic variables). In both models, a first-order autoregressive covariance structure for the repeated measurements level was used as recommended in longitudinal studies where correlations between measurements tend to weaken as time between them increases.35 Two approaches to treating time were considered; (1) either using a two-piece model with discrete time, grouping measurements into four measurement occasions (ie, pretreatment, post-treatment, 6-month follow-up and long-term follow-up) or (2) a model with a continuous time variable using the number of days to follow-up. Since grouping measurements facilitates the interpretation of the model, this approach was used. However, owing to the relatively wide distribution of duration to long-term follow-up assessment (ie, between 1 and 4 years), we tested whether those who completed the long-term follow-up at a short duration differed from those who completed the follow-up after a longer period in terms of the number of patients in remission at the time of follow-up. For this purpose, patients were categorised into two groups (‘short’ or ‘long’ duration), operationalised as either 1 SD below or above the mean duration, and analysed with a χ2 design. Further, since the aim of this study was to understand the sustainability of effects after completing treatment, a piecewise treatment of time was conducted. By using a piecewise growth model, two growth curves may be fitted in the same model, where each curve represents each developmental stage in the study (ie, treatment phase and follow-up phase). Piece 1 (T1) therefore constituted the phase between pretreatment and post-treatment, and piece 2 (T2) spanned the period between post-treatment, 6-month follow-up and long-term follow-up. For the T1 time variable, the four measurement occasions were coded as 0, 1, 1, 1, and for the T2 time variable, measurement occasions were coded as 0, 0, 1, 2. The benefit of this approach was the possibility to test whether there was a significant linear trend of continued improvement or worsening of symptoms after having completed treatment. The multilevel model testing the effect of outcome predictors included simultaneous entry of the following measurements: baseline CGI-S, level of adherence, treatment credibility and presence of family history of social anxiety. Consequently, the effect of each prognostic factor was estimated while controlling for the effects of the others. Predictor variables were standardised prior to analysis to facilitate comparison between effects measured on different scales. Within-group Cohen's d effect sizes for mean differences were calculated using estimated means and observed SDs and correlations between the repeated measurements.
Missing data analysis
Multilevel modelling provides several benefits in the treatment of missing data. As opposed to traditional complete case analyses where cases having incomplete data are deleted from the analysis, multilevel models incorporate all available data. Therefore, all patients who provided at least one outcome measurement were included in the analyses. All models were fitted using maximum likelihood estimation which calculates estimates of the statistical parameters most likely to have produced the observed data.36 In order to investigate any relationship between postmeasurements and missing data at long-term follow-up, an independent-samples t test was performed comparing mean post-treatment LSAS-SR among those who provided long-term follow-up data with those who were lost to long-term follow-up.
Results
Sample description
Patient characteristics are presented in table 1. The sample comprised 446 participants. Follow-up assessments were completed between 1.2 and 4.1 years from baseline (M=2.66, SD=0.80).
Description of the participants
Attrition and adherence
Of 446 patients who provided baseline measurements, 391 (88%) provided post-treatment data, 173 (39%) provided 6-month follow-up data and 321 (72%) provided long-term follow-up data on the main outcome measure. The mean level of treatment adherence was 8 (SD=3.35) of the 12 modules activated.
Remission
At post-treatment, 20.7% of patients who provided data had achieved remission from SAD, 34.1% at 6-month follow-up, and 35.2% at the time of long-term follow-up. The remission rate at long-term follow-up was found to be independent of when the follow-up assessment was completed; χ2 (1, N=141)=1.20, p=0.27. However, there was a significant difference in the proportion of patients in remission at follow-up depending on the use of psychotropic medication; χ2 (2, N=267)=12.41, p<0.01, indicating a moderate association (Cramer's V=0.22, p<0.02). Among those who reported no use of medication either during treatment or at the time of long-term follow-up, 41.8% (79 patients out of 189) had achieved remission, as opposed to 15.7% (8 out of 51) among those who reported using medication during treatment and at the time of long-term follow-up.
Multilevel models of long-term symptomatic improvement
Piecewise growth models that included a random intercept, a random linear slope for the treatment phase (piece 1) and a fixed linear slope for the post-treatment to the long-term follow-up phase (piece 2) were estimated for LSAS-SR, MADRS-S and EQ-5D. Change trajectories for these models are illustrated in figures 1⇓–3. Model-implied means and mean differences and observed SDs are presented together with associated effect sizes in table 2.
Estimated parameters from growth curve analysis of continuous outcomes

Improvement in social anxiety after internet-based cognitive–behavioural therapy for social anxiety disorder. Means are estimated from a linear piecewise multilevel growth model, depicted with 95% CIs. LSAS-SR, Liebowitz Social Anxiety Scale questionnaire Self-Report.
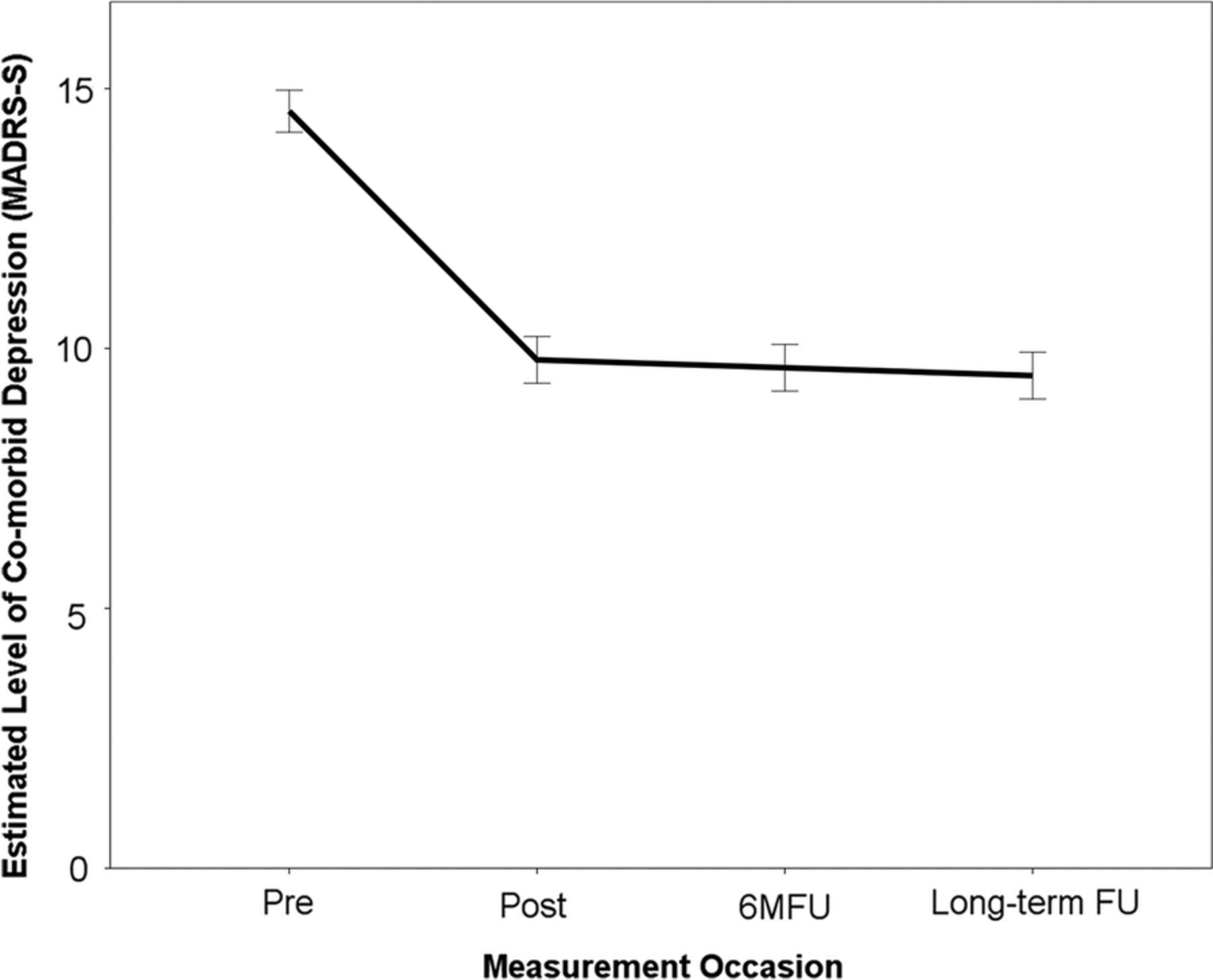
Improvement in comorbid depressive symptoms after internet-based cognitive–behavioural therapy for social anxiety disorder. Means are estimated from a linear piecewise multilevel growth model, depicted with 95% CIs. MADRS-S, Montgomery Åsberg Depression Rating Scale Self-report.

Improvement in health-related quality of life after internet-based cognitive–behavioural therapy for social anxiety disorder. Means are estimated from a linear piecewise multilevel growth model, depicted with 95% CIs. EQ-5D, Health-Related Quality of Life.
There was a significant effect of linear time on all three outcome measures between pretreatment and post-treatment (piece 1), reflecting large improvements in symptoms of social anxiety, moderate improvements in symptoms of depression and small improvements in health-related quality of life during the active treatment phase. After treatment (piece 2), continued long-term improvements (ie, a significant effect of time) in symptoms of social anxiety and quality of life were observed. Also, achieved improvements in symptoms of depression were maintained (ie, a non-significant effect of time).
Adverse effects
Of 281 patients who provided data on adverse effects, 22 (7.8%) subjects reported having experienced at least one adverse effect attributed to ICBT. However, 251 (89.3%) subjects responded that regardless of whether not they had experienced any adverse effect, these were in such cases minor and had no significant effect on them during treatment, and 263 (93.6%) reported that they experienced no significant adverse long-term effects. Nine (3.2%) subjects reported that adverse events attributed to the intervention had a very negative acute effect, and three (1.1%) reported that these also had very negative long-term effects. Common side effects described by subjects were experiencing feelings of inadequacy, guilt, stress, worry or failure of not adhering to the treatment schedule (sometimes triggered by receiving well intended reminders from therapists), anxiety associated with exposure assignments and also with an increased self-awareness of symptoms, negative cognitions and maladaptive behaviours.
Multilevel model explaining individual differences in the rate of symptomatic change
Estimates of model parameters predicting individual differences in the long-term rate of change in symptoms of social anxiety are presented in table 3 and illustrated in figures 4 and 5. A higher level of illness severity (ie, baseline CGI-S scores) was associated with a faster rate of improvement, whereas having a family history of social anxiety was related to a slower rate of improvement. When CGI-S scores and family history of social anxiety were controlled for, adherence and treatment credibility had no significant predictive value in explaining individual differences in the long-term rate of change.
Estimated parameters from growth curve analysis examining the long-term effects of adherence, treatment credibility, illness severity and family history on the rate of symptomatic improvement

Predicted long-term symptomatic change based on individual differences in illness severity. Predicted trajectory of social anxiety symptoms after internet-based cognitive–behavioural therapy for social anxiety disorder. For illustrative purposes, a categorisation was performed to depict predicted growth curves for patients scoring high and low on the Clinical Global Impression—Severity scale. High severity was operationalised as 1 SD above the mean CGI-S score and low credibility as 1 SD below the mean. Mean CGI-S was 3.79 (SD=0.83). LSAS-SR, Liebowitz Social Anxiety Disorder Scale—Self-Report; CGI-S; The Clinical Global Impression—Severity scale.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Predicted long-term symptomatic change based on individual differences in the family history of social anxiety. Predicted growth curves for patients reporting having a family history of social anxiety. LSAS-SR, Liebowitz Social Anxiety Disorder Scale—Self-Report.
Missing data analysis
To test any association between the level of social anxiety at post-treatment and missing data at long-term follow-up, an independent-samples t test was performed comparing mean post-treatment LSAS-SR scores among those who provided long-term follow-up data with those who were lost to follow-up. There was no difference in post-treatment LSAS-SR scores between patients who provided follow-up data (M=49.08, SD=23.68) and those who were lost to follow-up (M=52.64, SD=26.30); t(389)=−1.247, p=0.213. Also, there was no difference in pretreatment LSAS-SR scores between patients who provided follow-up data (M=69.07, SD=22.23) and those who were lost to follow-up (M=69.18, SD=25.99); t(444)=−0.046, p=0.964.
Discussion
Previous research on the clinical effectiveness of ICBT for SAD has demonstrated large short-term effects.12 ,13 The aim of the present study was to determine the sustainability of treatment effects in a naturalistic setting (ie, routine psychiatric care) and identify factors that might explain individual differences in the long-term rate of improvement. We are aware of only three long-term follow-up studies on ICBT for SAD, all of which were clinical trials. In these, large effect sizes were observed after treatment and sustained at 2.5-year follow-up,9 at 4-year follow-up11 and at 5-year follow-up.10 In line with these reports, we have observed similar results in this study within a naturalistic clinical context; a large treatment effect was achieved at post-treatment, and patients overall continued to improve in symptoms of social anxiety between 1 and 4 years after treatment. In addition, continued improvements in health-related quality of life were observed during the follow-up period.
A secondary aim of this study was to identify prognostic patient characteristics that moderate long-term treatment response. Expanding our knowledge about which patients are more likely to benefit from—or fail to respond to—ICBT might help further refine inclusion guidelines and modify treatment strategies to better suit different patient needs. Although adherence and treatment credibility have been associated with better outcome in previous research,19 we have found that these factors lack predictive value over longer follow-up time frames when severity of illness is controlled for. Evidence regarding the prognostic value of baseline illness severity is somewhat inconclusive. For example, one review37 on outcome predictors of conventional CBT for SAD found that although higher baseline severity predicted higher levels of severity after treatment, it was not related to the degree of improvement, whereas another review38 concluded that greater illness severity predicted a worse response. Consequently, our finding that illness severity is associated with a faster rate of symptomatic improvement is surprising. Nonetheless, this observation is a strong indicator that ICBT is also effective for patients who are severely ill, which may be contrary to common beliefs regarding internet-delivered therapies. We also identified family history of social anxiety as a predictor of poorer outcome. This relationship has been observed both in pharmacological treatment for SAD39 and in a randomised controlled trial on ICBT for SAD.17 Although family history has been shown to be associated with a twofold to threefold risk for developing SAD,40 it is unclear which mediating mechanisms of genetic and environmental factors might be responsible for the variance in treatment effects. Still, the identification of family history as a long-term outcome predictor may have implications for the need to monitor this patient group more carefully due to an increased risk of a lower response rate, and possibly also a higher level of therapist guidance during exposure training.
Finally, although we observed a difference in proportions of patients in remission from SAD at follow-up depending on the use of medication during and after treatment (41.8% of patients with no medication during or after ICBT had achieved remission at follow-up as opposed to only 15.7% among those who reported using medication during treatment and at the time of follow-up), these subgroups of patients may be difficult to compare because we do not know how they differ in terms of illness history.
There are some limitations of the study, the most apparent being the lack of a comparison group to control for spontaneous recovery. As this was a cohort study conducted within a naturalistic setting, this was an unavoidable limitation. However, available empirical data suggest a low probability of spontaneous recovery from SAD. For example, an 8-year study following the long-term course of SAD reported that only 13–14% had achieved remission after 1 year,41 which can be compared with 34.1% at 6-month follow-up in this study. Also, ICBT for SAD has demonstrated superiority to waiting-list controls.6 ,20 ,42–45 Taken together, it would seem unlikely that the observed improvements among patients in this study might be attributed to the effect of time alone. A second limitation concerns the operational definition of treatment adherence. This partly concerns defining adherence as the number of activated modules. Since participation and adherence in CBT typically refer to both in-session and out-of-session behaviour, homework assignments reflect a critical aspect of the treatment package. Therefore, since each new module was activated only after completion of the previous one, it is possible that many patients did not fully complete the homework assignment related to their last module. However, although the degree of completion of the last activated module is unclear, we still know how many modules each patient worked with at a minimum (ie, all until the last activated module). Consequently, for some patients (those who did not complete the last module they had access to), the level of adherence may be overrated by 1. On the other hand, a more serious potential risk of measurement error in regard to measuring adherence is the lack of information regarding how closely the number of modules correlates with actual therapeutic activity. Third, a note on the statistical approach of handling the relatively wide time frame of the long-term follow-up ‘time point’ is warranted, since these de facto ranges cover a period of several years. As described in the Methods section, there were mainly two alternative approaches to model how the outcome variables evolve over time. We could treat time as either discrete or continuous. Within a discrete framework, time values are defined as distinct time periods or measurement occasions; in this study, pretreatment, post-treatment, 6-month follow-up and long-term follow-up measurements were categorised into four separate assessment occasions irrespective of the actual duration since baseline. The alternative approach, treating time as continuous, would have meant that the time variable would range over the complete duration of the study (ie, 1492 days). We acknowledge that there are benefits with both approaches. For example, it could be argued that developing a model using a continuous time variable might be more exact and mathematically tractable. On the other hand, it might be easier to understand and interpret a model that corresponds to how the theoretical hypothesis to be tested is expressed (eg, to understand the degree of symptomatic improvement at long-term follow-up). Ultimately, we chose a discrete time framework in order to facilitate the development and interpretation of the multilevel model.
In sum, this study demonstrates that ICBT for the treatment of SAD in regular clinical practice is effective not only in the short term but also in the long term. Patients also reported significant reductions in comorbid depressive symptoms and improved quality of life. Furthermore, higher severity of illness was related to a greater rate of symptomatic improvement, whereas having a family history of social anxiety was associated with worse response. Considering that SAD is one of the most common anxiety disorders, and that access to CBT is rather limited, ICBT could significantly increase the availability of evidence-based effective treatments for a large patient group.
References
Footnotes
Funding This study was supported by research grants from the Stockholm County Council (grant number ALF 20130413).
Competing interests None declared.
Ethics approval Regional Ethical Review Board in Stockholm, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Study data are stored at the repository of Karolinska Institutet. Data are not freely accessible, but each request is assessed by Karolinska Institutet, and approval of data access can be given after this assessment. To request data, please contact Karolinska institutet by e-mail at info@ki.se or at Karolinska Institutet, SE-171 77, Stockholm, Sweden.