Article Text

Abstract
Objectives To identify adverse drug reactions associated with lamotrigine in children and compare the safety profile with other antiepileptic drugs.
Setting Databases EMBASE (1974–April 2015), MEDLINE (1946–April 2015), PubMed and the Cochrane library for randomised controlled trials were searched for studies on safety of lamotrigine.
Participants All studies involving paediatric patients aged ≤18 years who have received at least a single dose of lamotrigine with safety as an outcome measure were included.
Primary and secondary outcome measures The primary outcome measure was safety of lamotrigine. Drug interaction of lamotrigine was the secondary outcome.
Results A total of 78 articles involving 3783 paediatric patients were identified. There were 2222 adverse events (AEs) reported. Rash was the most commonly reported AE, occurring in 7.3% of the patients. Stevens-Johnson syndrome was rarely reported, with a risk of 0.09 per 100 patients. Discontinuation due to an adverse drug reaction (ADR) was recorded in 72 children (1.9% of all treated patients). Fifty-eight per cent of treatment discontinuation was attributed to different forms of rash and 21% due to increased seizures. Children on lamotrigine monotherapy had lower incidences of AEs. Headache (p=0.02), somnolence (<0.001), nausea (p=0.01), vomiting (p<0.001), dizziness (p<0.001) and abdominal pain (p=0.01) were significantly lower among children on monotherapy.
Conclusions Rash was the most common ADR of lamotrigine and the most common reason for treatment discontinuation. Children receiving polytherapy have a higher risk of AEs than monotherapy users.
Trial registration number CRD42013006910.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This systematic review assessed the quality of all the prospective studies.
Randomised controlled trials (RCTs), cohort studies and case reports were reviewed.
Only a limited number of RCTs of lamotrigine in children have been published, thus limiting the power of the meta-analysis.
The risks of adverse reactions between monotherapy and polytherapy users were compared in RCTs alone because only one prospective cohort study involving children receiving lamotrigine monotherapy was identified.
Background
Lamotrigine (LTG) was first synthesised in the early 1980s. It was approved for adult use in Ireland in 1990, the UK in 1991, and by the US Food and Drug Administration (FDA) in 1994.1 Since its market authorisation over two decades ago, it has been used increasingly for the treatment of paediatric epilepsy. It is the most commonly prescribed new generation antiepileptic drug (AED), accounting for 65% of new AED prescriptions in the UK2 and 12% of all AED prescriptions for children in the Netherlands.3
In the UK, LTG is recommended as monotherapy as the first-line treatment for newly diagnosed focal seizures and as an adjunct for refractory focal seizures in children.4 It is a second-line monotherapy drug for new onset generalised seizures and a useful adjunct for refractory generalised seizures. It is the third drug of choice, after ethosuximide and valproate, for absence seizures and it may be administered as a monotherapy or polytherapy.4
Dosing of LTG in children on adjunctive therapy is dependent on the effect of the coadministered drug. Higher doses may be required when coadministered with AEDs, such as phenobarbital, phenytoin, carbamazepine and oxcarbazepine, which have been shown to increase the drug's clearance and reduce its plasma concentration. Conversely, valproic acid reduces LTG clearance and raises its plasma concentration by as much as twofold; hence, a lower dose is recommended.5
A safety concern with LTG in children is the occurrence of a skin rash. This can vary in intensity, from transient mild rash to Stevens-Johnson's syndrome (SJS), which can be fatal.6 Children are generally more predisposed to skin rashes than adults.7 Most of the other known adverse reactions are neurological and are largely dose dependent.7 LTG can worsen myoclonic seizures and is usually avoided in patients with severe myoclonic epilepsy of infancy (Dravet syndrome).8
This systematic review was performed to identify all studies of LTG safety in children, to determine the adverse reactions of LTG and to compare the safety of the drug with other AEDs.
Methods
Search strategy
Databases EMBASE (1974–April 2015), MEDLINE (1946–April 2015), PubMed and the Cochrane database of randomised controlled trials (RCTs) were searched for original research or reports in which paediatric patients received at least a single dose of LTG with safety as an outcome measure. ‘Paediatrics’ was defined as any patient ≤18 years old. All studies satisfying these criteria were included irrespective of the language of publication. A search combining Lamotrigine with pediatric* or paediatric* or child* or neonate* or neonat* or infan* or newborn or adolescent* or boy* or girl* or toddler for the multipurpose search was carried out. All included articles were independently evaluated by two reviewers. Study was conducted in compliance with the PRISMA guidelines and registered on PROSPERO (Number: CRD42013006910 available from: http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42013006910)
Data extraction
Data extracted from each study included: year of study, setting, age of patients, study design, number of patients receiving LTG and comparator, dose, type of seizure, study outcome, summary of result, type of therapy, number of withdrawals and reason for withdrawal, and the number and type of adverse events (AEs) for both LTG and the comparator drug(s).
Data quality assessment
The RCTs were assessed for quality using the Cochrane collaboration's tool for assessing risk of bias in randomised trials.9 Observational studies were assessed using the System for the Unified Management of the Review and Assessment of Information (SUMARI).10 This form comprises of nine appraisal criteria and any study that met more than four of these criteria was considered to be of a sufficiently good quality. All studies were independently assessed by two reviewers; a third blinded reviewer was involved only if both reviewers did not agree on any study.
Data collection and statistical analysis
All relevant data were extracted onto an Excel spread sheet. χ2 Analysis was used to compare categorical data. The RCTs were aggregated and meta-analyses were conducted using Revman V.5. The relative risks (RRs) of AEs present in at least two RCTs were calculated. An RR greater than one indicates a positive effect of LTG. After testing for homogeneity (I2 ≤50% or χ2 p≥0.05), the fixed effect model was used for homogeneous data and random model for heterogeneous data.
Results
Summary of studies
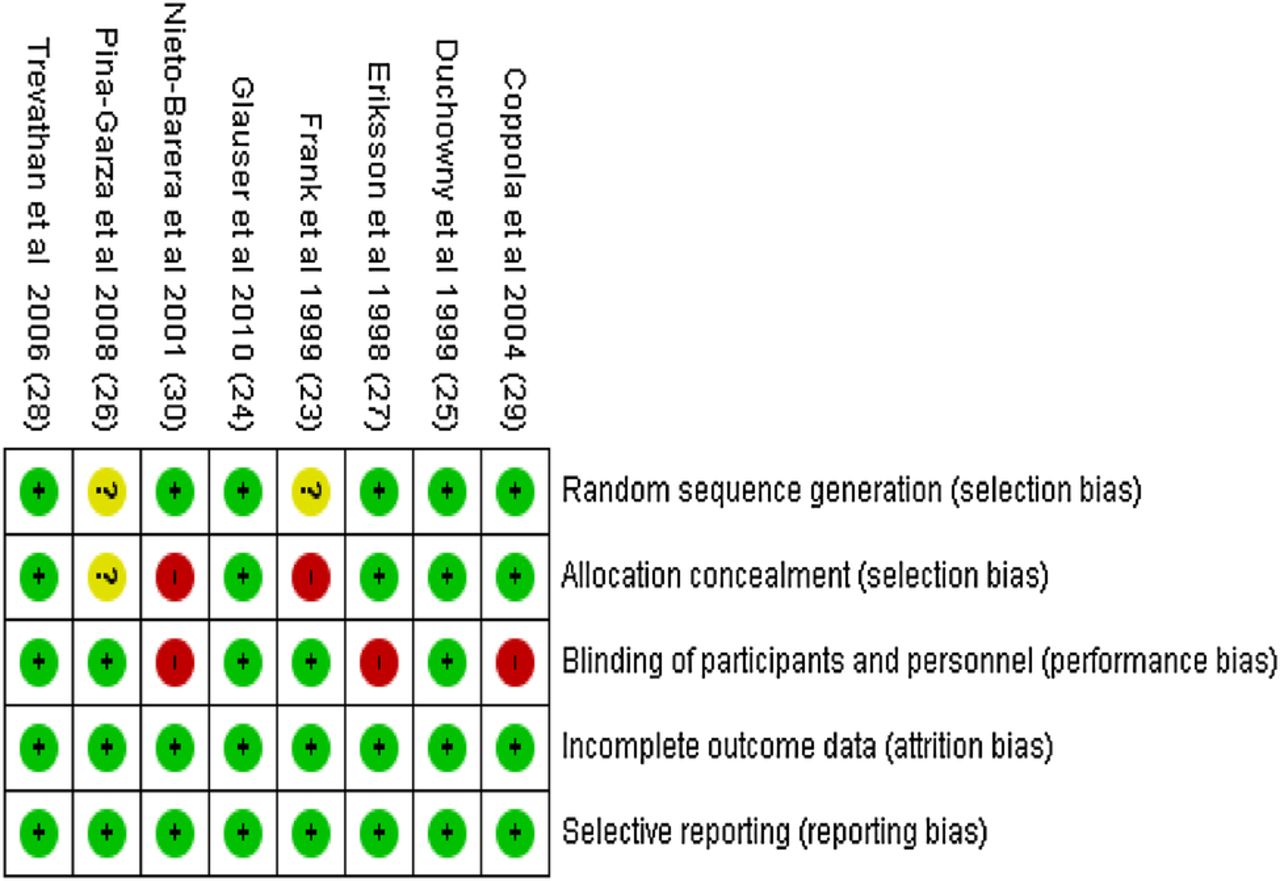
A total of 78 articles with reports on safety of lamotrigine were identified after the literature search (figure 1). A total of 3783 paediatric patients were administered LTG. The most common types of articles were case reports (table 1). The largest number of patients were in cohort studies (3012, 80%). There were 17 cohort studies and 9 RCTs. There were 50 case reports involving 53 children. All RCTs were of sufficiently good quality and eligible for meta-analyses (figure 2). All cohort studies were considered to be of good quality and were included in the final data aggregation (see online supplementary table S1).
Summary of all articles

Flow chart for screened articles.

Risk of Bias summary for randomised controlled trials.
Safety results
There were 2222 documented AEs in 3783 children in the reviewed articles. The majority (1524) of the AEs were reported in 12 prospective cohort studies11–22(see online supplementary table S2). There were 549 AEs reported from RCTs.23–31
Prospective studies
Common adverse events (≥1/100 and <1/10) from pooled prospective studies (RCTs and cohorts) were: rash, headache, fever, somnolence, vomiting, seizure aggravation, dizziness, cough, aggression, ataxia and insomnia. Uncommon AEs (≥1/1000 and <1/100) were: behavioural disturbance, nausea and anorexia (table 2). About one-third of all AEs (35.8%) were neurological events, while gastrointestinal and respiratory events were 14.8% and 13.9% of all AEs, respectively.
Risk of all adverse events from pooled prospective cohort studies and RCTs according to body system (number of children=3417)
Rash was the most common AE in children receiving LTG. From all prospective studies, the risk of rash was 7.3 per 100 patients (table 2). It accounted for 13% of all AEs. It was also the most common reason for withdrawal of therapy, with 58% of treatment discontinuation attributed to different forms of rash (table 3). SJS was rarely reported, with a risk of 0.09 per 100 patients. All cases of SJS resulted in treatment discontinuation. The RR of rash with LTG compared with placebo from two RCTs, involving 112 patients on LTG, was 3.66 (95% CI 0.11 to 123.11), which was not statistically significant (p=0.47). Seventy-two children had deterioration in seizure control and the risk of aggravated seizures was 2.14 per 100 patients (table 2).
Adverse reactions leading to discontinuation of treatment
There were significantly higher risks of dizziness (RR 4.57, 95% CI 1.88 to 11.12, p<0.001), abdominal pain (RR 2.53, 95% CI 1.12 to 5.70, p=0.03) and nausea (RR 5.94, 95% CI 1.59 to 22.13, p=0.008) with LTG than placebo in the RCTs. Twenty-one per cent of children receiving LTG had dizziness compared with 4.5% on placebo. Sixteen percent and 12.5% of LTG treated children had abdominal pain and nausea, respectively, compared with 6% and 1.7% of placebo-treated children. The RRs of other common AEs from RCTs identified were not significantly different between LTG and placebo-treated children (figures 3 and 4).

Relative risks of adverse events between lamotrigine and placebo.

Relative risks of adverse events between lamotrigine and placebo.
When compared with valproic acid, the risk of somnolence and vomiting were significantly lower for LTG (RR 0.35, 95% CI 0.13 to 0.89, p=0.04) and (RR 0.20, 95% CI 0.04 to 0.89, p=0.03), respectively. Three percent and 1.3% of children on LTG had somnolence and vomiting, respectively, while these symptoms were recorded in 9.5% and 6.8% of those on valproic acid. The risk of other common adverse events, such as rash, dizziness, headache and seizure aggravation, were not significantly different (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relative risks of adverse events between lamotrigine and valproic acid.
Discontinuation of LTG treatment due to adverse drug reactions (ADRs) was recorded in 72 children (1.9% of all treated patients). Rash (58%) and seizure aggravation (21%) were the most common reasons for discontinuation (table 3).
Case reports
There were more case reports of rash than any other AE, accounting for about half (49%) of all reports (see online supplementary table S3). Rash varied in severity from mild morbilliform rash to toxic epidermal necrolysis (TEN). Other variants were urticarial, SJS and Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS syndrome). The period of onset of rash after start of LTG treatment varied between 1 day and 103 weeks, with the median duration of onset of 25 days (IQR: 14–35 days). In half (48%) of the cases of rash, LTG was coadministered with valproic acid There were seven case reports of seizure aggravation (see online supplementary table S3). Other adverse reactions reported were: movement disorders, disseminated intravascular coagulopathy, parageusia and syndrome of inappropriate antidiuretic hormone secretion.
Effect of dosing and polytherapy on ADRs
LTG doses were titrated over several weeks until the maximum maintenance dose was achieved. Patients receiving LTG monotherapy received an almost similar median initial dose (median 0.5 mg/kg (1QR 0.4–1.1)) as those receiving combination treatment with valproic acid (median 0.5 mg/kg, (IQR 0.15–0.75)). Patients treated with combination therapy of enzyme-inducing drugs received a higher median dose of initial LTG (1 mg/kg (IQR 0.6–2)). Children on mixed AED regimen, excluding valproic acid, received a higher median maintenance dose of LTG (median=15 mg/kg (15–15.1)) than those on monotherapy (median 11 mg/kg (IQR 10–14.4)) and valproic acid combination (5 mg/kg (IQR 5–5.1)).
LTG was given as part of a polytherapy regimen in five RCTs. The most frequent reports of rash (16%) were in a study with a high initial LTG starting dose of 0.5 mg/kg/day in VPA comedicated patients and 2 mg/kg/day in those receiving enzyme-inducing AEDs. The dose escalation to reach maintenance doses of 1–3 and 5–15 mg/kg/day respectively, was achieved in 6 weeks.25 Three other polytherapy studies26–28 introduced LTG treatment at much lower doses (0.15–0.2 mg/kg in VPA comedicated patients and 0.6–1 mg/kg/day in those receiving enzyme-inducing drugs). The rates of dose escalation were much slower (12–19 weeks). Of these three studies, only one reported a single case of rash (5%),26 while the other two did not record any rash. A fifth study administered 0.2 mg/kg/day initial dose to VPA comedicated patients and 2 mg/kg/day to those on enzyme-inducing AEDs. This study recorded a 6% rash rate.31
There were four RCTs in which LTG was administered as monotherapy.23 ,24 ,29 ,30 The initial dose in one study was 0.3 mg/kg/day (24), dose escalation was slow (up to 16 weeks) and a 3% incidence of rash was reported. The three other studies administered 0.5 mg/kg/day as initial doses.23 ,29 ,30 Two of these each reported a rash incidence rate of 7%,23 ,30 while one of these escalated the dose rapidly over 6 weeks.30 The third study reported a 5% rash incidence rate.29
All but one of the prospective cohort studies used LTG polytherapy. Comparison of the incidence rates of ADRs between RCTs involving children who received LTG monotherapy or polytherapy showed that monotherapy users had significantly lower rates of AEs than polytherapy users (table 4). The incidence rates of dizziness, somnolence, headache, vomiting, nausea and abdominal pain were all significantly lower in patients on LTG monotherapy than polytherapy. There was also a trend towards a decreased incidence of rash in patients on LTG monotherapy, although this was not statistically significant (p=0.09).
Incidence rates of AEs in monotherapy and polytherapy LTG users in RCTs
Discussion
Rash was the most common AE in children receiving LTG treatment. The risk of rash was 7.3 episodes per 100 children. It also accounted for 10% of all AEs. Other commonly reported AEs were neurological symptoms, mainly somnolence, headache, aggravated seizures, dizziness, as well as vomiting. A previous safety review of 13 manufacturer sponsored clinical trials involving 1096 children had also shown a similar result.32
Children are more likely than adults to develop a rash with lamotrigine.33 Simple maculopapular rashes were the most common types of rash identified in this review. These were usually transient and often without long-term complications. LTG associated rashes are usually highly variable and the most severe forms are SJS and TEN. TEN is the more severe of these two, with an average background mortality rate of 25–35% compared to 1–5% in patients with SJS.34 Patients with TEN are also more likely to have long-term complications, with up to 50% of them reported to have long-term problems.34 Despite rash being the most common ADR with LTG, there were no statistically significant differences between LTG and either placebo or valproic acid in relation to the occurrence of rash in the RCTs reviewed. Only two RCTs compared the risks of rash between LTG and placebo or valproic acid, but these studies were insufficiently powered to adequately compare the risk of rash.
Rapid dose escalation and high initial doses have been reported to be predisposed to rash manifestation.7 According to the current recommendations in the UK and USA, an initial dose of 0.15 mg/kg/day should be given to valproate (VPA) comedicated children, 0.3 mg/kg/day to those receiving enzyme-inducing AEDs and monotherapy.35 ,36 The protective mechanism of the introduction of small incremental doses, although not fully understood, is believed to involve the desensitisation of antigen presenting cells and T lymphocytes.37 Human leucocyte antigen (HLA) B genotyping may be useful in determining the predisposition to LTG-induced rash, but the level of HLA involvement is not fully determined.38 Comedication with valproic acid is also a significant predictor of rash in LTG-treated patients.33 Half of the case reports of rash identified in this review occurred when LTG was concomitantly administered with valproic acid. Valproic acid is a glucuronide inhibitor which increases the half-life of LTG and decreases its clearance.39 Owing to this inhibitory effect, LTG starting and maintenance doses are recommended to be lower during concurrent valproic acid therapy.
Neurological effects are the most common ADRs of AEDs.40 Somnolence, headache and dizziness were frequently reported among patients in this review. A previous study had identified somnolence as the most common ADR in patients receiving LTG as add-on treatment, while a much lower incidence was reported in monotherapy users.32 A similar pattern has been shown in this study, with a significantly lower incidence of somnolence (p<0.001) reported in patients on monotherapy. Comparative safety analysis of RCTs in this review, however, shows that patients receiving LTG had significantly lower risk of somnolence than those treated with valproic acid. The small number of studies included in the meta-analyses necessitates a cautious interpretation of this result.
About 2% of patients had an increase in seizures. Additionally, increased seizures was the second most common reason for discontinuing LTG. Seizure aggravation is a recognised problem in patients with epilepsy receiving LTG; the cause and mechanisms of these paradoxical drug-induced seizures are unknown. New seizures may not be easily traced to antiepileptic drugs since there is usually an inherently high variability in seizure frequency in patients with epilepsy.41 It is thought to be most common in children with myoclonic epilepsy.8
For most of the ADRs, children on polytherapy had significantly higher incidence of ADRs than those on monotherapy (table 4). We have only compared ADRs in RCTs because only one prospective monotherapy cohort study was identified. In addition to the potential interactions between the drugs, the addition of one or more AED also adds to the chances of more ADRs. The relationship between polytherapy and increased ADRs has been established in a previous study of AEDs.42 Polytherapy with valproic acid has also been shown to be associated with a greater risk of hepatotoxicity, pancreatitis and other serious ADRs.43
A limitation of this study is that only one reviewer searched and selected the included articles. However, the quality of all the included articles was independently assessed by two reviewers. The relationship between rash and age could not be established because most of the studies did not report the ages of children with rash.
In conclusion, rash, which occurred in a spectrum of varying intensity, was the most common ADR associated with LTG; it was also the most common reason for the discontinuation of treatment. High initial LTG dose and rapid dose escalation are risk factors for rash. Patients on LTG polytherapy are more likely to develop ADRs than monotherapy users.
Acknowledgments
The authors would like to thank Janine Cherrill for assisting with the quality assessment of the articles.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors OE, HMS and IC conceived the idea as part of OE's PhD. OE did the literature search and extracted the data. HMS and IC reviewed the extracted data. OE wrote the first draft, and IC and HMS edited the draft and subsequent drafts. OE wrote the final draft. OE, HMS and IC agreed to the final draft.
Funding This work is part of OE's PhD, funded by the Commonwealth Scholarship Commission.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.